Since several years, damage to pulp has been a key consideration in dental treatment. The pulp is highly responsive to thermal damage. A variety of restorative and prosthetic procedures such as preparation of cavity, tooth preparation, polymerisation of lining materials and curing of restorative resin materials are potential sources of thermal damage to the pulp [1,2]. Several other factors such as the thickness and shade of the restorative material, its contents, porosity, duration of curing and Residual Dentin Thickness (RDT) also cause thermal damage to the pulp [3]. Curing lights are used for polymerisation of light cure resin based composites and other dental materials that can be cured with light. Curing lights are of several types that include Quartz Tungsten Halogen curing light (QTH), Light Emitting Diode (LED) curing light, Plasma Arc lights (PAC) and Argon ion lasers. Animal studies in the literature on rhesus monkeys have shown that a rise in the intrapulpal temperature by 5.6°C resulted in irreversible pulpal damage and pulpitis in 15% of monkeys whereas 11°C and 16.6°C increase in the pulpal temperature caused pulpal damage in 60% and 100% of monkeys respectively [1]. Intrapulpal rise in temperature during curing of light activated resin materials relates to heat released during polymerisation of the material and heat emanated from the dental curing light, with the heat from the curing light being the major contributing factor [3,4]. The type of curing light may also affect the intensity of thermal damage caused to the pulp.
This study was designed to evaluate the temperature rise caused by different light curing units i.e., LED, QTH, PAC and to examine the influence of RDT i.e., 2mm, 1mm and 0.5 mm on the temperature increase in pulp in vitro.
Materials and Methods
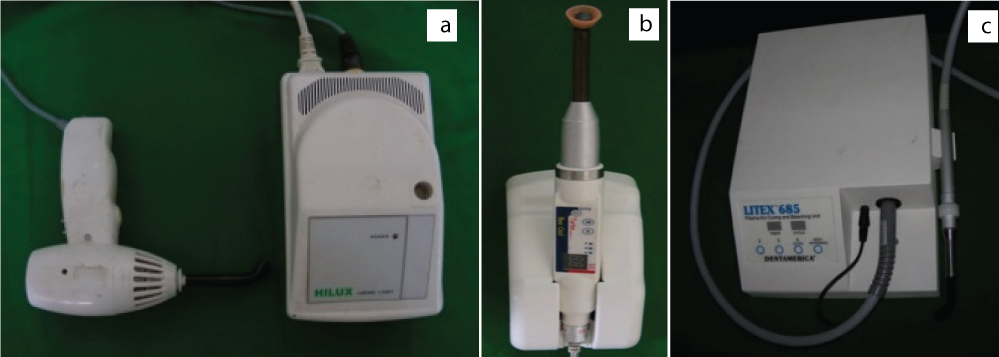
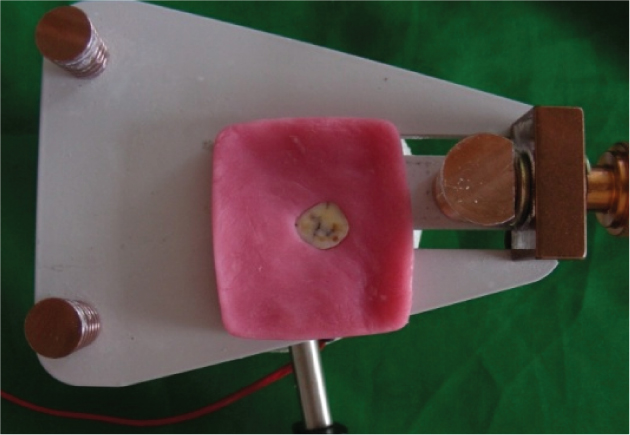
The materials used in the study were cold cure acrylic base plate for stabilization [Table/Fig-1] dentin disks of three different thicknesses i.e., 2mm, 1mm and 0.5mm [Table/Fig-2]. The three curing lights used were Quartz tungsten halogen (QTH, HILUX 250), Light emitting diode (LED, Be Cool Turbo) and Plasma arc curing (PAC, Dentamerica LITEX-685) [Table/Fig-3].
Stabilization of dentin disk in cold cure acrylic.

Dentin disks of different thicknesses (0.5mm, 1mm and 2mm).

Quartz tungsten halogen (a), Light emitting diode (b), Plasma arc curing (c).
