A Rare Cause of Ophthalmia Neonatorum-Achromobacter denitrificans
Viraraghavan Vadakkencherry Ramaswamy1, Gajanan Venkat Rao2, N Suryanarayana3
1 Consultant, Department of Neonatology, Nori Multispeciality Hospital, Vijayawada, Andhra Pradesh, India.
2 Consultant, Department of Neonatology, Nori Multispeciality Hospital, Vijayawada, Andhra Pradesh, India.
3 Consultant, Department of Neonatology, Nori Multispeciality Hospital, Vijayawada, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Viraraghavan Vadakkencherry Ramaswamy, 504, Sai Bhagwathy Apartments, Gandhi Nagar, Vijayawada, Andhra Pradesh-520003, India.
E-mail: 19.vira@gmail.com
A 72-hour-old neonate presented with lethargy and eye discharge. Keratitis and corneal ulceration was present on the left side. Work up revealed early onset sepsis with meningitis and keratoconjunctivitis. A rare organism, Achromobacter denitrificans was isolated from the blood and the eye discharge. This is the first case report of Achromobacter denitrificans causing early onset sepsis and keratoconjunctivitis in a neonate.
Keratoconjunctivitis, Meningitis, Neonatal sepsi
Case Report
Ophthalmia neonatorum is a very common occurrence in the newborn period. The most common organisms causing this condition are Chlamydia trachomatis, Neisseria gonorrhoeae, Escherichia coli,Klebsiella pneumonia and Staphylococcus aureus. We here report a rare case of keratoconjunctivitis causes by Achromobacter denitrificans in a preterm neonate.
A 72-hour-old neonate was referred from a peripheral level II nursery with lethargy and poor feeding. He was born to a primiparous mother vaginally who had leaking per vaginum since seven days before delivery. History of multiple per vaginal examinations was present. There was no history suggestive of clinical chorioamnionitis such as maternal fever, uterine tenderness, maternal or foetal tachycardia and maternal leucocytosis. There was history of wiping the eyes immediately after birth with saline soaked gauze which was a common practice in that setting. Prophylactic antibiotic drops for prevention of ophthalmia neonatorum were not administered.
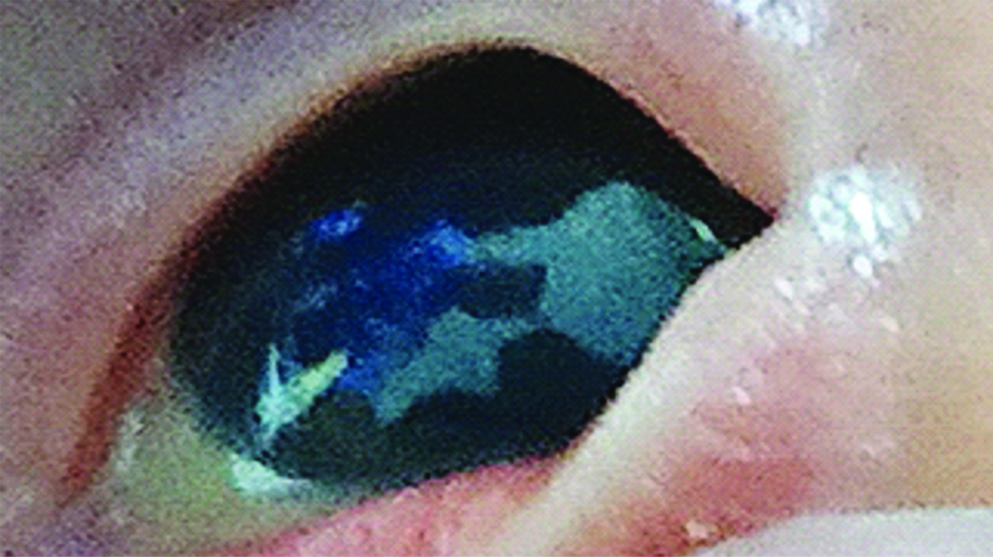
At the time of admission, baby was lethargic. Bilateral purulent eye discharge was present. The left cornea had a corneal ulceration of about 2X2 mm in the 5 o’clock position just extending into the central region [Table/Fig-1]. Blood cultures, conjunctival swabs for culture, gram stain and other tests for sepsis work up were sent. Sepsis screen was positive with leucopenia (3200/mm3), neutropenia (800/mm3) and elevated C-Reactive Protein levels (35 mg/L). Lumbar puncture was done and revealed meningitis with Cerebrospinal Fluid (CSF) analysis showing 340 cells/mm3 (90% Neutrophils), protein of 174 mg/dL and sugar of 25 mg/dL. However, CSF culture was sterile.
