Air Pollution
Earth’s atmosphere is a complex natural gaseous system essential for support of life. Due to rapid urbanisation our earth’s ecosystem is under threat. Polluted area (caused due to usage of more and more vehicles), biological materials and other harmful substances released into atmosphere causes damage to food crops, diseases and death in humans [1]. It has become a major problem that is affecting millions of people worldwide. WHO estimated that air pollution is known to cause death of 2.4 million people per year.
Indoor air pollution and urban air quality are listed as two of the world’s worst poisonous pollution problems in the 2008 Blacksmith Institute, World’s Worst Polluted Places report [2]. There are many causes for air pollution but generally classified as gaseous and particulate pollutants. Gaseous pollutants include Sulphur Dioxide (SO2), Nitrogen Oxides (NO2), Ozone (O3), Carbon Monoxide (CO), Volatile Organic Compounds (VOC), Hydrogen Sulphide (H2S), Hydrogen Fluoride (HF), and various gaseous forms of metals which are emitted from fossil fuel, fired power plants, smelters, industrial boilers, petroleum refineries, and manufacturing facilities. This may cause damage to natural resources which ultimately leads injury to ecosystems, organisms and respiratory diseases in human [3,4]. Particulate pollutants come both in large and small/fine forms. Larger ones include dust, asbestos fibres, and lead. Finer ones include sulfates (SO4) and nitrates (NO3). Main sources of these pollutants are automobile industries, mining operations, power plants, etc. These particulates pollute the air which leads to potential health problems especially to those individuals who work in these industries and who are exposed to dust for a longer time [5]. Particulate pollutants are classified as primary and secondary pollutants. Primary ones are emitted directly into the air from pollution sources. Major primary pollutants produced by human activities include SO2, NO2, O3, CO and VOC. Secondary ones are produced when primary pollutants undergo chemical changes in the atmosphere. Example for secondary pollutant is O3. It is formed when NO2 and VOCs are assorted and warmed by sunlight. O3 is a major component of smog. O3 present in the troposphere/atmosphere is close to the ground, should not be confused with beneficial ozone that is located in the stratosphere/ atmosphere. This beneficial ozone protects the earth from harmful ultraviolet light [6].
Sources of air pollution: There are various factors responsible for releasing pollutants into the atmosphere. These sources can be classified into two categories: Anthropogenic/man-made sources and Natural sources. Man made sources are smoke stacks of power plants, waste incineration and biomass used for cooking in developing and poor countries [7]. Natural sources like large areas with few or no vegetation, methane, emitted by the digestion of food by animals e.g., cattle [8].
Percentage of Population Exposed to Air Pollution: Air pollution can affect any one, but those who are suffering from lung, heart diseases and old age are more likely to be affected. Pollutants aggravate the symptoms of asthma in old people because of weak immune system [9].
Health Effects Associated with Exposure to Air Pollution: Air pollution leads to changes in respiratory and cardiovascular functions, clinical symptoms, outpatient and emergency room visits, hospital admissions and finally premature death. However, the number of people affected worldwide is quite significant. Epidemiological studies using sophisticated statistical tools have shown that risk of air pollution related to health seems to be relatively low. In other words, even when the WHO 2000 air quality guidelines are met, the increased health risk still exists [1,9]. Chronic exposure to air pollution is a significant risk factor for a number of health conditions including respiratory infections, Chronic Obstructive Pulmonary Disease (COPD), stroke and lung cancer. Health effects are difficulty in breathing, wheezing, coughing, asthma and worsening of existing respiratory and cardiac conditions [1].
According to WHO report, indoor air pollution is the 10th preventable risk factor. Although many people think of air pollution as an outdoor urban phenomenon, some of the highest concentrations occur in the inverse situation, i.e., rural and indoors. Such levels are due to the high proportion of rural/developed countries population relying on unprocessed biomass fuels (like wood, charcoal, agricultural waste, crop residues, dung) which have high pollutant emission factors, in simple small scale combustion devices such as household cooking. Research has also shown that there is derangement of respiratory function in women who are exposed to these fumes [1,2].
Biomass Fuels
It is a renewable energy source and biological material derived from living, or recently living organisms. It can be often made out of plant matter grown to generate electricity or heat. It can be converted into other types of energy too such as methane gas or fuels used for transportation, such as ethanol or biodiesel fuels.
