The prevalence of vitamin D deficiency is rising worldwide. Populations living in tropical countries with abundant of sunlight are also affected by this problem [1,2]. It is a major medical concern due to the pleiotropic effects of vitamin D in maintaining optimal health [3]. Vitamin D plays an important role in determining optimal maternal and foetal health outcomes. In pregnant women, low vitamin D level had been linked to increased risk for pre-eclampsia, gestational diabetes mellitus, bacterial vaginosis, preterm birth and Small-for-Gestational-Age (SGA) newborns [4]. Health consequences of suboptimal vitamin D levels among women at early pregnancy are debatable. Leffelaar ER et al., observed that women with low vitamin D level during early pregnancy (12 to 14 weeks) gave birth to infants with low birth weight and increased risk for SGA [5]. In contrast, Ates S et al., showed that there was no significant relationship between low serum 25-hydroxyvitamin D at 11-14 weeks of gestation and adverse pregnancy outcome [6]. If such relationship exists, early intervention can be implemented to avoid adverse pregnancy outcomes by identifying and treating the women with vitamin D deficiency in the early pregnancy.
Vitamin D can be synthesised endogenously or obtained exogenously. The endogenous vitamin D synthesised cutaneously serves as the main source of vitamin D. The cutaneous synthesis of vitamin D is initiated by Ultra Violet B rays (UVB) from the sunlight. This process is influenced by the amount of the skin exposed to the sun, skin pigmentation and the use of sun protection (shade and sunscreen) [7,8]. On the other hand, exogenous vitamin D can be found in fortified food such as milk, margarine, cereal and sardine, as well as supplements. In Malaysia, the recommended vitamin D intake for pregnant women is 200 IU/day to ensure adequate absorption of calcium [9].
The common risk factors for vitamin D deficiency are dark skin pigmentation, lack of sun exposure, extensive clothing, old age, obesity and malabsorptive syndrome [10]. Bukhary NBI et al., showed that Malays and Indians were more susceptible to vitamin D deficiency compared to Chinese due to high sun protection score and high skin pigmentation [11]. Daily intake of food that have high vitamin D content help to reduce vitamin D deficiency problem [11]. Ates S et al., indicated that women with covered attire were at risk for vitamin D deficiency due to the lack of sun exposure [6]. The use of multivitamins containing vitamin D has been shown to increase vitamin D levels in women [6,12].
This pilot study aimed to determine the prevalence of vitamin D deficiency in Malaysian women at early pregnancy (11-16 weeks gestation) and the associated risk factors. Similar studies have been conducted in Malaysia excluding those co-morbidities such as diabetes mellitus, asthma, hypertension and chronic kidney disease [11]. This could artificially lower the prevalence of vitamin D deficiency. In this study, it was hypothesised that the prevalence of vitamin D deficiency in Malaysian women at early pregnancy was high. This was associated with common risk factors aforementioned. It was also assumed that pregnant women taking supplements containing vitamin D would have higher daily vitamin D intake and a higher circulating vitamin D level. It is hoped that this study would identify the extent of vitamin D deficiency in Malaysian women at early pregnancy and ways to identify them to enable early intervention.
Materials and Methods
This was a descriptive cross-sectional study carried out in a tertiary medical institution in Kuala Lumpur, Malaysia. Sample size calculation was performed using the formula based on prevalence of vitamin D deficiency using L-Kish formula. The inputs used were Z (value found in statistical tables which contain the area under the normal curve)=1.96, e (acceptable sampling error)=0.08, p (estimated proportion of an attribute that is present in the population)=0.9 (90% of pregnant women in the study of Bukhary NBI et al., had vitamin D deficiency). A total of 57 pregnant women at early pregnancy were selected fulfilling the minimum sample size number for pilot study. These women were recruited from the obstetrics and gynaecology clinic, wards and outpatient clinic of the institution from March 2017 until August 2017. The subjects provided written informed consent to participate in this study and the study protocol was reviewed and approved by Universiti Kebangsaan Malaysia Research Ethics Committee (ref code: UKM FPR.4/244/FF-2017-114). The study was conducted in accordance with Declaration of Helsinki.
