Introduction
Measuring arterial blood gas, which is performed in different parts of the body, plays an important role in clinical evaluation.
Aim
The present study was conducted to determine the effect of position change on arterial oxygen saturation in different parts of the body, in cardiac and respiratory patients.
Materials and Methods
The present randomised clinical trial was conducted on 169 hospitalised patients admitted to 22 Bahman Hospital of Gonabad in 2016. Patients were selected through convenient sampling, then were randomly assigned into three groups of cardiac patients, respiratory patients and control. Initially, the patient was placed in a semi-fowler’s position for 15 minutes; then, arterial oxygen saturation was measured at three points i.e. the auricle, fingertip and tip of the greater toe simultaneously. Then, the patient was placed in the supine and prone positions and the arterial oxygen saturation was measured following the same protocols of the former position. Collected data were analysed at a significance level, p-value less than 0.05 by SPSS-version 20 through the analysis of variance with repeated measures, independent t-test and Pearson correlation coefficient.
Results
The mean oxygen saturation percentage has statistically significant difference at different positions (p=0.016). It was also found that there was a significant difference between the mean oxygen saturation on three different points i.e. fingertip, auricle and the tip of the greater toe (p<0.001).
Conclusion
The arterial oxygen saturation in the semi-fowler’s position and the auricular point were higher in the three groups of patients with and without cardio-respiratory disorder than other positions and body points.
Introduction
Constant control of blood oxygen saturation using a finger pulse oximeter is known as a routine and standard technique for caring for ill patients. The measurement of arterial blood gas plays an important role in clinical evaluation and has been widely used over the past three decades. In this method, the sensor of the device is placed on various parts of the body, including fingers, toes, legs, and nasal tip. The result of various researches done on the effect of the location of pulse oximeter shows that there is a difference in the measurement results [1].
Physical positions are varied and include supine, prone, semi-prone, lateral, fowler’s, semi-fowler’s, hi-fowler’s positions etc. Each position has a specific application. In sitting positions, fowler’s position is said to be the position were the patient’ bed has a 45 degree angle to the horizontal. This inclination is 30° for the semi-fowler’s position and 90° for the hi-fowler’s position. Different physical states can produce different physiological effects, such as cardiovascular and respiratory changes, which occur mainly due to the effect of gravity on the bloodstream and its distribution in the venous, pulmonary and arterial systems. Changes in the diaphragm, which occur mainly due to abdominal visceral pressure, are among the factors influencing the respiratory effects of various states of the body [2].
Berry EC and Kohn ML, introduced the prone condition first as a therapeutic maneuver for pulmonary diseases in 1974. Different studies have been done on both children and adults, and in almost all of these studies, the improvement of the oxygenation state has been reported in the prone state compared to the supine position. In addition to improving the respiratory state, the prone condition has other benefits, including improvement in neuronal development in neonates. Many researchers have hypothesised that improved oxygenation in the abdomen is practical for increasing residual capacity. Improving the state of oxygenation in the abdomen may be due to a reduction in the pressure of the abdominal organs on the aperture and allowing it to move more due to increased lung volume [3].
However, some believe that prone position, with the effect of compression due to weight on the chest wall, is likely to cause lower levels of pulmonary volume [4]. In patients with respiratory distress syndrome and in pulmonary damage, the reason for improved arterial oxygen saturation in the abdomen can be due to improved blood flow and pulmonary ventilation, as well as a reduction in intrapulmonary shunt [5]. Also, the prone position can reduce airway resistance and improve the coordination of chest-abdominal movements in patients with severe airway problems [6].
The improvement of oxygenation in prone condition in preterm infants is unjustifiable due to the increased strength of the respiratory muscles, since it seems that the strength of the muscles in the prone position does not increase the strength of the respiratory muscles [7].
