Lung cancer is one of the most common cancer and leading cause of cancer mortality worldwide. It accounts for 12.9% of all new cancers and one out of five cancer deaths are due to lung cancer. Of the estimated 1.8 million new cases in 2012 (12.9% of the total), 58% occurred in less developed regions [1]. Lung cancer remains the commonest cancer among males worldwide [1]. In India, lung cancer constitutes 9.3% of all cancers [2]. Lung cancer incidence and mortality is rising in females and declining in males in developed nations. The observed variations in lung cancer rates and trends across countries or between males and females within each country largely reflect differences in the stage and degree of the tobacco epidemic [3]. Tobacco smoking is the leading cause of lung cancer accounting for about 90% of cases [4]. Adenocarcinoma, squamous cell carcinoma, large cell carcinoma and small cell undifferentiated carcinoma are the common histological types accounting for more than 90% of all lung cancers [4]. The advent of personalized chemotherapy based on histology and molecular expression and relative increase in adenocarcinoma worldwide has generated a renewed interest in epidemiology of lung cancer [4,5]. Therefore, understanding the burden of lung cancer according to histological type is not only of epidemiological interest but also crucial for treatment decision. Developed nations have witnessed a shift in lung cancer histology and adenocarcinoma has surpassed the squamous cell type to become the most common type of lung cancer [4]. The overall incidence of lung cancer is on the rise in India [6]; however, a trend of histological shift is not observed uniformly across the country [7-14]. Therefore, the study aimed to understand the current epidemiological trend of lung cancer in patients presenting to authors’ institute in Southern India. The authors’ institute {Jawaharlal Institute of Post-graduate Medical Education and Research (JIPMER)} is an apex government health care institution located in the union territory of Puducherry, South India and caters to health need of population in several adjacent South Indian states.
Materials and Methods
This was a hospital based prospective cross-sectional study conducted between January 2011 to December 2012 in the department of Pulmonary Medicine, JIPMER, Puducherry, South India. A total of 125 patients diagnosed with a cytological or histological confirmation of lung cancer were included. Patients with clinico-radiological suspicion of lung cancer but no cytological or histological confirmation were excluded. The study was approved by the institute ethics committee and written informed consent was obtained from the participants. Patient’s demographic data (age, sex, and residence), smoking status, clinical presentation, radiological findings, histological type and stage of cancer were prospectively collected. For analysis, patients were classified as non-smokers, if they denied of smoking ever and smokers that included both current and former smokers. Staging of NSCLC was done as per 7th edition of the TNM classification based on Tumour size and extension (T), lymph Nodal involvement (N), and presence of distant metastasis (M) [15]. SCLC was staged as either limited (disease confined to one hemithorax with or without regional lymph node metastases and/or ipsilateral pleural effusion) or extensive disease [16]. The WHO classification of lung tumours was followed for classifying different histo-morphology of lung cancer [17]. Immunohistochemistry was performed using immunostaining such as thyroid transcription factor -1, p40, p63, synaptophysin and chromogranin to identify specific histology of lung cancer [18]. Quantitative data were presented as mean with Standard Deviation (SD) whereas categorical data were expressed as percentages. Association between smoking, sex and histopathology was calculated by Chi-Square test. Odds Ratio (OR) with 95% confidence interval was calculated and p-value ≤ 0.05 was considered significant. Data was analysed in SPSS version 21.0.
Results
The demographic details of the study population are summarized in [Table/Fig-1]. A total of 125 {115 (92%) NSCLC, 10 (8%) SCLC} lung cancer patients were included during the study period. Mean age of presentation was 55±9.62 years. Seven (5.6%) patients were ≤40 years. Majority of patients were male (95 patients, 76%) with a male to female ratio 3.1:1. Overall, 71 patients (56.8%) were smokers and all were males. Cough was the commonest symptom found in 110 (88%) patients, followed by dyspnea 92 (73.6%) patient and chest pain in 63 (50.4%) patients. Adenocarcinoma [Table/Fig-2 A,B] was the most common type of lung cancer seen in 67(53.6%) patients followed by squamous 39 (31.2%), small cell carcinoma 10(8%), [Table/Fig-3A, B], undifferentiated carcinoma 7(5.6%) and large cell carcinoma in 2 (1.6%) patients. Majority of NSCLC patients (104) presented with advanced disease {stage IV disease 70 (61%), stage IIIb 20 patients (17.4%), Stage IIIa 14 (12.2%) Stage IIb 7 patients (5.2%), Stage IIa 4 patients (3.5%)}. Nine patients (90%) of SCLC had extensive disease and 90% (9 patients) were smoker. Most non-smokers (38 patients, 73%) had adenocarcinoma whereas equal proportions (29 patients, 41%) of smoker had squamous cell and adenocarcinoma each. Males were five times more likely to have squamous cell carcinoma than females (OR = 5.54, CI 1.76-17.44). Smokers were 3.8 times more likely to have squamous histology than non-smokers (OR =3.8, CI 1.6-9).