The inclusion criteria were gestation period up to 16 weeks, the age of the mother ranged from 19 to 40-years-old and singleton pregnancy. Meanwhile, the exclusion criteria were multiple pregnancies, and pregnant women that were prescribed with drugs affecting vitamin D metabolism (anti-epileptics, anti-tuberculotics, statins, glucocorticoids). Patients fulfilling the criteria were explained about the study. After obtaining informed consent, the patient completed physician-guided questionnaire. This is a face-to-face interview as the patients were required to fill in information regarding socio-demographic information (age, ethnicity, occupation), clinical data (height, weight, BMI, gestational age, parity, gravidity, problem in previous pregnancy, maternal co-morbidities) and a validated food frequency questionnaire for vitamin D intake. Skin colour of respondents was assessed using Fitzpatrick skin classification. They were classified based on skin colour scheme: skin type I (pale, white skin), skin type II (white skin), skin type III (light brown skin), skin type IV (moderate brown skin), skin type V (dark brown skin), and skin type VI (black skin). Also, inquiries and information pertaining to sun protection was obtained from the respondents which included the use of sunblock lotion, hijab, cap/hat, long sleeve shirt, gloves, long pants, long skirt and umbrella. Data regarding length of time exposed to sunlight were obtained by multiplying sunlight exposure in minutes per day with exposure in days per week.
Dietary Assessment: The dietary intake of the respondents was assessed by using a seven-day dietary recall method. The food frequency questionnaire for vitamin D intake was divided into several parts which consisted of fortified food (dairy products, cereal, others), natural food (seafood, meat, egg product, mushroom) as well as dietary supplements (vitamin for pregnant mother and other additional supplements). Atlas of food exchange and portion size was used to help to quantify food portion size in order to calculate total dietary intake of vitamin D among the respondents in a day (IU/day). U.S. Department of Agriculture (USDA) food database was used to calculate the amount of vitamin D in each food [13]. The food frequency questionnaire for vitamin D intake has been validated for use in Malaysian population [9].