The position of the body at the time of measurement is one of the most important factors; if the physiological characteristics of individuals differ with varying the position of the body, it might lead to an inadequate diagnosis of the patient and improper use of drugs that are not only useful to the patient but also sometimes endangers the patient’s life [8,9]. Cardiovascular disease is one of the most prevalent disorders that have become widespread due to new possibilities and technologies, lifestyle changes and modern lifestyles [10]. According to World Health Organisation statistics, in developing countries like India, cardiovascular mortality rates have increased from 9 million in 1990 to more than double in 2020, accounting for three-quarters of total deaths [11]. Nowadays, patient satisfaction is considered as one of the important indicators for assessing the quality of care provision. The limitation of movement affects patients’ satisfaction by causing fatigue and patients need to adopt different physical conditions and rest during the stages of illness and admission. Doctors and nurses may also disregard this important fact and do medical experiments and clinical observations regardless of the position the body of the patient is in and they might monitor, interpret, and decide on the conditions of the patient [12]. On the other hand, considering the importance of physiological indicators in the special sectors and their role in the amount of oxygen demand in the myocardium, accurate measurements of these indicators can be a way to prevent adverse side effects in these patients [13]. Although, generally speaking, semi-fowler’s conditions are advisable for these patients [14], the fact is that keeping patients in this situation is not feasible during the whole period of hospitalization and during the night and, as mentioned, often a team of therapists will examine these patients and determine cardiovascular parameters by locating patients in different situations, which is quite important in the process of making the best medical decision for the intended patient, a fact which has not been sufficiently addressed in former research. On the other hand, long periods of rest on the bed and in a semi-fowler’s position are difficult and unbearable for many patients, and many of them constantly complain of back pain and tend to relieve the back pain and increase their comfort through changing the position of their body on the bed. Studies show that this type of back pain is caused by motionlessness and limitation of the patient’s condition in a semi-fowler’s position [15]. Pain as an unpleasant mental sensation with the onset of stress response causes various complications such as activation of the sympathetic system; pain, generally, results in increased heart rate, blood pressure and respiratory rate, decreased pulmonary volume, and ultimately increased myocardial ischaemia [16]. Therefore, providing a proper procedure for patient positioning and their absolute rest period can, in addition to reducing the amount of pain and providing more comfort for patients and increasing their satisfaction with caring services, prevent secondary complications following an infarction [17].
Considering the necessity of position change and the importance of measuring the oxygen saturation of arterial blood, the present study was conducted to determine the effect of position change on arterial oxygen saturation in cardiac and respiratory patients and compare the results in different positions and points of the body.
Materials and Methods
The present randomised clinical trial was conducted on 169 patients hospitalised in the internal medicine ward and ICU and CCU of 22 Bahman Hospital in Gonabad, Iran, during May 2016 to July 2016. The samples were selected through convenience method then, they were randomly allocated in three groups of cardiac patients, respiratory patients and control.
The sample size was calculated through the following formula for couple studies (dependent two-sampled) with 80% and a confidence level of 95 percent, and of course with the help of similar studies, and it turned to be 111 subjects. In order to provide sufficient samples in the subgroups of patients with and without cardiac and respiratory diseases, modulation formula was used and 157 subjects were selected; also, for the purpose of possible loss, 177 subjects (59 persons per group) were considered.
Consciousness, not having polish on the nail or plaster on the site of the prep and the ability to change position were the main inclusion criteria; also, a request for withdrawal at each stage of the study and a drop in the level of consciousness were the main exclusion criteria. Patients with acute coronary syndrome were selected in the group of cardiac patients and patients with chronic obstructive pulmonary disease in the respiratory group. Patients in the control group had no cardiovascular and respiratory disorders. There was no medical recommendation for patients to observe a specific position. Meanwhile, patients were matched in terms of hospitalisation time and other conditions in three groups.
Required data were collected using a ppm-ARAD-Ver pulse oximeter device made in Iran, which is a standard instrument for measuring the oxygen saturation percentage. Equation reliability was used to determine the reliability of the device and the accuracy of the device was checked and compared every day before the start of work with another pulse oximeter machine. The checklist of data collection includes information such as sex, age, marital status, arterial oxygen saturation in prone, supine and semi-fowler’s positions (three positions), and also the amount of arterial oxygen saturation in different parts of the body, such as the tip of the thumb, the tip of the greater toe and the ear auricle.