Demographical comparison of lung cancer between smokers and non-smokers.
| Overall | Smoker | Non-smoker | p-value |
|---|
| (n=125) | (n=71) | (n=54) |
|---|
| Age (years)* | 55(9.62) | 56.3(7.41) | 54.39(7.37) | |
| (Mean±standard deviation) |
| Male number, (%) | 95(76) | 71(75) | 24(25) | |
| Histology - number (%) | | 0 .022 |
| Adenocarcinoma | 67(53.6) | 29(41) | 38 (73) | |
| Squamous cell | 39(31.2) | 29(41) | 10(19) | |
| NSCLC Undiff | 7(5.6) | 4(5.6) | 3(5.7) | |
| Large cell | 2(1.6) | 1(1.1) | 1(1.9) | |
| Small cell | 10(8) | 9(12.5) | 1(2) | |
| NSCLC stage – number (%) | 0.725 |
| IIa | 4(3.5) | 3(4.8) | 1(1.9) | |
| IIb | 7(5.2) | 4 (6.4) | 3(5.8) | |
| IIIa | 14(12.2) | 9(14.3) | 5(9.6) | |
| IIIb | 20(17.4) | 13(20.6) | 7(13.5) | |
| IV | 70(61) | 34(54) | 36(69) | |
| SCLC stage – number (%) | 0.239 |
| Limited disease | 1(10) | 1(11) | 0(0) | |
| Extensive disease | 9(90) | 8(89) | 1(100) | |
NSCLC – Non Small Cell Lung Cancer, NSCLC Undiff – Non Small Cell Lung Cancer undifferentiated, SCLC – Small Cell Lung Cancer
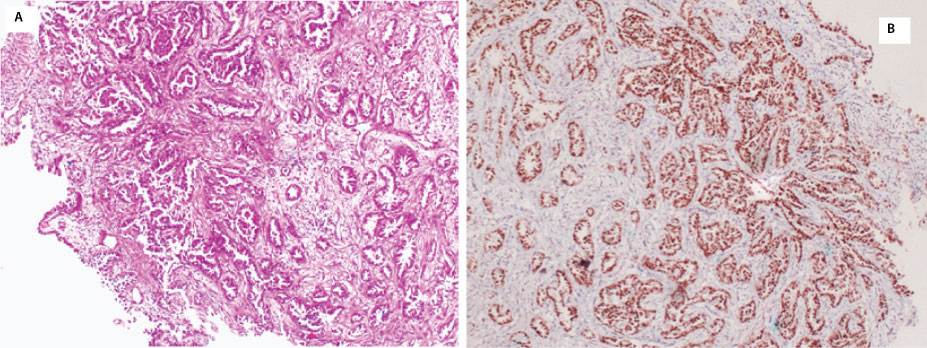
Section shows endobronchial mucosa with the epithelium showing features of adenocarcinoma (H&E 100X). Tumour cells are strongly immunopositive for TTF-1 indicating adenocarcinoma of lung (nuclear) (IHC X100)
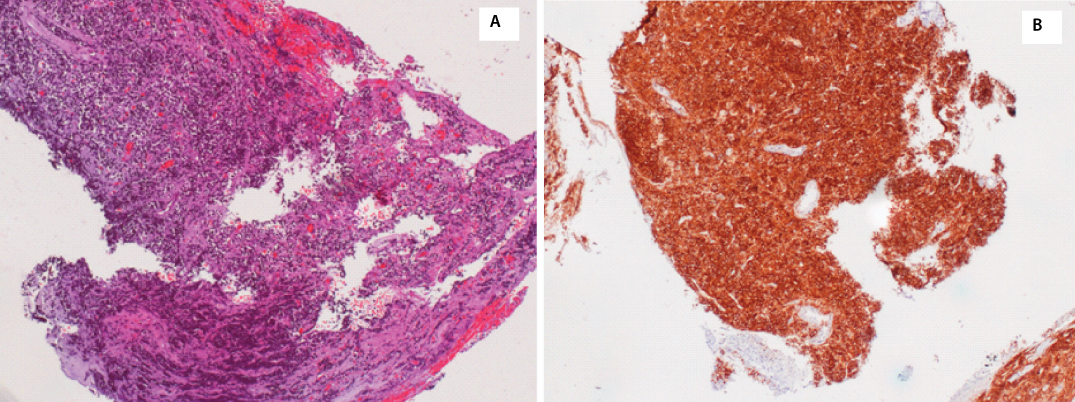
Fragments of endobronchial mucosa showing round, dark, hyperchromatic cells with scant cytoplasm in cords and nests favouring small cell lung cancer (H&E x100). Tumour cells are diffusely positive for synaptophysin (cytoplasmic) indicative of small cell carcinoma of lung (IHC X100).
Discussion
Adenocarcinoma was found to be the commonest type of lung cancer in our patients with a trend of diminishing male-female ratio. Disappointingly, most patients presented in advanced stage (Stage IV & IIIB) precluding curative treatment. Majority of non-smokers as well as significant proportions (41%) of smokers had adenocarcinoma. Smoking and male sex was strongly associated with development of squamous histology.