25-Hydroxyvitamin D Analysis: Venous blood sample (10 ml) was collected using plain tubes from the pregnant women in their first 16 weeks of pregnancy. The blood was centrifuged at 3500 rpm for 10 min at 4°C (Eppendorf Centrifuge 5804R, Hamburg, Germany) to extract the serum. The serum was then stored at -80°C until analysis. The determination of 25-hydroxyvitamin D (25(OH)D) level was conducted using enzyme-linked immunosorbent assay following manufacturer’s protocols (IDS, Tyne & Wear, UK). The subjects were classified based on their serum 25-hydroxyvitamin D level into several groups, which are severe vitamin D deficiency (<25 nmol/L), mild vitamin D deficiency (25-49 nmol/L), vitamin D insufficiency (50-74 nmol/L) and vitamin D sufficiency (≥75 nmol/L) [11,12].
Statistical Analysis
The research data were analysed by using Statistical Software for Social Sciences version 24.0 (IBM, Armonk, USA). The general characteristics of the respondents were described in mean±standard deviation, percentage (%) and mean (minimum, maximum). Chi-squared test and Spearman correlation test were used to determine the association between risk factors of interest and vitamin D status of the subjects. The association between dietary components and total daily vitamin D intake was performed using chi-squared test. The results were considered significant when the p-value was <0.05.
Results
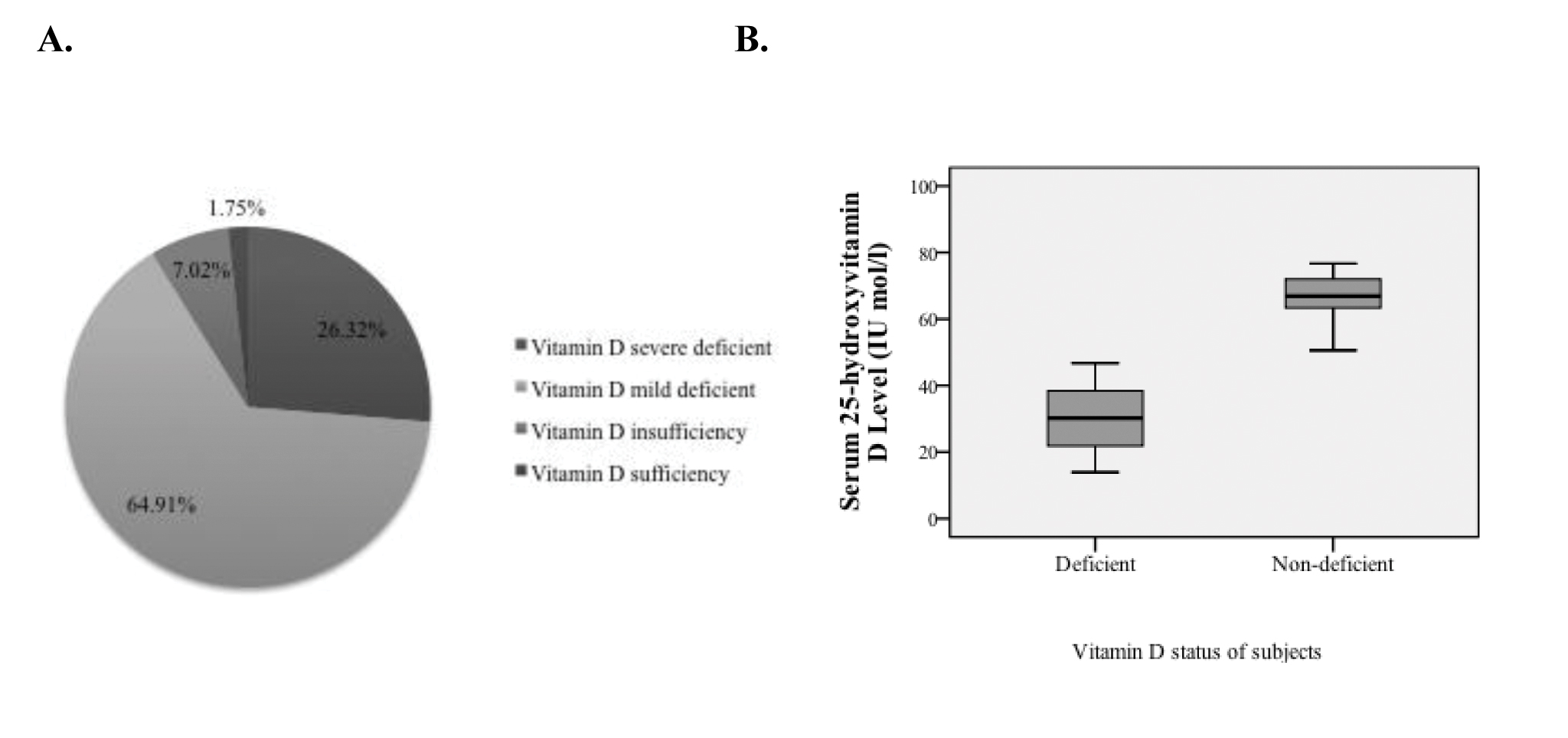
A total of 57 pregnant women at early pregnancy aged 18-40 years (mean 32.88±4.52 years) were recruited for the study. Of these respondents, 85.96% were Malay and 14.04% were non-Malay. Majority of our respondents were employed (78.95%), non-healthcare provider (80.7%) and working indoor (96.49%). It was observed that 42.11% of the respondents had co-morbidities such as diabetes mellitus, asthma, hypertension and chronic kidney disease. Only 52.63% of the subjects met the Recommended Nutrient Intake (RNI) of vitamin D for Malaysia (>200 IU/day). The prevalence of vitamin D deficiency (serum 25(OH)D <50 nmol/L) was 91.23% among our respondents. Among those with vitamin D deficiency, 26.32 % suffered from severe vitamin D deficiency (serum 25(OH)D <25 nmol/L) and 64.91% had mild vitamin D deficiency (serum 25(OH)D 25-49 nmol/L) [Table/Fig-1].
Basic characteristics of the subjects.