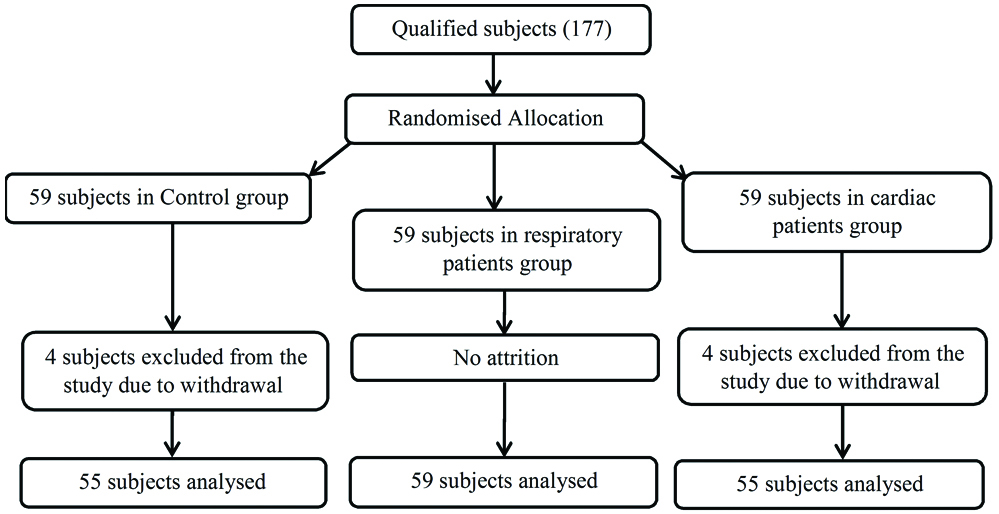
After approving the research, obtaining the ethics license, carrying out the necessary coordination with the research deputy of Gonabad University of Medical Sciences and the officials of the 22 Bahman hospital of Gonabad and the internal, ICU and CCU departments, the patients who were eligible for inclusion criteria were selected by convenience sampling method. After describing the goals of the research and obtaining informed consent from the participants, they were assigned randomly by simple method to three groups of patients with cardiac and respiratory disease and control. The percentage of arterial oxygen saturation was measured in different positions, as well as in different parts of the body, by pulse oximeter and recorded in the checklist for the three groups. First, the patient was placed in a semi-fowler’s position for 15 minutes [18], and the arterial oxygen saturation percent was measured simultaneously in three sites of the tip of the thumb, the tip of the greater toe and the ear auricle. Then, the patient was placed supine and prone positions and the oxygen saturation percentage was measured simultaneously at different parts in the previous manner [Table/Fig-1]. The procedure conducted in same day. There was an interval of 15 minutes between positions. No complication during or after the study was observed. There was not any follow up.
Process execution chart (based on CONSORT).
The main ethical consideration observed in the present study included the acknowledgement of the Ethics Committee of Gonabad University of Medical Sciences (Code of Ethics: GMU.REC.1393.19), coordination with the research environment, obtaining informed written consent from the subjects; assuring the samples in terms of confidentiality of their personal information, informing the subjects to be free to leave the study at each stage, informing the subjects about the possibility of placement in all three groups randomly, and registering the study with the IRCT2016082817800N2 code at the Test Registration Center Iranian Clinical Sciences.
Statistical Analysis
Collected data was analyzed using SPSS version 20.0. To analyse the data, descriptive statistics (mean, standard deviation, relative frequency and percentage) and analytical statistics (such as ANOVA tests with repeated observations, independent t-test, Pearson’s correlation coefficient and chi-square) were used and p-value less than 0.05 was considered significant.
Results
Out of 177 subjects (59 in each group) participating in the present study, 4 subjects in the control group and 4 subjects in cardiac disease group withdrew from the study. Finally, data collected from 55 patients in the cardiac group, 59 in the respiratory group and 55 in the group of patients in the control group was analysed [Table/Fig-1].
