Mental stress can be regarded as the disturbance in the mental balance of a person [1]. This is quite frequent in the case of students, where changes in daily routine, peer pressure, employment, social image and economic independence demand sudden increase in responsibility, introducing a drastic change in lifestyle and hence mental stress [2,3]. Students are seen to resort to dangerous practices such as alcohol abuse and drug abuse when the level of stress becomes very high [3]. If left unattended, stress can evolve into other psychological problems such as depression, Post-Traumatic Stress Disorder (PTSD), anxiety and suicide ideation [4].
Stress must be understood from the point-of-view of each person to come up with effective and personalised solutions [3]. Questionnaires and also physiological data such as Respiratory Rate (RR) and Electroencephalography (EEG) signals are used for quantification of stress [5-8]. Therapy is required when the student is unable to cope with stress on their own. Conventional methods are quite cumbersome, with these forms of therapies exposing the patients to life-threatening hazards [9,10]. Virtual Reality Therapy (VRT) is one such form of therapy that is showing itself as a potential workaround over these shortcomings. Virtual Reality, in short, is the illusion of living in reality virtually [11]. It aims to inoculate behavioral responses in the virtual world that are similar to those observed in the real world [12]. Virtual Reality has enhanced ecological validity due to its ability to mimic the real world nearly to perfection, greater control over the stimulus given to the user by the therapist, thus allowing for a better understanding of the effects, and also provide stimulus that could be almost impossible or life-endangering to do in the real world [12,13]. VRT also offers a high degree of immersion, with even relatively less-immersive approaches such as flat screen systems having enhanced ecological validity and effectiveness than traditional approaches as long as it is able to mimic the real world and respond well to user interaction [12]. Due to these advantages, VRT is commonly being seen used in the domains of Stroke rehabilitation, therapeutic application in Post-Traumatic Stress Disorders seen in war veterans, balance disorders, pain alleviation for burn victims, route learning of animals and humans, and also for understanding brain functioning during these various tasks by coupling them with techniques such as EEG and functional Magnetic Resonance Imaging [12-14]. Although popularity is being gained among the ranks of the medical community and an increase in the use of VR solutions in research studies, it is still far from widespread adoption due to the complex nature of the systems and their design and also due to insufficient clinical evidence obtained [13].
This study is aimed at adding to this ever increasing list, creating a simple, easy-to-use Virtual Reality Environment and testing it on participants, studying the effect of VRT in rehabilitation of mental stress using task performance metrics before and after therapy. This study also utilises the conceptualisation capacity of EEG waves, studying the variations in the mean band powers at various stages of the therapy to better understand the brain responses to the same. The various results are correlated to throw light on how effective the therapy was at mitigating the stress present in the participants. The study hypothesizes that Virtual Reality as rehabilitation aid will reduce the stress for both controls and experimental group.
Materials and Methods
Participant Selection: A total of sixty five final year students from the department of Biomedical Engineering were engaged in this study. The inclusion criteria were healthy, right-handed, and non-placed participants in their final year undergoing campus placements and want to work. This was due to the fact that there is an increased amount of stress due to the pressure of getting a job and also due to peer pressure. History of epileptic seizures was considered to be the exclusion criterion. The participants were filtered according to these criteria and a total of 25 participants were selected. Based on DASS-21 scores, these participants were segregated into two groups, the score of 14 was considered as normal (control) and the scores of 16 and above was measured as mildly stressed (experimental) [15]. Two participants opted to discontinue from the study while three participants displayed noisy EEG data, thus bringing down the final number to 20, equally split into the two groups (10 control + 10 experimental). The entire experiment was conducted in a soundproof room where the participants sat in comfortable seating arrangements. The experimental protocol was carried out for duration of approximately 30 minutes in accordance with the guidelines of the Institutional Ethics Committee for human volunteer research. The experiment was conducted after obtaining an informed consent from each of the participants, which gave them complete details about the experiment, their role in the same, and also guaranteed the safeguarding of their privacy, with the ability to withdraw from the study whenever they wanted to. Both the groups were exposed to Stroop Task to induce stress in the participants during the experimental protocol of this study.