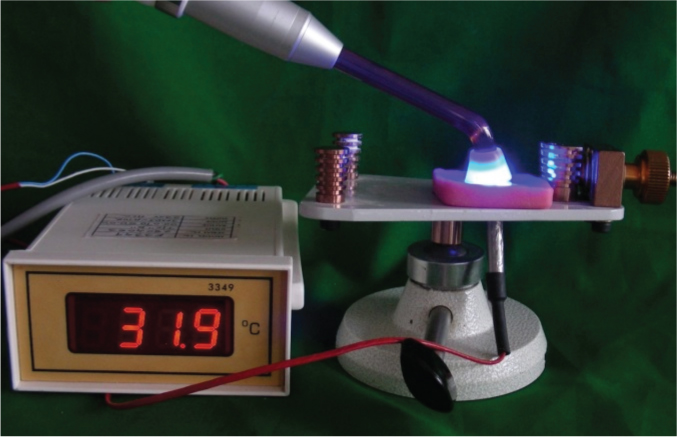
A thermocouple with its tip secured to a digital thermometer was used for evaluation of the temperature. An outlet was made on the opposing side of the cold cure acrylic base plate with the attached dentin disk for the attachment of the thermocouple [Table/Fig-4,5]. The thermocouple was placed at the centre of the outlet prepared and the light guide exit windows of the light curing units were placed above the dentin disks in the centre and activated for time duration of 20 seconds [Table/Fig-6]. The temperature rise was noted.
Outlet made on the opposing side for the attachment of thermocouple.

Attachment of thermocouple to dentin disk.
Light curing of composite resin placed on dentin disk to which a thermocouple is attached.
The same arrangement and procedure is repeated for the dentin disks of 2mm, 1mm and 0.5mm thicknesses. For statistical analysis, the data registered with the above mentioned arrangement was then subjected to one-way ANOVA and t-test with a significance level of 0.05.
Results
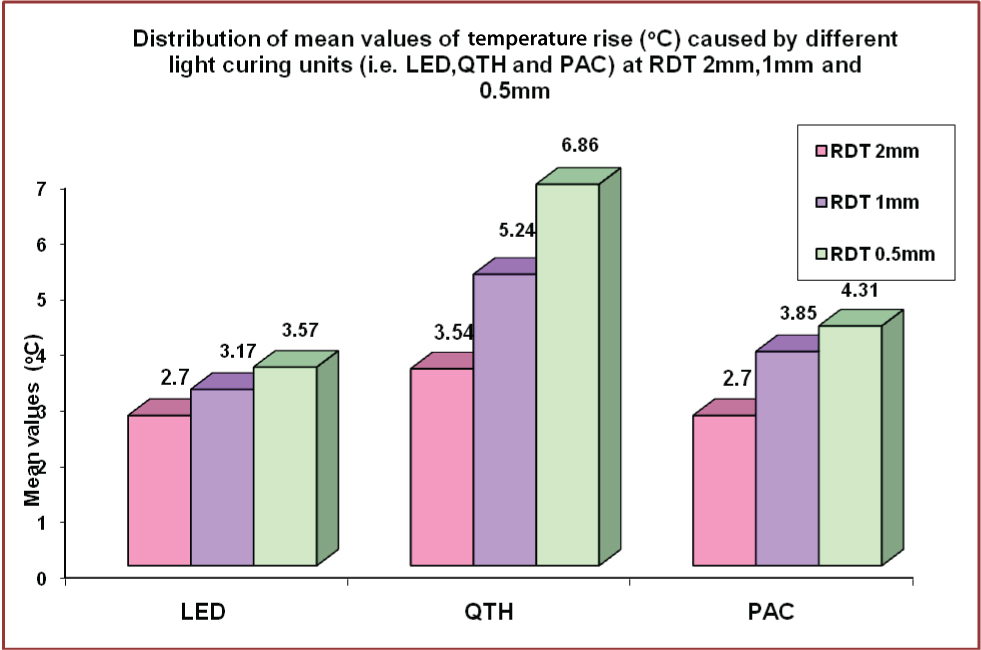
The changes in the intrapulpal temperature due to LED, QTH and PAC with 0.5mm, 1mm and 2mm RDT dentin disks were determined as a difference between the initial and maximum temperature values. When the dentin disks of 2mm RDT were cured by LED, QTH and PAC, a significantly higher rise (p < 0.05) in intrapulpal temperature was observed with the use of QTH in all the 10 samples with a difference of approximately 10C [Table/Fig-7,8]. A higher temperature rise was observed with reduced thickness of dentin disks. The temperature rise with 1mm dentin disks was higher with use of QTH than other curing lights and also higher than the rise observed with 2mm RDT disks by approximately 1.40C [Table/Fig-7,9]. There was a difference of temperature rise on curing of approximately 40C between dentin disks of 2mm and 0.5 mm thickness [Table/Fig-7,10].