The mean age of subjects in cardiac, respiratory, and control groups turned out to be 71.72±12.88, 72.62±12.52 and 66.45±17.46 years respectively. According to the results of one-way ANOVA, there was no significant difference between the mean age of the three groups (p=0.05). The majority of subjects in all three groups were women (54.54% in the cardiac group, 57.62% in the respiratory tract and 65.45% in the in control group) and the chi-square test showed no significant difference between the groups in terms of gender distribution (p=0.48). the majority of samples were married in all three groups (89.09% in the cardiac group, 91.52% in the respiratory group and 83.63% in the control group) and chi-square test showed no significant difference between the groups in terms of marital status (p=0.41).
The results of ANOVA test with repeated observations indicate that there is a significant difference between the two positions in terms of the average percentage of saturation of the fingertip oxygen (p=0.016). The Least Significant Difference (LSD) post-hoc test showed that the observed difference was due to the difference between the prone positions as compared to two other positions. The average oxygen saturation percentage in the position of the lower abdomen is less than that of the semi-fowler’s position and the rest; it, also, has the highest rate in semi-fowler’s position. There was no significant difference between the mean oxygen saturation of the eardrum and foot in different positions (p>0.05).
There was a statistically significant difference in the mean percentage of oxygen saturation of the tip of the thumb, the tip of the leg and the ear auricle in semi-fowler’s, supine and prone positions (p<0.05). The LSD post-hoc test showed that the observed difference was due to the difference in the mean oxygen saturation percentage of the ear auricle with two other sites. In all three positions, the percentage of oxygen saturation in the eardrums was the highest and that of the tip of the greater toe was the lowest.
As shown in [Table/Fig-2], according to the results of ANOVA with repeated observations, the mean oxygen saturation of the semi-fowler’s position of the patients in the three groups was significantly different in three locations (p<0.05). The LSD post-hoc test showed a difference between the heart rate and respiratory disease in the group of cardiovascular patients due to the difference in mean of oxygen saturation in the ear auricle and in the respiratory group due to the difference in the mean oxygen saturation of the foot with two other sites. In two groups of cardiac disease and control, the mean percentage of oxygen saturation in the ear auricle turned out to be higher than the tip of the fingers and feet. In the respiratory group, the mean oxygen saturation of the foot was lower than the tip of the finger and the ear auricle. Based on one-way ANOVA, there was a statistically significant difference in the mean oxygen saturation of the thumb between the three groups (p=0.04), but there was no statistically significant difference at two other points (p<0.05).
Comparison of mean oxygen saturation of arterial blood in patients in three groups in different parts of the body in a semi-fowler’s position.
| GroupPoint | Cardiac patients | Respiratory patients | Control | One-way ANOVA test results |
|---|
| Mean±SD | Mean±SD | Mean±SD |
|---|
| Fingertip | 91.8±4.93 | 93.5±3.51 | 92.8±4.48 | F=2.28df=2p=0.10 |
| Ear auricle | 92.9±4.56 | 93.3±4.08 | 93.7±4.10 | F=0.55df=2p=0.57 |
| Toe | 91.9±4.31 | 91.6±4.27 | 93.5±4.13 | F=3.23df=2p=0.04* |
| Results of ANOVA test with repeated measures and LSD | F=5.44df=2p=0.003* | F=13.56df=2p=0.001* | F=3.27df=2p=0.004* | |
*Significant values at p-value <0.05
According to the results presented in [Table/Fig-3], based on the results of ANOVA with repeated observations, there was a significant difference between the mean oxygen saturation of cardiorespiratory patients in three examined sites in supine position (p<0.05). The LSD post-hoc test showed that the difference was observed in the cardiac group was due to the difference in the mean oxygen saturation of the thumb and in the respiratory group due to the difference in mean of the saturated oxygen saturation of the ear auricle in two other places. In the cardiac group, the mean oxygen saturation of the foot was lower than the tip of the finger and the ear, and in the respiratory group, the mean percentage of oxygen saturation in the ear auricle was higher than the tip of the fingers and toes. In addition, there was no significant difference between the mean oxygen saturation of the supine position in the control group in three locations (p=0.29). One-way ANOVA showed that there was a statistically significant difference between the mean oxygen saturation percentage of the toes and thumbs between the three groups (p<0.05), but there was no statistically significant difference in the site of ear auricle (p>0.05).