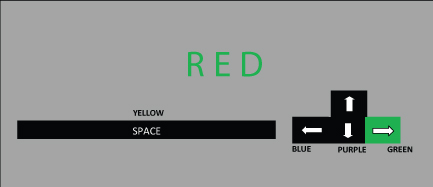
Stroop Task: The Stroop task consists of a set of words representing a variety of colours. Each word is coloured in either the same or different colour as the word. The user is tasked with describing the colour of the word and not the word itself [16]. For example, the word RED in the colour green must be described as GREEN and not RED. The study used a set of five colours, and had two different sets of stimuli. The congruent stimulus was the one where the word and the colour inscribed were the same, whereas the incongruent stimulus had one word and another colour. The task was created as a computer application via Psycho Pi using Python. The triggers were given via the computer screen and the participant responds to the triggers using a set of keyboard buttons. [Table/Fig-1,2] represent the Stroop incongruent (RED represented in Green colour) and congruent (RED represented in Red colour) stimuli respectively. The keyboard buttons used to respond were also depicted, with the green colour representing the correct response key to the corresponding stimulus.
Diagrammatic representation of the stroop task incongruent stimulus.
Diagrammatic representation of the stroop task congruent stimulus.

Task Stimuli: The task stimuli used for this study was a mathematical task Go-Nogo task. The visual stimuli were presented by pairs corresponding to trials. The first stimulus is an arithmetical equation and the second was an integer value. The first type of pair corresponded to the result of the equation described by the first stimulus being equal to the second stimulus and not equal to the same in the second type of pair. The subject was tasked with pressing the response button (in this study, the Enter button) as soon as possible for the first type pairs and ignoring the second type pairs. For each pair, the inter-stimulus interval was equal to 1100 ms, with the first stimulus lasting 400 ms and the second stimulus lasting 200 ms. The duration between two trials was equal to 3100 ms, with a total number of trials equal to 200 [17]. The parameters of performance were calculated for every condition separately. This was realised using the Psytask software.
Virtual Environment: The Virtual environment screen was developed to relieve the induced stress (by stroop task) during the experiment protocol. The environment set the stage for a peaceful surrounding wherein the user can relax and feel at peace.
The environment was created with the ability to stroll around in a forest-like environment, interact with elements and also listen to various natural sounds. This includes ability to walk or run around the environment, using a horse as mount to navigate [Table/Fig-3], colours that reflect nature, and also other human elements with whom dialogue can be established. Brightness of the screen was adjusted to the comfort of the user. To better improve the immersion of the environment, a soundproof room was used and kept dark.
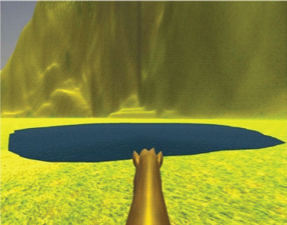
System Specifications: The VR Environment was displayed using a 15.6" laptop screen from a First Person Perspective. The gaze movements in the environment were seen in response to the movements in the mouse and interactions with various elements in the environment were possible with the help of a keyboard. The environment was created using the Unity 3D v5, a Gaming Engine used to build high-graphic 3-Dimensional content using JavaScript. The environment consisted of a Forest-like environment, with the user able to move as they please and also interact with the various elements present in it, for the entire duration of the therapy. The therapy was given in a dark, sound-proof room and contained ambient nature sounds to make the environment more immersive. The Electroencephalograph (EEG) signals measured during the same were recorded using the RMS SuperSpec with the 10-20 electrode setup. Task performances given before and after the therapy were mathematical tasks, deployed using the software PsyTask.
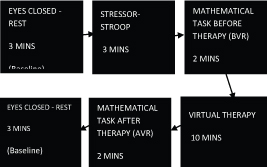
Experimental Protocol: At the start of the protocol, the participant is made to sit with their eyes closed for obtaining baseline and stabilising the signal. After three minutes of the same, the subject is induced stress using the Stroop task, performing the task for a total of three minutes. The subject is then made to perform the mathematical task for a total of two minutes, immediately after the induction of stress, thus allowing for a measure of their performance during a stressed state. They are then subjected to the Virtual Reality Environment for 10 minutes, allowing the subject to calm themselves. The subject then performs the mathematical task for another two minutes, measuring their performance during a relaxed state. Finally, the subject goes back to closing their eyes (baseline). The experimental protocol is depicted in [Table/Fig-4]. The experimental setup is depicted in [Table/Fig-5].