Purpose of using Biomass and its Effects: It is the most precious and versatile resource as solar energy in earth crust which provides not only food but also energy, building materials, fabrics, medicines and chemicals. Biomass is used since the discovery of fire for various tasks such as fuel for cooking, automobile, electricity, etc. In India 2.5 billion people rely on biomass for cooking and remaining house hold works in urban and rural areas [10]. Half of the world’s population relies on biomass because they are cheap and mostly free of cost when compared to other fuels [11,12]. In the absence of new policies, the number of people relying on biomass will increase to over 2.6 billion by 2015 and to 2.7 billion by 2030 due to increased cost of other fuels. Biomass fumes cause air pollution which leads to death of 1.3 million people yearly, mostly women and premature children [10,13]. Studies show that concentrations of ambient air particles are associated with a wide range of effects on human health, especially on cardio respiratory system [14]. Growing evidence indicates that particulate pollution increases daily deaths and hospital admissions throughout the world [15].
Historical Prospective
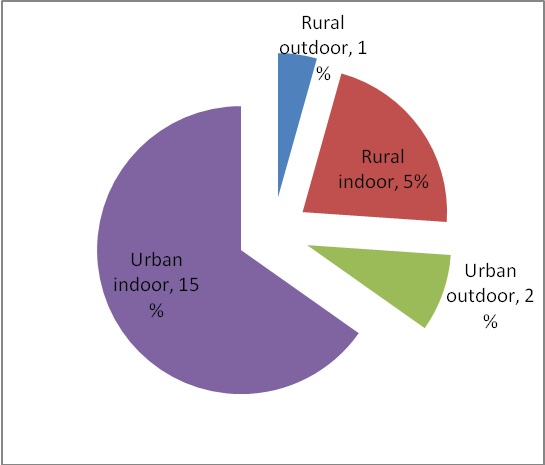
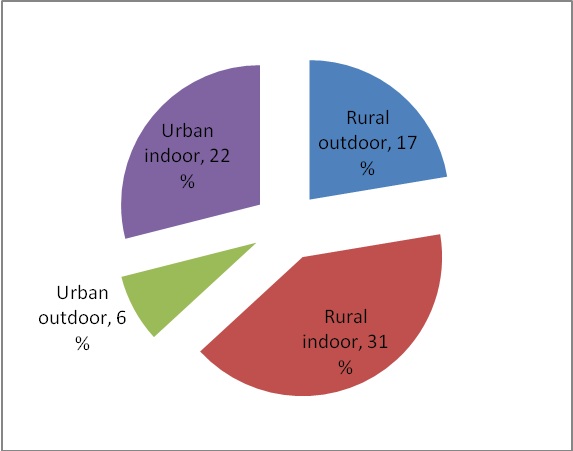
From the 1960s through 1980s, several population based studies were taken up in the industrialized countries and these investigations confirmed the adverse effects of air pollution on human health. These findings opened a floodgate of epidemiological and toxicological investigation on fine and ultrafine particulate biomass pollution and their effect on the respiratory diseases. It was found that long-term, repeated exposures to biomass pollution increase the cumulative risk of chronic pulmonary and cardiovascular disease and even death [16]. WHO estimated that urban air pollution is responsible for approximately 800,000 deaths and 4.6 millions lost life-years. The estimated health impact of urban air pollution is based largely on the results of epidemiological studies conducted in industrialized countries. [Table/Fig-1,2] shows that indoor air pollution by biomass fumes account for 76% in developing countries and it accounts for 23% in developed countries [17].
Air pollution caused by biomass fumes in developed countries.
Source: Krik R. Smith Fuel combustion, air pollution. Exposure and health: situation in developing countries [17].
Air pollution caused by biomass fumes in developing countries.
Source: Krik R. Smith Fuel combustion, air pollution. Exposure and health: situation in developing countries [17].
Biomass Fumes Pollution and Respiratory System: Air borne pollutants enter the body through breathing, causing damage to primary target lung apparatus such as bronchi, bronchioles and alveoli. Studies show that about 480 million alveoli are present in both lobes of an adult human lung; women will be having less alveoli and lung volume than men [18]. The mean size of single alveolus is 4.2×10 μm3. Alveoli make up approximately 64% of the lung space. Human lungs have a total surface area of 1,400 m2, and every day we inhale approximately 15m3 of air. Weight of this inhaled air is greater than the food and water we consume in a day. The lung volume and breathing frequencies of healthy adults at rest is 400-500ml and 15-17 breaths per minute respectively [19].
The pollutants present in biomass fumes include CO, SO2, NO, suspended particulate matter, benzene and benzopyrene [14].
Pollutants
The pollutants present in biomass fumes include:
Carbon Monoxide (CO): It is a toxic gas emitted into the atmosphere as a result of burning process formed by the oxidation of hydrocarbons and other organic compounds. The CO gas at 1000rpm (release per minute) can cause unconsciousness in about one hour and death in four hours. However, concentration of CO as little as 200 rpm may produce symptoms of poisoning. If inhaled for few hours it may be toxic, given at concentration of 30 rpm as it causes dizziness, headache [20]. CO interferes with O2 transport through the formation of carboxyhemoglobin. Intense short term exposure to CO can lead to loss of consciousness was known by physicians in the late 19th century. It can be used as an anaesthetic [21].