Active corneal ulceration involving the 3 to 5 O’Clock position.
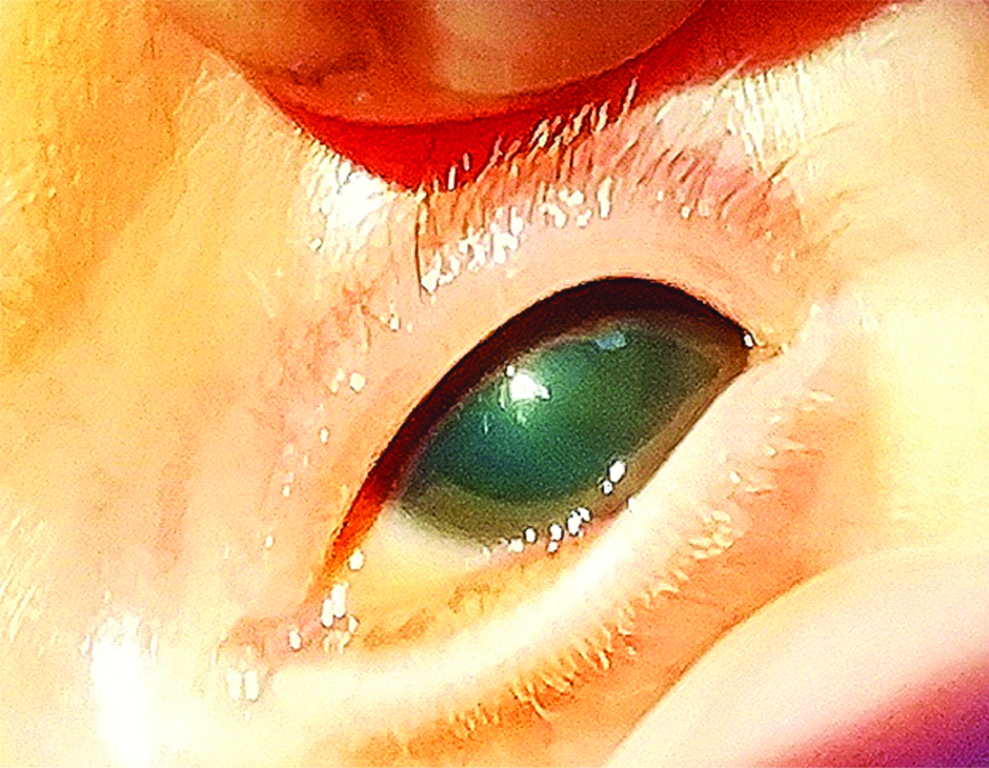
The baby was started on intravenous antibiotics namely, meropenem and amikacin. He was also started on tobramycin eye drops, Carboxymethyl cellulose eye drops and atropine oinment. Symptomatic improvement was present in the form of improving activity over the course of next 48 hours. The gram stain of the conjunctival swab revealed gram negative rods and plenty of pus cells. The conjunctival swab and the blood cultures (BACTEC) revealed the growth of Achromobacter denitrificans. It was sensitive to meropenem, piperacillin tazobactum, levofloxacin, ceftazidime and cefoperazone sulbactum. It was resistant to amikacin, gentamycin, and colistin. Amikacin was stopped and ceftazidime was added. Intravenous antibiotics were given for a total duration of 21 days. Topical tobramycin was changed to 0.5% moxifloxacin eye drops and was given for 14 days. Corneal ulcer subsequently healed after a week of topical antibiotic and cycloplegic therapy, with a residual opacity in the 5 o’clock position [Table/Fig-2]. The baby was discharged on day 25 of life with advice to follow up with the ophthalmologist.