Comparison of mean oxygen saturation of arterial blood in patients in three groups in different parts of the body in supine position.
| GroupPoint | Cardiac patients | Respiratory patients | Control | One-way ANOVA test results |
|---|
| Mean±SD | Mean±SD | Mean±SD |
|---|
| Fingertip | 92.2±4.63 | 91.5±2.72 | 93.8±4.00 | F=5.43df=2p=0.005* |
| Ear auricle | 92.3±4.65 | 92.9±2.63 | 93.4±3.66 | F=1.10df=2p=0.33 |
| Toe | 91.4±4.80 | 90.8±3.98 | 93.3±4.15 | F=4.93df=2p=0.008* |
| Results of ANOVA test with repeated measures and LSD | F=4.66df=2p=0.017* | F=13.59df=2p<0.001* | F=1.24df=2p=0.29 | |
*Significant values p-value <0.05
[Table/Fig-4] shows that based on ANOVA test with repetition of observations, there was no significant difference between the mean oxygen saturation between the cardiac patient and control groups in the three locations of patients (p=0.3 and 0.08, respectively for groups). But in the respiratory group, this difference was significant in three locations (p<0.001). The LSD post-hoc test showed that the observed difference was due to the difference in the mean percentage of saturation of the ear auricle in comparison with the two other sites and the percentage of oxygen saturation in the ear auricle was higher than the fingertip and toe. One-way ANOVA showed that there was a significant difference between the three groups in the mean oxygen saturation percentage at all three points (p<0.05).
Comparison of mean oxygen saturation of arterial blood in patients in three groups in different parts of the body in prone position.
| GroupPoint | Cardiac patients | Respiratory patients | Control | One-way ANOVA test results |
|---|
| Mean±SD | Mean±SD | Mean±SD |
|---|
| Fingertip | 91.2±4.46 | 91.7±3.77 | 91.7±4.05 | F=3.61df=2p=0.02* |
| Ear auricle | 91.6±4.66 | 93.3±3.83 | 93.3±4.12 | F=3.41df=2p=0.03* |
| Toe | 89.8±11.93 | 91.3±4.32 | 91.3±4.31 | F=2.76df=2p=0.06 |
| Results of ANOVA test with repeated measures and LSD | F=1.09df=2p=0.3 | F=10.39df=2p<0.001* | F=0.12df=2p=0.08 | |
*Significant values p-value <0.05
Other findings indicate that there was no significant difference in arterial oxygen saturation in both sexes (p=0.45). It was also found that there was no significant relationship between oxygen saturation percentage in different types of positions and in different points with the age of subjects (p<0.05).
Discussion
The aim of this study was to evaluate the effect of changing different positions on arterial oxygen saturation in cardiac and respiratory patients. There turned out to be a significant difference between the two positions in terms of the mean oxygen saturation (p=0.016), so that the average oxygen saturation percentage in prone positions is significantly lower than supine and semi-fowler’s positions. This finding does not overlap with the results of Moeenpoor A and Aghbalian F study, entitled “position effect on arterial oxygen saturation in preterm infants with respiratory distress syndrome in the hospital”. In their study, they found that the percentage of arterial oxygen saturation in the abdomen was significantly higher than the supine position, in the premature infants, with respiratory distress syndrome [19]. This difference in the results can be due to differences in the research community, because the present study was conducted on adults and Moeenpoor’s study on preterm infants.
In the present study, the mean percentage of oxygen saturation of thumb, toes, and ear auricle was significantly different in cardiac, respiratory and control groups (p>0.05). The mean oxygen saturation percentage of the ear auricle was significantly higher than the tip of the toe and the thumb. This finding was consistent with the results of Mosayebi Z et al., study who, also, reported that arterial oxygen saturation was always lower in the lower extremity than in the upper extremity [20].
In this study, the average percentage of oxygen saturation in the fingertip of respiratory patients was significantly different in three positions (p<0.001). The average oxygen saturation percentage in the semi-fowler’s position is significantly higher than the supine and prone positions. The researchers studied three groups of patients with normal status, patients with pulmonary oedema and patients with cardiac disease, and found that the compliance was higher in semi-fowler’s position in comparison with fowler’s position in all patients [21,22].