The EEG signals were recorded using the RMS SuperSpec software. The standard 10-20 Electrode Setup was used for EEG, with Ag/AgCl electrodes placed on the scalp in the prefrontal, frontal, central, temporal, occipital and parietal regions. Reference electrodes were placed in the earlobes and a ground electrode was also used. The electrodes were coupled via a paste for impedance matching. [Table/Fig-6] depicts the processing steps for EEG signals diagrammatically.
EEG processing and feature extraction.
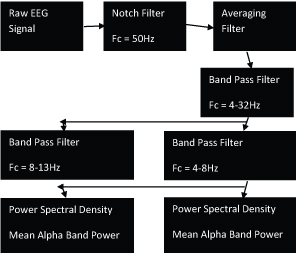
The raw EEG signals (sampling frequency of 256Hz) obtained were restricted to a band of 4-32Hz, with the delta waves (0.1-4Hz) filtered using a band-pass filter (Fc = 4Hz-32Hz) to remove any eye blink artifacts. The signal was passed through a moving average filter using a triangular window (half-width of 30) to improve the signal-to-noise ratio. A notch filter (Fc = 50Hz) was used to remove any power-line interference. The filtered signal was then split into the respective bands- theta (Band Pass Filter, Fc = 4-8Hz) and alpha (Band Pass Filter, Fc = 8-13Hz). Beta bands were not taken into consideration, as alpha waves and theta waves were more constant in their changes to stressful conditions and thus better indicators of stress [18,19]. Power Spectral Density (PSD) of the separated bands were calculated and used for further statistical analysis.
The Mann-Whitney U-Test was used for independent sample analysis of the DASS scores between the Normal and Mildly Stressed Groups, and the Posthoc Wilcoxon Signed-Rank Test was used for related sample analysis of EEG and Task Performance during Rest (baseline), Task before therapy and Task after therapy. The significance values (p) were measured with a threshold of 0.05. The mean and standard errors of the significant samples were taken for further graphical representation.
Results
The experiment was conducted on a sample pool consisting of 65 final year non-placed students from the department of Biomedical Engineering. A sample size of 25 was calculated with an error margin of 15%, with two discontinuations and three noisy data giving a final list of 20, which was segregated into two equal groups- control and experimental.
In the Stroop Task, the percentage of correct answers for incongruent stimuli was 95.87% for control and 92.87% for experimental group while the percentage of wrong answers for control group was 4.1% and 7.3% for experimental group. The response time for incongruent stimuli was 1225ms for the control group and 1596ms for the experimental group.
The percentage of correct answers for congruent stimuli was 97.58% for control group whereas its 97.24% for experimental group. While, the percentage of wrong answers for control group was 2.42% and 2.76% for experimental group. For congruent stimuli, the response time was 1120ms and 1394ms for the control and experimental group respectively.
This is in line with the Stroop interference effect, with increased response time in both groups for incongruent stimuli than congruent stimuli [16]. This is further substantiated by the percentage of wrong answers, both groups able to find it easier to answer congruent than incongruent stimuli. The control group had increased correct and decreased wrong answer percentages than experimental group for both types of stimuli, suggesting an introduction of stress which caused a reduction in performance. Normal group was able to cope with the stress due to their inherent ability to do so, which was not seen in the stressed participants [3].
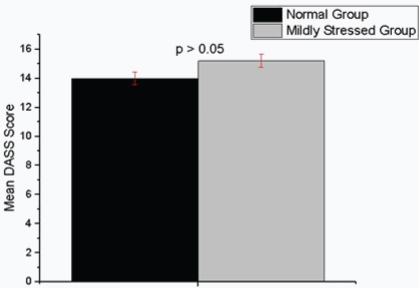
As can be seen in [Table/Fig-7], there is no statistically significant difference between the Normal and the Mildly Stressed Group (p>0.05). The score of 14 was considered as Normal (control) and the scores above 14 were measured as mildly stressed (experimental) [15].