| Independent variables | n | Percentage (%) |
|---|
| A) Sociodemographic data |
| Age (mean±standard deviation) (year) | | 32.88±4.52 |
| Ethnicity-Malay-Non-Malay | 498 | 85.9614.04 |
| Working status-Working -Not-working | 4512 | 78.9521.05 |
| Occupation-Healthcare provider -Non-healthcare provider | 1146 | 19.3080.70 |
| Work environment -Indoor-Outdoor | 552 | 96.493.51 |
| B) Clinical Data |
| Pre-pregnancy BMI (kg/m2)-Normal-Overweight -Obese | 181920 | 31.5833.3335.09 |
| Antenatal BMI (kg/m2)-Normal -Overweight -Obese | 181821 | 31.5831.5836.84 |
| Gravidity {Mean (Min, Max)} | | 2 (1,8) |
| Parity {Mean (Min, Max)} | | 1 (0,6) |
| Maternal co-morbidity-With co-morbidity-Without co-morbidity | 2433 | 42.1157.89 |
| C) Dietary |
| Dairy product and fish-Taking-Not taking | 2730 | 47.3752.63 |
| Supplement with vitamin D-Taking-Not taking | 1938 | 33.3366.67 |
| Vitamin D daily intake (IU/day)<200≥200 | 3027 | 52.6347.37 |
| D) Factors related to skin |
| Skin colour by using Fitzpatrick classification-Type I-II-Type III-VI | 3027 | 52.6347.37 |
| Dressing style-Covered (score ≥4)-Uncovered (score <4) | 3720 | 64.9135.09 |
| E) Sun exposure (mean±SD) (min/week) | | 197.54±225.62 |
| -Vitamin D status |
| F)Vitamin D (25-OHD) status-Deficient (<50 nmol/L)-Non-deficient (≥50 nmol/L) | 525 | 91.238.77 |
| G)Vitamin D deficiency sub-class-Severe deficient (<25 nmol/L)-Mild deficient (25-49.99 nmol/L) | 1537 | 26.3264.91 |
[Table/Fig-2] showed the boxplot of vitamin D distribution of our respondents. The median of serum 25(OH)D for vitamin D deficient and non-deficient was 30.19 nmol/L and 66.85 nmol/L respectively. The minimum and maximum value of serum 25(OH)D level for vitamin D deficiency was 13.91 nmol/L and 46.69 nmol/L respectively. Meanwhile, for vitamin D non-deficient, the minimum value was 50.60 nmol/L and the maximum value was 76.70 nmol/L.
A. Pie chart on distribution of patients with the known vitamin D status; and B. Box plot that showed median, minimum and maximum value of serum vitamin D level (nmol/L) of Vitamin D deficient and non-deficient.
The associations between vitamin D status (deficient vs non-deficient) and characteristics of the subjects as well as risk factors of interest were shown in [Table/Fig-3]. Generally, the associations between vitamin D status and characteristics examined were not significant (p<0.05). Statistically near significant relationship were detected between vitamin D status and dairy or fish intake (p=0.08), and duration of sun exposure (p=0.09).
Association between sociodemographic, clinical data, risk factors and vitamin D status in women at early pregnancy.
| Variable | Serum 25-OHD <50 nmol/L n (%)Mean±SDMedian(IQR) | Serum 25-OHD ≥50 nmol/L n (%)Mean±SDMedian(IQR) | p-value |
|---|
| Ethnic | Malay | 46 (93.88) | 3 (6.12) | 0.28a |
| Non-Malay | 6 (75.00) | 2 (25.00) |
| Working status | Non-working | 11 (91.67) | 1 (8.33) | 1.00a |
| Working | 41 (91.11) | 4 (8.89) |
| Working Environment | Indoor | 50 (90.91) | 5 (9.09) | 1.00a |
| Outdoor | 2 (100.00) | 0 (0.00) |
| Pre-pregnancy BMI | Obese | 18 (90.00) | 2 (10.00) | 1.00a |
| Non-Obese | 34 (91.89) | 3 (8.11) |
| Gestational | 11.27±2.658 | 11.20±2.387 | 0.96b |
| Gravidity | 1(1,3) (min=1, max=8) | 1 (1,3) (min=1, max=7) | 0.809b |
| Parity | Nulliparous | 21 (91.30) | 2 (8.70) | 1.00a |
| Multiparous | 31 (91.18) | 3 (8.82) |
| Maternal comorbidity | Without comorbidity | 31 (93.94) | 2 (6.06) | 0.71a |
| With comorbidity | 21 (87.50) | 3 (12.50) |
| Vitamin D dietary intake per day (IU/day) | <200 | 28 (93.3) | 2 (6.7) | 0.90a |
| ≥200 | 24 (88.9) | 3 (11.1) |
| Dairy product & Fish | No | 25 (83.33) | 5 (16.67) | 0.08a |
| Yes | 27 (100.00) | 0 (0.00) |
| Supplement with vitamin D | No | 33 (86.8) | 5 (13.2) | 0.25a |
| Yes | 19 (100.0) | 0(0.0) |
| Skin colour by using Fitzpatrick classification | Class I-II | 26 (86.7) | 4 (13.3) | 0.42a |
| Class III-VI | 26 (96.3) | 1(3.7) |
| Dressing style | Covered (score ≥4) | 32 (86.5) | 5(13.5) | 0.22a |
| Uncovered (score <4) | 20 (100.0) | 0 (0.0) |
| Duration of sun exposure (min/week) | 70 (0,245) | 420 (5,420) | 0.09c |
a p-value obtained from Yates-corrected chi-squared test
b p-value obtained from independent sample t-test
c p-value obtained from Spearman’s correlation test
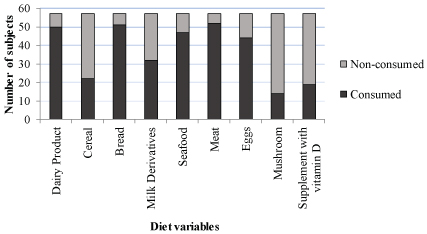
The dietary survey indicated that dairy product and meat were major sources of vitamin D in the subjects [Table/Fig-4]. Analysis of daily vitamin D intake status and dietary components revealed no significant relationship (p>0.05) [Table/Fig-5]. Only the use of vitamin D supplement was associated with sufficient daily vitamin D intake (p<0.001). However, no significant association was found between daily dietary intake of vitamin D status and vitamin D status based on serum 25(OH)D (p>0.05).