Sulphur Dioxide (SO2): It is an acidic gas emitted indirectly proportional to the amount of sulphur in fuel. It combines with water vapour in the atmosphere to produce acid rain. It can affect human health more likely in those suffering from asthma and chronic lung diseases. Evidence suggests that exposure to SO2 given at low levels makes the airways in the lung more sensitive to bronchoconstrictors, substances that cause airways to constrict. This in turn inhibits O2 exchange and results in wheezing, gasping, shortness of breath. The relative risk of respiratory mortalities increase in the concentration of pollutant ranged from 1.015mg/m3 to 10mg/m3 [22].
Nitrogen Monoxide (NO): NO is formed during combustion process at high temperatures from the oxidation of nitrogen in air. The major types of oxides of nitrogen present in air are NO and NO2. The main source of NO is road traffic and biomass emissions. Major amount of NO is emitted by biomass [23]. NO2 is a precursor of O3 formed in the troposphere. Oxides of nitrogen are immunotoxic and increase the susceptibility of respiratory tract to infections such as influenza. Frequent exposure to high concentration of NO causes airway irritation and consequent acute respiratory illness [23].
Suspended Particulate Matter: Particulate Matter (PM) is combination of solid particles and liquid droplets also known as aerosols found in the air. Coarse particles/>2.5μm in diameter come from windblown dust and grinding operation is also known as PM10. Fine particles/<2.5μm in diameter of PM 2.5 are emitted from burning of timber, which causes health problems comprising of premature death, respiratory related hospital admission and emergency room visit. The exacerbation of asthma, acute respiratory symptoms such as severe chest pain, gasping, coughing, chronic bronchitis and decreased lung function. Persistent exposure to biomass smoke is associated with impaired lung function, COPD, sore throat, cough, recurring head ache, eye irritation, dizziness, muscle pain, asthma, life threatening health problems and associated with greater risk of hypertension, cancer in lungs. Women who were using biomass fuel had several cellular changes in their lungs. Sputum samples of these women contained an excess of alveolar macrophages, neutrophils, eosinophil’s, lymphocytes [17,22].
Effect of Chronic Exposure to Pollutants Present in Biomass Fumes: The symptoms are broadly classified into 2 groups: Upper Respiratory Symptoms includes-Runny nose, Sinusitis, Sore throat, Wet cough, dry cough, cold, head ache, red eyes and fever. Lower Respiratory Symptoms includes-wheezing, phlegm, chest discomfort and shortness of breath. The structural and functional damage of respiratory system, very often the symptom of multifactor respiratory diseases like asthma and COPD are aggravated following exposure to biomass fumes pollutants [24].
Adverse Health Effects of Biomass Fumes Pollution:
Overall Mortality: There is a little doubt that exposure to biomass emissions result in increased risks of mortality, particularly from cardiopulmonary causes. A meta analysis found that PM10, CO, NO2, O3 and SO2 were significantly associated with mortality. A study in Los Angeles for the period 1982-2000 found a strong increase in mortality with prolonged exposure to PM2.5. Among all of them NO2 was the strongest predictor for mortality. This effect was again evident during a later on analysis of 12 Canadian cities between 1981-1999 were positive and statistically significant association was observed between variations in NO2 concentration and fluctuation in daily mortality rates [25].
Respiratory Effects: One of the most commonly studied and reported health effect linked to pollution was respiratory morbidity. Sood A have found that exposure of biomass leads to adverse effects on respiratory system ranging from coughing and wheezing which are acute symptoms, chronic conditions such as asthma, CB and emphysema [26]. Studies have shown varying results on the relationship between NO2 exposures on respiratory health. NO2 is most clearly associated with cough [15].
The decrease in lung function in biomass fuel users may be due to the chronic inhalation of particulate matter and toxic gases emitted during biomass combustion leading to inflammatory changes. It can be explained as if when cooking index is increased, the pulmonary functions are also much affected. Cooking index indicates number of hours of cooking per day is multiplied with number of years of cooking [27].
Cooking index = No. of hours of cooking/day × No. of years of exposure [27].
Previous Studies Associated with Biomass Fuels and Lung Function Tests:
Revathi M et al., found that the lung function parameters were significantly lesser in the study group, exposed to biomass fuel and concluded that the reduction in the pulmonary function in the biomass exposed women could be due to high exposure of biomass pollutants with inadequate ventilation [28]. Agarwal A et al., found that there is impairment of the lung function in women exposed to biomass fumes compared to those not exposed to such fumes [29]. Reddy TS et al., indicated that passive smoking showed no significant difference between the two groups using biomass and LPG and may be due to better ventilation in kitchens [30]. Levi M et al., studied pulmonary function tests in COPD patients and results were compared with the controls and found that wood or charcoal alone independently increased the risk of COPD and concluded that a strong association between wood or charcoal smoke exposure for COPD [31].