DASS scores-Control vs Experimental Group.
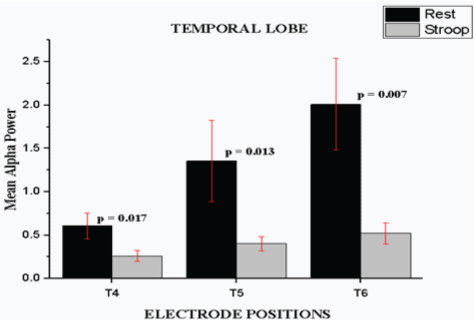
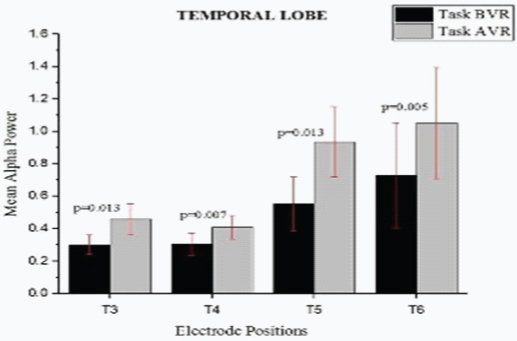
For the normal group, there were statistically significant changes in the mean Alpha Band Powers between Rest and Stressor (Stroop Task) in the temporal region electrodes T4 (p=0.017), T5 (p=0.013) and T6 (p=0.007) with a reduction in the mean band power [Table/Fig-8a] and also between the tasks performed before and after therapy in the temporal region electrodes T3 (p=0.013), T4 (p=0.007), T5 (p=0.013) and T6 (p=0.005) with an increase in mean band power [Table/Fig-8b].
Mean Alpha Power for Control Group- Rest vs Stroop.
Mean Alpha Power for Normal Group-BVR vs AVR.
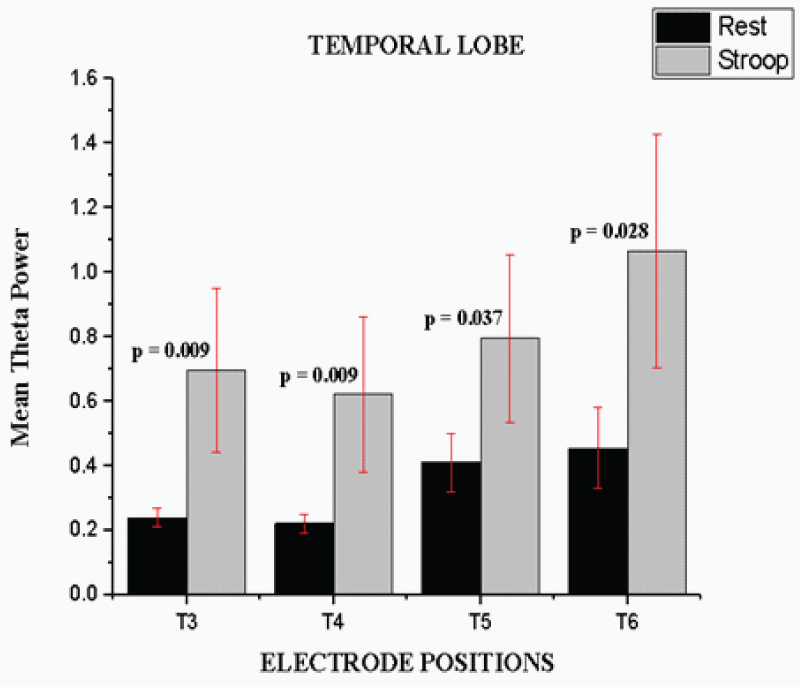
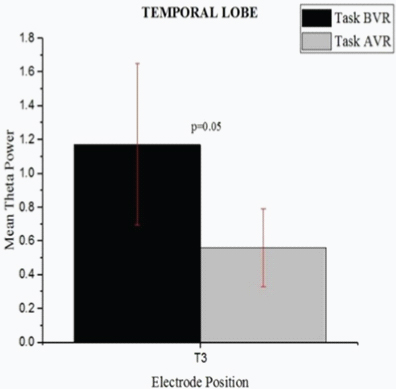
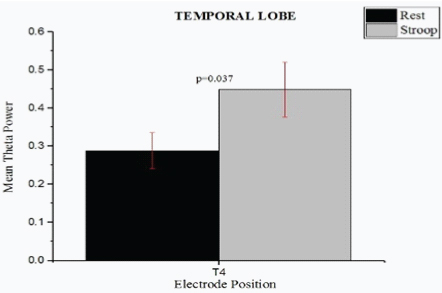
Statistically significant changes were also seen in the mean Theta Band Powers across the temporal region electrodes T3 (p=0.009), T4 (p=0.009), T5 (p=0.037) and T6 (p=0.028) between Rest and Stressor (Stroop Task) with an increase in the mean band powers [Table/Fig-8c] and in the temporal region electrode T6 (p=0.05) between the tasks performed before and after therapy with a decrease in the mean band powers [Table/Fig-8d].