According to a recent report that analysed Surveillance, Epidemiology, and End Results (SEER) program data to investigate recent lung cancer incidence according to histologic types, found that overall there is a gradual decline of lung cancer incidence in the United States. Squamous and small cell carcinoma rates declined since the 1990s in both sexes. Adenocarcinoma rates showed a decreasing trend among males until 2005, after which a rise in incidence was seen among both sexes of all racial/ethnic groups between 2006 to 2010. Noteworthy is the recent upsurge of adenocarcinoma rates among young females, among all racial/ethnic groups in United States [19].
All histological types of lung cancer are associated with smoking with the association strongest for squamous and small cell carcinoma and modest for adenocarcinoma. Several factors related to smoking like number of cigarettes per day, duration of smoking, type and composition of cigarettes, degree of inhalation, and years of smoking cessation influence lung cancer risk and possibly determine the histology type. Present rise in adenocarcinoma rates in developed nations has been correlated with the increase in use of filtered cigarettes that encouraged deep smoke inhalation resulting in greater deposition of carcinogens in peripheral lung [4,19]. Furthermore, the risk of lung cancer declines more rapidly for squamous cell carcinomas and less rapidly for adenocarcinomas following smoking cessation partly explaining the relative excess of adenocarcinoma in recent years [19]. In addition, improvisation in cancer diagnostics with increasing use of immunohistochemistry during the last decade play a key role in identifying accurate histology of lung cancer and coincides with the precipitous drop in rates for unspecified carcinomas [19].
Previous studies in India during 1962-2001 reported squamous cell carcinoma as the commonest type with its prevalence varying from 26% to 73% and that of adenocarcinoma 3.9% to 34% [6]. However, many of these studies reported a surprisingly high percentage of tumours as “unclassified” histology potentially underestimating the true prevalence of different histological types of lung cancer [6]. A previous study from the authors’ institute reported only 100 cases of pathologically confirmed lung cancer over 8 years (1981-1988) period with squamous type as the most common histology (27%) followed by adenocarcinoma (21%); however, 33% were classified as undifferentiated carcinoma that could underestimate the true burden of different histological types [8]. 125 cases of lung cancer were detected over two years with adenocarcinoma emerging as the most common type. This suggests not only a possible rise of lung cancers but also a histological shift favouring adenocarcinoma in the study population. Two recent publications from Chennai, a city geographically close and socio-culturally similar to authors’ place, reported adenocarcinoma as the most common primary lung cancer in 55% and 42.6% of patients respectively [18,20]. This indicates a possible histological shift of lung cancer in recent time in Southern India. However, such a shift in lung cancer histology is not observed in North, Eastern and North-eastern India where squamous cell carcinoma continues to be the predominant lung cancer [11-14]. These geographical differences may be attributed to variations in smoking prevalence and overall smoking behaviour in the study population. According to the population-based cancer registry report 2009-11, lung cancer remains the leading cancer among males in Bangalore, Chennai, Delhi, Kolkata, Tripura, Kollam and Thiruvananthapuram and among females in Manipur and Mizoram [21]. As per the consolidated report of hospital-based cancer registries 2007-2011 based on histologic types in India, adenocarcinoma was the commonest lung cancer among males in Mumbai, Chennai, Thiruvananthapuram and Guwahati after exclusion of the category ‘Neoplasm malignant’ and among females in most centres [22]. In the present study, the proportions of smokers and male to female ratio were similar to studies reporting adenocarcinoma as most common histology [18,20], and lesser compared to studies reporting squamous histology as commonest lung cancer [11-14]. Comparative demographics of lung cancer patients in India pre- and post-1985 shows a declining trend of male-female ratio (6.67:1 vs 5.76:1) with a rise of adenocarcinoma cases in both sexes and a substantial drop in the histological types classified as “Others” during the later phase (1986-2001), suggesting an improvisation in specific histological diagnosis of lung cancer in recent years [6].
Limitation
Being a single-centre hospital-based study; it is acknowledged that the findings may not be a true reflection of lung cancer epidemiology in the population. However, most epidemiological data on lung cancer in India are based on hospital-based studies. Furthermore, hospital records are integral data source for population-based cancer registry. Population-based cancer registry provides a fairly accurate estimate of overall cancer incidence and prevalence in a population whereas hospital-based registries are more reliable source of estimation of lung cancer burden according to histological types because data sources that contribute to population-based registry such as municipality, insurance companies and general practitioners are unlikely to record specific histology of lung cancer. Therefore, the present study findings may be a close reflection of the prevailing lung cancer histology patterns in the reference population. Secondly, the smoking details were not analyzed separately in this study. Therefore, further studies should be conducted in the reference population to look for the association between the smoking behavior and type of lung cancer.
Conclusion
To conclude, there is ample evidence that suggests a rising trend of adenocarcinoma in India and has surpassed squamous cell carcinoma in southern India as the commonest type of lung cancer. The male-to-female ratio in lung cancer is gradually diminishing. Larger population-based data according to histological types of lung cancer are needed to further substantiate the current observation.
NSCLC – Non Small Cell Lung Cancer, NSCLC Undiff – Non Small Cell Lung Cancer undifferentiated, SCLC – Small Cell Lung Cancer