Comparison of Mean effects across the three RDT groups (0.5, 1, 2 mm) across the three light curing units (LED, QTH, PAC).
| Light curing units | RDTmm | n | Mean | Std. Dev. | Significance of Mean difference | | | |
|---|
| LED | Groups | | | | Pairs for comparisons | Mean difference | p-value | Significance |
|---|
| 0.5 | 10 | 3.57 | 0.27 | 0.5 Vs 1mm | 0.4 | 0.087 | NS |
| 1 | 10 | 3.17 | 0.28 | 0.5 Vs 2mm | 0.87 | 0.001 | HS |
| 2 | 10 | 2.7 | 0.55 | 1 Vs 2mm | 0.47 | 0.035 | S |
| Total | 30 | 3.15 | 0.52 | Across the 3 groups | 0.0001 | HS |
| QTH | 0.5 | 10 | 6.86 | 0.49 | 0.5 Vs 1mm | 1.62 | 0.001 | HS |
| 1 | 10 | 5.24 | 0.35 | 0.5 Vs 2mm | 3.32 | 0.001 | HS |
| 2 | 10 | 3.54 | 0.25 | 1 Vs 2mm | 1.7 | 0.001 | HS |
| Total | 30 | 5.21 | 1.43 | Across the 3 groups | 0.001 | HS |
| PAC | 0.5 | 10 | 4.31 | 0.36 | 0.5 Vs 1mm | 0.46 | 0.029 | S |
| 1 | 10 | 3.85 | 0.16 | 0.5 Vs 2mm | 1.61 | 0.001 | HS |
| 2 | 10 | 2.7 | 0.51 | 1 Vs 2mm | 1.15 | 0.001 | HS |
| Total | 30 | 3.62 | 0.78 | Across the 3 groups | 6.001 | HS |
Statistical significance determined by following tests S: Significant Across the group comparisons: by One-way ANOVA (F-test) HS: Highly significant pair-wise comparisons: by Bonferroni Multiple Comparison test NS: Not significant
Change in intrapulpal temperature due to LED, QTH and PAC (in degree Celsius) with 2mm RDT
| RDT 2mm | LED (oC) | QTH (oC) | PAC (oC) |
|---|
| 1 | 3.1 | 3.9 | 3.0 |
| 2 | 2.3 | 3.6 | 2.1 |
| 3 | 2.3 | 3.3 | 2.1 |
| 4 | 2.1 | 3.6 | 3.3 |
| 5 | 3.4 | 3.6 | 3.5 |
| 6 | 2.1 | 3.1 | 2.6 |
| 7 | 2.3 | 3.9 | 2.3 |
| 8 | 2.7 | 3.3 | 2.7 |
| 9 | 3.5 | 3.5 | 2.3 |
| 10 | 3.2 | 3.6 | 3.1 |
Change in intrapulpal temperature due to LED, QTH and PAC (in degree Celsius) with 1mm RDT.
| RDT 1mm | LED (oC) | QTH (oC) | PAC (oC) |
|---|
| 1 | 3.5 | 4.8 | 3.6 |
| 2 | 3.1 | 5.4 | 3.8 |
| 3 | 2.8 | 5.0 | 3.8 |
| 4 | 3.4 | 5.6 | 3.8 |
| 5 | 3.3 | 5.0 | 3.9 |
| 6 | 3.1 | 4.8 | 3.7 |
| 7 | 3.0 | 5.6 | 3.9 |
| 8 | 3.6 | 5.2 | 4.1 |
| 9 | 2.8 | 5.2 | 3.8 |
| 10 | 3.1 | 5.8 | 4.1 |
Change in intrapulpal temperature due to LED, QTH and PAC (in degree Celsius) with 0.5 mm RDT.
| RDT 0.5mm | LED (oC) | QTH (oC) | PAC (oC) |
|---|
| 1 | 3.5 | 7 | 4 |
| 2 | 3.3 | 6.2 | 3.8 |
| 3 | 3.3 | 6 | 4.2 |
| 4 | 3.3 | 7.3 | 3.8 |
| 5 | 3.7 | 7.1 | 4.6 |
| 6 | 3.9 | 6.6 | 4.4 |
| 7 | 3.3 | 7.4 | 4.4 |
| 8 | 3.9 | 7.1 | 4.9 |
| 9 | 3.9 | 6.6 | 4.6 |
| 10 | 3.6 | 7.3 | 4.4 |
When the results were compared among PAC and LED, the intrapulpal rise in temperature was significantly higher (p < 0.05) with PAC. With respect to QTH and LED and QTH and PAC, QTH had highly significant values (p < 0.05) of temperature rise when compared to LED and PAC [Table/Fig-7,11].