Mean Theta Power for Normal Group- Rest vs Stroop.
Mean Theta Power for Normal Group- BVR vs AVR.
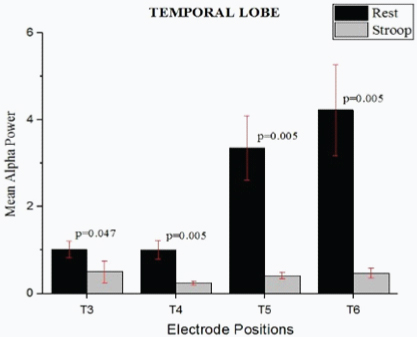
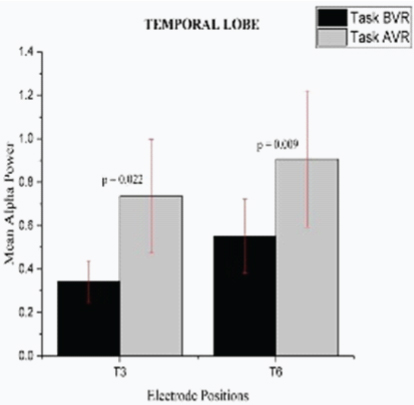
For the Mildly Stressed Group, there were statistically significant changes in the mean Alpha Band Powers between Rest and Stressor (Stroop Task) in the temporal region electrodes T3 (p=0.047), T4 (p=0.005), T5 (p=0.005) and T6 (p=0.005) with a reduction in the mean band power [Table/Fig-9a] and in the temporal region electrodes T3 (p=0.022) and T6 (p=0.009) between the tasks performed before and after therapy with an increase in the mean band power [Table/Fig-9b].
Mean Alpha Power for Mildly Stressed Group- Rest vs Stroop.
Mean Alpha Power for Mildly Stressed Group- BVR vs AVR.
Statistically significant changes were also seen in the mean Theta Band Powers across the temporal region electrode T4 (p=0.037) between Rest and Stressor (Stroop Task) with an increase in the mean band power [Table/Fig-9c] but no statistically significant changes were seen between the tasks performed before and after therapy (p>0.05).
Mean Theta power for mildly stressed group- Rest vs Stroop.
No statistically significant changes were seen between normal and Mildly Stressed Groups.
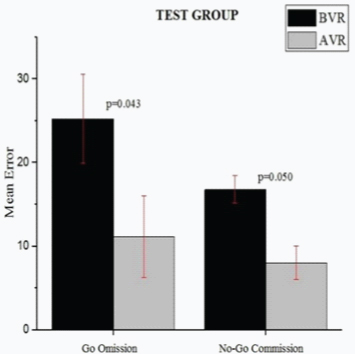
In the Normal Group, there weren’t any statistically significant difference in the Go Omission and No-Go Commission Errors (p>0.05) [Table/Fig-10a]. This was in contrast to the Mildly Stressed Group, which showed statistically significant changes in the Go Omission (p=0.043) and No-Go Commission Errors (p=0.05, [Table/Fig-10b]) between the tasks performed before (BVR) and after therapy (AVR) with a huge drop in these values. No statistically significant changes were seen between normal and mildly stressed groups.