This finding, however, isn’t consistent with the results of Farhadi N et al., study, on the effect of different body positions on arterial oxygen saturation in paramedicine students at Yasuj University of Medical Sciences. The results of their study indicated that the average percentage of oxygen saturation in the arterial blood is the same for prone and supine positions [23]. Probably the reason for the lack of consistency is that Farhadi’s study was performed on healthy students, however current study was done on patients, and on the other hand, subjects in Farhadi’s study were placed in a semi-fowler’s position in lithotomy position. Also, some researchers examined the status of different physical positions on the percentage of arterial oxygen saturation in patients with stroke, the results of which showed no significant changes in arterial blood gas levels, including arterial oxygen saturation, a fact which is not consistent with the findings of the present study [24,25]. This difference might be due to the difference in the population studied in two research. Raymond studied stroke patients while the present study was conducted on patients with respiratory and cardiac disease [24].
Limitation
Some limitations of the present study include the lack of cooperation between the patients and their family to change the position repeatedly, the lack of access to advanced arterial oxygen measurement, and the limitation of the number of measuring devices.
It is suggested that future studies should be conducted on larger sample ranges with more frequent measurements of arterial oxygen and other types of positions as well as different patients.
Conclusion
In general, the present study showed that arterial blood oxygen in the earauricle and in the semi-fowler’s position is higher than other points and positions; thus, these should be considered, while providing nursing care, and evaluating arterial oxygen saturation, for cardiac, respiratory and even patients without respiratory and cardiac disease.
*Significant values at p-value <0.05
*Significant values p-value <0.05
*Significant values p-value <0.05
[1]. Chair SY, Taylor-Piliae RE, Lam G, Chan S, Effect of positioning on back pain after coronary angiographyJournal of Advanced Nursing 2009 42(5):470-78.10.1046/j.1365-2648.2003.02646.x12752867 [Google Scholar] [CrossRef] [PubMed]
[2]. Perkins GD, Mcaulery DF, Gilles S, Routledge H, Gao F, Changes in pulse oximeter oxygen saturation predict equivalent changesPublic Health 2003 7(4):67 [Google Scholar]
[3]. Berry EC, Kohn ML, Operating room technique 2004 ST louisMosby co:477 [Google Scholar]
[4]. Dimitrious G, Greenough A, Pink L, McGhee A, Hickey A, Rafferty GF, Effect of posture on oxygenation and respiratory muscle strength in convalescent infantsArchives of Disease in childhood, Fetal and Neonatal Edition 2002 86:147-50.10.1136/fn.86.3.F14711978742 [Google Scholar] [CrossRef] [PubMed]
[5]. Mohammadzade A, Alizade B, Amiri B, The effect of health care for low birth weight on arterial oxygen saturationJournal of Mashhad University of Medical Sciences 2005 87:48 [Google Scholar]
[6]. Brayan AC, Comments of a devil’s advocateThe American Review of Respiratory Disease 1974 110:143-44. [Google Scholar]
[7]. Aiton NR, Fox GF, Alexander J, Ingram DM, Milner AD, The influence of sleeping position on functional residual capacity and effective pulmonary blood flow in healthy neonatesPediatrics Pulmonary 1996 22:342-47.10.1002/(SICI)1099-0496(199612)22:6<342::AID-PPUL2>3.0.CO;2-L [Google Scholar] [CrossRef]
[8]. Hakim TS, Dean GW, Lisbona R, Effect of body posture on spatial distribution of pulmonary blood flowJournal of Applied Physiology 1988 23:694-705.10.1152/jappl.1988.64.3.11603259226 [Google Scholar] [CrossRef] [PubMed]