Consumption of dietary intake of vitamin D among pregnant women at early pregnancy.
Vitamin D intake in IU per day according to diet variables.
| Variables | IU Intake per day | p-value |
|---|
| <200 (n=30)n (%) | >200 (n=27)n (%) |
|---|
| Dairy product | No | 5 (16.7) | 2 (7.4) | 0.510a |
| Yes | 25 (83.3) | 25 (92.6) |
| Cereal | No | 20 (66.7) | 15 (55.6) | 0.390b |
| Yes | 10 (33.3) | 12 (44.4) |
| Bread | No | 2 (6.7) | 4 (14.8) | 0.570a |
| Yes | 28 (93.3) | 23 (85.2) |
| Milk derivatives | No | 15 (50.0) | 10(37.0) | 0.325b |
| Yes | 15 (50.0) | 17 (63.0) |
| Seafood | No | 5 (16.7) | 5 (18.5) | 1.000a |
| Yes | 25 (83.3) | 22 (81.5) |
| Meat | No | 1 (3.3) | 4 (14.8) | 0.289a |
| Yes | 29 (96.7) | 23 (85.2) |
| Eggs | No | 6 (20.0) | 7 (25.9) | 0.594b |
| Yes | 24 (80.0) | 20 (74.1) |
| Mushrooms | No | 23 (76.7) | 20 (74.1) | 0.820b |
| Yes | 7 (23.3) | 7 (25.9) |
| Supplement with vitamin D | No | 28 (93.3) | 10 (37.0) | <0.001b |
| Yes | 2 (6.7) | 17 (63.0) |
IU = International Units
a p-value obtained from Yates-corrected chi-squared test
b p-value obtained from the chi-squared test
Discussion
The current study showed that a substantial proportion of the women at early pregnancy were suffering from vitamin D deficiency (91.23%; serum 25(OH)D<50 nmol/L), of which more than half had mild deficiency (64.91%; serum 25(OH)D 25-49 nmol/L) and the rest had severe deficiency. Although Malaysia is a tropical country receiving abundant sunlight throughout the year, the high prevalence of vitamin D deficiency is surprisingly common. A previous study conducted in Malaysia revealed that the prevalence of vitamin D deficiency was 90.4% in the pregnant women at first trimester (n=358), whereby 43.9% and 46.5% had severe and mild vitamin D deficiency respectively [11]. This was similar with the prevalence observed in this study, whereby 91.23% women in the first trimester were found to be deficient in vitamin D. Jan Mohamed HJ et al., reported a lower prevalence of deficiency among pregnant women at second and third trimester, which was 59.8% (n=61) and 37.3% (n=38) respectively [12]. The reason for this discrepancy might be due to the different location where it was carried out. The previous study was performed in a suburban region of northern Malaysia, while the subjects of this study were recruited from the central urban region of Malaysia.
In this study, no association between ethnicity and vitamin D status was found. This was in contrast with previous studies performed in Malaysia, whereby a higher prevalence of vitamin D sufficiency was found in Chinese women compared with Malay and Indian women [2,14,15]. Bukhary NBI et al., found that Malay and Indian pregnant mothers in their first trimester had 34 times and 17 times higher risk of developing vitamin D deficiency respectively compared to their Chinese counterparts due to darker skin pigmentation and higher sun protection [11]. Among non-pregnant women, a higher plasma 25(OH)D level was found in Chinese (58 nmol/L) compared to Malay (43 nmol/L) and Indian (45 nmol/L) subjects [14]. Similarly, Man RE et al., showed that vitamin D deficiency was more common among Indian adult men (84.3%), followed by Malay (84.1%) and Chinese (52.3%) in Malaysia [15]. In accordance with the results of ethnicity, skin pigmentation classification according to Fitzpatrick scheme was not associated with vitamin D status among the subjects of this study. Theoretically, melanin in the skin competes with 7-dehydrocholesterol to absorb UVB, thereby attenuating the production of 25(OH)D [16]. The use of sun protection could eliminate the difference between subjects with different skin pigmentations.