Task Performance Metrics for Control Group-BVR vs AVR.

Task performance metrics for mildly stressed group-BVR vs AVR.
Discussion
Virtual Reality-based rehabilitation therapy is widely used for stroke recovery and an attempt is made to use this technique to reduce the mental stress encountered in young adults. Based on the DASS Scores, the participants are divided into control and experimental group and the same VR environment employed. Thus, further discussions will involve in analysing trends seen in each group. The participants are positioned in a more naturalistic virtual environment for safe navigation.
Task performance was improved in the Mildly Stressed Group after therapy, with a decrease in their percentage of Omission for Go trials and percentage of Commission for No-Go trials. This was in line with the findings that Virtual Reality-based rehabilitation is seen to have a positive impact, with studies done on Stroke, ADHD, Amnesia, and TBI showing increased task performance after various sessions of VRT [20]. The same cannot be said for the Control group, which showed no statistically significant changes in these values. Normal people can easily cope with stress and have a higher threshold than stressed people [3]. This could possibly be the reason for there being no change in the Task Performance metrics in the Control group before and after therapy.
This trend in cognitive functioning can further be supported by the results obtained from the EEG. When we consider the EEG band powers of alpha and theta, a reduction in alpha band power and an increase in the theta band power are correlated to an increase in stress levels, with the converse also holding true [18,19]. This is because Alpha waves are usually related to a state of calmness while theta waves are usually related to stressful thinking and disappointment [7]. When we consider the results obtained from EEG, there is a significant reduction in the alpha band powers and an increase in mean theta band powers for both the Normal and Mildly Stressed Group from Rest to Stressor (Stroop Task), indicating an increase in stress levels. While there was an increase and decrease in the mean alpha band power and mean theta band power respectively from the task performed before therapy to that after therapy for the Control group, indicating the introduction of calmness by the therapy in the participants, the Mildly Stressed Group showed statistically significant change only in the mean alpha band power from the task performed before therapy to that after therapy. This could probably be due to the smaller sample size considered. Furthermore, these changes are seen across the electrodes T3, T4, T5, and T6 in the Temporal Region, which are considered to relate to cognitive functions such as attention to colour and shape, true and false memory recognition, visual fixation and memory (Brodmann Areas 42, 21, 37) [19]. No changes were observed in the rest of the lobes. Thus, the therapy was able to improve cognitive functioning in the two groups, increasing their Alpha Band Power, decreasing their Theta Band Power and hence reflecting on their Task Performance results.
While intra-group variations in the parameters measured were seen, no inter-group variation was seen in the study. This can be attributed to the lack of any statistically significant change between the DASS scores of the two groups. This could possibly indicate the two groups not having too much of a variation in terms of their stress levels. Though the study showed an improvement in cognitive functioning and reduction in stress levels in each group, these could not be compared between the two groups used in the study. Thus no conclusive evidence regarding the relative extent of stress reduction in the stressed group with respect to the control group could be obtained. While one of the reasons could be due to the overlapping of the DASS scores in both groups (as stated before) and also the lower number of samples, another reason could be due to the Virtual Environment not tailored to the preferences of each participant. Thus, while the environment could be efficient to certain users, it could be inconsequential in stress reduction in others. Addition of an audio stimulus in the form of music could also improve the efficiency of the VRT, making the environment an audio-visual stimulus.
Conclusion
Results indicate a therapeutic effect introduced by Virtual Reality Therapy in the Normal and Mildly Stressed Groups. The hypothesis could not be proved i.e., inter-group variations were not seen potentially due to the Normal and Mildly Stressed Groups not being very different, due to the Virtual Environment being created not considering preferences of the participants and also due to relatively high margin of error (15%). By increasing the sample size (thus decreasing margin of error), choosing Severely Stressed participants instead of Mildly Stressed participants or creating a Virtual Environment tailored to the users’ preferences with additional audio stimuli, one can perform inter-group analysis of these parameters and further substantiate the effects of VRT in stress reduction.