Residual corneal opacity in the neonate.
Discussion
This was a case of early onset neonatal sepsis with meningitis and ophthalmia neonatorum caused by a rare organism Achromobacter denitrificans.Achromobacter denitrificans was first identified in 1971 [1]. It is an aerobic gram negative rod which can cause opportunistic infections in immunocompromised individuals [2]. It can be found as a normal commensal in the gastrointestinal tract and can also colonise saline bottles and water supply in hospital settings resulting in outbreaks. Several cases of meningitis in newborns have been reported in the literature. Most of these cases are associated with bad outcomes in the form of high mortality and high morbidity such as hydrocephalus [3,4]. This case also had meningitis, which however responded to therapy.
Spierer O et al., had described the clinical features and outcomes of Achromobacter denitrificans keratitis in a case series of 28 adults [5]. The most common scenarios included post-operative cases of corneal transplantation, shrapnel injury, contact lens use, dry eye syndrome and in topical corticosteroid use. However, till date no case of ophthalmia neonatorum or early onset neonatal sepsis caused by this organism has been reported. Similar to that in adults, this baby also had a poor visual outcome with corneal scarring. Even though, the mother had many risk factors for early onset neonatal sepsis, the exact source of this organism from where the baby got infected was not known. It most likely was from the saline soaked gauze that was used to wipe the eye lids soon after birth. It might also be from the maternal birth canal.
This organism is resistant to commonly used antibiotics such as aminoglycosides [6]. Early diagnosis and treatment is of utmost importance. The infections caused by this organism most likely have been under reported in the literature because of the difficulty in positively identifying the organism. The reason for this is not that it is difficult to culture this organism, but that it is morphologically very similar to other gram negative rods. This organism can be easily confused with Pseudomonas aeruginosa which is also a gram negative rod [6].
This is the first case report of Achromobacter denitrificans causing early onset sepsis and keratoconjunctivitis in a neonate.
Conclusion
The lesson for the clinician is that unnecessary wiping of eyelids with saline soaked gauze soon after birth should not be done. Also, whenever a gram negative rod is isolated in any culture sample or gram stain of a conjunctival discharge, apart from pseudomonas, Achromobacter denitrificans should be thought of.
[1]. Yabuuchi E, Ohyama A, Achromobacter xylosoxidans n. sp. from human ear dischargeJpn J Microbiol 1971 15:477-81.10.1111/j.1348-0421.1971.tb00607.x5316576 [Google Scholar] [CrossRef] [PubMed]
[2]. Reverdy ME, Freney J, Fleurette J, Coulet M, Surgot M, Marmet D, Nosocomial colonization and infection by Achromobacter xylosoxidansJ Clin Microbiol 1984 19:140-43.10.1128/JCM.19.2.140-143.19846699141 [Google Scholar] [CrossRef] [PubMed]
[3]. Boukadida J, Monastiri K, Snoussi N, Jeddi M, Berche P, Nosocomial neonatal meningitis by Alcaligenes xylosoxidans transmitted by aqueous eosinPediatr Infect Dis J 1993 12:696-97.10.1097/00006454-199308000-000157692379 [Google Scholar] [CrossRef] [PubMed]
[4]. Lee SL, Tan KL, Achromobacter meningitis in the newbornSingapore Medical Journal 1972 13(5):261-65. [Google Scholar]
[5]. Spierer O, Monsalve PF, O’Brien TP, Alfonso EC, Gologorsky D, Miller D, Clinical features, antibiotic susceptibility profiles, and outcomes of infectious keratitis caused by Achromobacter xylosoxidansCornea 2016 35(5):253-55.10.1097/ICO.000000000000079826989957 [Google Scholar] [CrossRef] [PubMed]
[6]. Rush R, Friedlander M, Alcaligenes xylosoxidans conjunctivitisCornea 2007 26(7):868-69.10.1097/ICO.0b013e31806c78bc17667625 [Google Scholar] [CrossRef] [PubMed]