Indoor occupations like healthcare workers were associated with high prevalence of vitamin D deficiency [17]. Sharma N et al., reported that housewives suffered from more severe vitamin D deficiency compared to working women probably they spent more time indoor [18]. However, there was no significant association between working status and vitamin D status in the current study (p=1.00). This could be caused by the high sun avoidance tendency among working women. The similar findings were obtained in Malaysian men, whereby no significant relationship was found between outdoor work and circulating vitamin D concentration [15].
Ates S et al., and Bukhary NBI et al., demonstrated a significant association between the style of attire and vitamin D status [6,11]. The subjects in this study were predominantly Malay Muslims who adopted a covered attire style. Traditionally, this comprises a headscarf and long dresses that leave only face and hands exposed [14,15]. This could contribute to vitamin D deficiency due to the lack of sun exposure [6]. However, no significant association was discovered between attire style and vitamin D status in the current study, may be because the effects of sun avoidance behaviour was greater than the attire.
Previous studies had shown that individuals with higher Body Mass Index (BMI) had lower serum 25(OH)D level [15,19]. This is due to sequestration of 25(OH)D by the adipose tissue, thereby reducing its circulating level. No significant association between maternal BMI and serum vitamin D concentration was found in this study. Considering the mean BMI of the subjects in this study was 25.67±4.93 kg/m2, they were not very obese and the effects of adipose tissue on circulating 25(OH)D level was minimal.
Dairy products and oily fish are rich sources of vitamin D [19-21]. However, all subjects from this study who consumed dairy products and fish had vitamin D deficiency. This might be due to active consumption of dairy products and fish among women with the knowledge that they had poorer health due to vitamin D deficiency [22,23]. The cross-sectional design of this study could not resolve the causal relationship between dietary intake and vitamin D deficiency.
Charatcharoenwitthaya N et al., that supplementation of 400 IU/day vitamin D levels in the first trimester is sufficient to maintain adequate vitamin D throughout pregnancy in women with adequate and mild deficiency [24]. However, in severe deficiency even at a higher dosage of 800 IU/day was not sufficient to obtain an adequate level of vitamin D throughout pregnancy in 20% of women. Multivitamin and dairy products are major sources of dietary vitamin D as illustrated by previous studies [6,12]. However, the bioavailability of vitamin D varies due to the difference in individual absorption, tissue deposition and catabolism. This would explain the absence of a significant relationship between daily dietary vitamin D intake and circulating 25(OH)D level.
Malaysian women, like most Asian populations, value the aesthetic value of fair skin [15]. Therefore, the Malaysian women limit their time outdoors and exposure to sunlight. The time spent per week for sunlight exposure for subjects in the current study was 70 minutes. This was well below the recommended sunlight exposure to maintain optimum vitamin D status, which is 140 minutes per week [20]. The association between time of sunlight exposure and circulating vitamin D level was close to statistical significance (p=0.09).
Limitation
Firstly, the sample size of this study was small. This was a single centre study in an urbanised region of Malaysia, thus it might not be representative of the whole Malaysia. We did not calculate the melanin index and sun protection score for our subjects. Measurement of serum 25(OH)D level was performed using ELISA assays instead the more reliable high-performance liquid chromatography-mass spectrometry due to technical limitations. Due to cross-sectional nature of this study, causal relationship between risk factor of interest and vitamin D deficiency could not be firmly established.
Conclusion
Vitamin D deficiency is prevalent among Malaysian women at early pregnancy. This may be associated with the lack of sunlight exposure but a larger study is required to validate this speculation. Supplement is the most important source of dietary vitamin D in these women. However, the dose needs to be adjusted so that it can improve circulating 25(OH)D level. Vitamin D screening at early pregnancy should be implemented to identify women at risk and allow early intervention.
a p-value obtained from Yates-corrected chi-squared test
b p-value obtained from independent sample t-test
c p-value obtained from Spearman’s correlation test
IU = International Units
a p-value obtained from Yates-corrected chi-squared test
b p-value obtained from the chi-squared test