[9]. Numa AH, Hammer J, Newth CJ, Effect of prone and supine positions on functional residual capacity, oxygenation and respiratory mechanics in ventilated infants and childrenAmerican Journal of Respiratory and Critical Care Medicine 1997 156:1185-89.10.1164/ajrccm.156.4.96010429351620 [Google Scholar] [CrossRef] [PubMed]
[10]. National Institutes of HealthMorbidity and Mortality: Chart Book on Cardiovascular, Lung and Blood and Diseases 2011 BethesdaUS Department on heart and Human Services, Public health Service [Google Scholar]
[11]. WHO. Cardiovascular diseases (CVDs). Available at: http://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) [Google Scholar]
[12]. Farasyn A, Meeusen R, The influence of non-specific low back pain on pressure pain thresholds and disabilityEuropean Journal of Pain 2005 9:375-81.10.1016/j.ejpain.2004.09.00515979017 [Google Scholar] [CrossRef] [PubMed]
[13]. Mcmanus DD, Gore J, Yarzebski J, Spencer F, Lessard D, Goldberg RJ, Recent trends in the incidence, treatment and outcomes of patients with STEMI and NSTEMIAmerican Journal of Medicine 2011 124(1):40-47.10.1016/j.amjmed.2010.07.02321187184 [Google Scholar] [CrossRef] [PubMed]
[14]. Saul G, Robin P, Cardio Vascular Emergencies’ & Practical procedures 2012 1st edTehranArt in Teb Publication [Google Scholar]
[15]. Bexendale M, Path physiology of coronary artery diseaseNursing Clinics of North America 2008 20(20):143-52. [Google Scholar]
[16]. Urden LD, Stacy KM, Lough ME, Thelan’s critical care nursing: diagnosis and management 2006 MissouriMosby [Google Scholar]
[17]. Yeh RW, Sidney S, Chandra M, Sorel M, Selby JV, Go AS, Population trends in the incidence and outcomes of acute myocardial infarctionNew England Journal of Medicine 2010 362:2155-65.10.1056/NEJMoa090861020558366 [Google Scholar] [CrossRef] [PubMed]
[18]. Adaryani RM, Ahmadi F, Fatehi A, Mohammadi E, Faghih Zadeh PS, The effect of changing position on patients’ fatigue and satisfaction after coronary angiographyIranian Nursing Quarterly 2006 19(48):25-35. [Google Scholar]
[19]. Moeenpoor A, Aghbalian F, Position effect on arterial oxygen saturation in preterm infants with respiratory distress syndrome in the hospitalCalendar of Military Research and Health Sciences 2008 6(1):9-13. [Google Scholar]
[20]. Mosayebi Z, Movahedian AH, Safari A, Akbari H, Review the results of pulse oximetry in the early detection of heart disease congenital cyanotic hands and feet newborns born in hospitals Shabihkhani first six monthsRazi Journal of Medical Sciences 2012 19(101):24-28. [Google Scholar]
[21]. Canand M, Body Position and the mechanics of breathingJournal Canadian Medical Association 2005 75(11):939 [Google Scholar]
[22]. Mohammadpour A, Sharghi RN, Khosravan SH, Alami A, Akhond M, The effect of a supportive educational intervention developed based on the Orem’s self-care theory on the self-care ability of patients with myocardial infarction: a randomized controlled trialJournal of Clinical Nursing 2015 24(11-12):1686-92.10.1111/jocn.1277525880700 [Google Scholar] [CrossRef] [PubMed]
[23]. Farhadi N, Molazem Z, Khosravi A, Ghashghaie ZK, Effects of postural change on oxygen saturationArmaghan-E-Danesh 2005 10(2):59-65. [Google Scholar]
[24]. Raymond C, Hilary J, Valerie M, Martin JC, Brian F, Lindsay C, The effect of body position on arterial oxygen saturation in acute strokeThe Journals of Gerontology, Bio Sciences and Medical Sciences 2000 5(4):239-44.10.1093/gerona/55.4.M23910811154 [Google Scholar] [CrossRef] [PubMed]
[25]. Zarea K, Nikbakht-Nasrabadi A, Abbaszadeh A, Mohammadpour A, Facing the challenges and building solutions in clinical psychiatric nursing in Iran: A qualitative studyIssues in Mental Health Nursing 2012 33(10):697-706.10.3109/01612840.2012.69837123017047 [Google Scholar] [CrossRef] [PubMed]