Mean values of temperature rise caused by LED, QTH and PAC curing lights on dentin disks of 2mm, 1mm and 0.5mm thickness (Green colour key in figure).
Discussion
This study evaluated the intrapulpal temperature rise by the use of three different curing lights, LED (Light emitting diode), QTH (Quartz tungsten halogen) and PAC (Plasma arc curing) on dentin disks of 2mm, 1mm and 0.5mm thickness.
It has been suggested that high performance curing lights cause an increase in the intrapulpal temperature and result in pulpal necrosis. The normal temperature of pulp is about 1.7°C in incisors, 1.9°C in premolars and 1.2°C in molars and the critical threshold where pulpal changes can be observed is 5.5°C [1]. The mechanism of pulpal temperature rise does not involve infection or any microorganisms and the signs and symptoms of pulpal necrosis can be observed after several months of exposure to curing light. At this time it gets difficult for the clinician to diagnose or relate the symptoms to pulpal changes resulting from curing light. Pulpal blood flow rate which is high in dental pulp as compared to other oral tissues also makes the tooth more susceptible to temperature change [5].
Several studies have reported that the heat generated during restorative procedures is harmful to the pulp [6,7] and that the heat generated by the light source is mainly responsible for the pulpal temperature rise [8]. High energy output sources cause more damage than low energy output sources [9].
Diverse combinations of curing lights and dentin disks of different thicknesses produced statistically significant differences in temperature rise. The traditional clinical threshold of 5.5°C was reached when QTH was used on dentin disks of 0.5mm thickness. Therefore, the combination of curing light, restorative material and tooth anatomy should always be considered before any restorative or prosthetic procedures.
Among all the curing lights, the lowest rise in intrapulpal temperature was caused by LED curing light. However, it should not be understood by the clinicians that LED will not cause damage to the pulp or is the best curing light. Compared to LED and PAC curing lights, QTH caused significantly higher temperature rise considering its low irradiance value (790 mW/cm2). As the power of the curing lights reduce, the irradiation time increase proportionately [9].
[Table/Fig-11] show a steep increase in the temperature rise when QTH was used with reducing dentin thickness. It is a rational hypothesis that the intrapulpal temperature rise would be higher with longer duration of irradiation. The tooth anatomy i.e., the size of the pulp chambers and RDT also plays a significant role in pulpal temperature rise.
Similar results have been reported by Rajesh Ebenezar AV et al., Ulusoy C et al., Uzel A et al., and Malkoc S et al., that reported higher temperature rise caused by halogen lights as compared to LED and PAC [10-13]. However, some studies have reported contradictory results to the present study, stating that LED and halogen are low energy output sources and cause lower temperature rise as compared to PAC [14]. Another study also reported fewer rises in temperature to a traditional halogen curing light as compared to high energy output sources [15]. A study carried out to evaluate the effect of light activation of composite restoration on primary molar concluded that LED curing light caused a significant elevation of intrapulpal temperature of greater than 5.5 degree Celsius [16]. Another study indicated that the intrapulpal temperature rise is affected by remaining dentin thickness during light curing of composite resin [17].
Since the exothermic reaction during polymerisation reaction of light activated resin restorative materials and heat emanating from the curing lights cannot be avoided, the finding that intrapulpal temperatures can be raised to a value that can damage the pulp is of concern to the dental clinicians. Nevertheless, several restorations have been performed without a significant pulpal damage. Therefore, precautions should be taken by the clinicians such as conservative cavity preparation allowing the RDT to be more which insulates the pulp chambers from the heat, use of a cavity liner material that does not generate heat and needlessly long irradiation periods.
Conclusion
The lowest intrapulpal temperature rise was induced by LED curing light. This study shows that the remaining dentin thickness is inversely proportional to the temperature rise and that the choice of curing light is crucial when polymerising light activated resin based restorations to minimise any thermal damage to the pulp. Type of curing light, type of restorative material, tooth anatomy affect the pulpal temperature. The clinician should be aware of all these factors and should take them into consideration to prevent thermal damage to the pulp.
Statistical significance determined by following tests S: Significant Across the group comparisons: by One-way ANOVA (F-test) HS: Highly significant pair-wise comparisons: by Bonferroni Multiple Comparison test NS: Not significant