Behera D et al., studied ventilatory function in non-smoking rural Indian women using different cooking fuels. Lung function parameters were measured in 3,318 non smoking Indian women using four different types of cooking fuels (biomass, LPG, kerosene and mixed). Biomass fuel users had FVC values less than 75% predicted whereas in other groups it was more than 75% of predicted. However, FEV1, FEV1/FVC (%) and PEFR were within normal limits in all the four groups. The absolute values of all the three parameters of lung functions were the lowest in the biomass and mixed fuel users. A negative correlation was observed between these parameters and the duration of cooking and exposure index and showed that, lung function, particularly FVC, is affected by indoor air pollution due to domestic biomass cooking fuel [32].
Pravallika P et al., showed biomass fuel for cooking had sub clinical respiratory impairment mainly in early stage small air way obstruction. The adverse effects of biomass fuel on lung function could be due to exposure to high concentration of pollutants like CO, SO2, NO2, PM, polyhydroxy aromatic hydrocarbons liberated by biomass fuel combustion and inadequate ventilation. It is also found that degree of dysfunction or lung impairment correlates with duration of exposure [24].
Kiraz K et al., compared frequency of COPD and CB in rural women exposed to biomass fuels and urban women who are not exposed to such fuels and stated that all the pulmonary functions tests were normal except FEV which lowered in rural women leading to COPD [33].
Po JYT et al., concluded that exposure of biomass leads to adverse effects on respiratory system among rural population. Awareness and remedial measures like improvement of stove design lowers exposure to emission which might reduce adverse effects [34].
Rinne ST et al., showed that there was a significant increase in mortality of infants (p=0.008), increase in history of cough (p=0.02) and ear ache (p<0.001) in children among families using higher proportion of biomass fuel for cooking [35].
Lahari T et al., studied health impact of biomass fuel use in rural India and showed respiratory symptoms like cough, sore throat, wheeze and chest pain were more prevalent in women using biomass fuels, and lung functions were impaired in biomass users. Sputum cytology of a large majority of biomass users revealed inflammatory and hypersensitivity reactions, and their blood samples showed anaemia, low antioxidant levels, depletion of CD4+ T helper cells and significant increase in CD8+cytotoxic T cells and CD56+ natural killer cells, indicating altered immunity. Biomass users had thrombocytosis, platelet P-selectin overexpression and increased micronucleus frequency in exposed cells, suggesting greater risk for cardiovascular problems and genotoxicity [36].
Liu S et al., studied the association between COPD and the use of biomass fuels for cooking and heating in developing countries and showed that the prevalence of COPD is significantly higher in rural population. They concluded that indoor pollutants from biomass fuels was an important risk factor for COPD [37].
Conclusion
Healthy non smoking women using biomass fuel for cooking are affected by sub clinical respiratory impairment mainly early stage small air-way obstruction. The adverse effects of biomass fuel on lung function could be due to exposure to high concentration of pollutants like carbon monoxide, sulphur dioxide, nitrogen dioxide, particulate matter, polyhydroxy aromatic hydrocarbons liberated by biomass fuel combustion and inadequate ventilation. It is also found that degree of dysfunction or lung impairment correlates with duration of exposure.
[1]. Frank JK, Julia C, Air pollution and public health: emerging hazards and improved understanding of riskEnviron Geochem Health 2015 37(4):631-49.10.1007/s10653-015-9720-126040976 [Google Scholar] [CrossRef] [PubMed]
[2]. Vargas MPS, Teran LM, Air pollution: Impact and preventionRespirology 2012 17(7):1031-38.10.1111/j.1440-1843.2012.02213.x22726103 [Google Scholar] [CrossRef] [PubMed]
[3]. Anderson JO, Thundiyil JG, Stolbach A, Clearing the air: a review of the effects of particulate matter air pollution on human healthJ Med Toxicol 2012 8(2):166-75.10.1007/s13181-011-0203-122194192 [Google Scholar] [CrossRef] [PubMed]
[4]. Ostro B, Tobias A, Querol X, Alastuey A, Amato F, Pey J, The effects of particulate matter sources on daily mortality: A case-crossover study of Barcelona, SpainEnviron Health Perspect 2011 119(12):1781-87.10.1289/ehp.110361821846610 [Google Scholar] [CrossRef] [PubMed]
[5]. Brook M, Rajagopalan S, Particulate matter, air pollution, and blood pressureJournal of the American Society of Hypertension 2009 3(5):332-50.10.1016/j.jash.2009.08.00520409976 [Google Scholar] [CrossRef] [PubMed]
[6]. Nemery B, Hoek P, Nemmar A, The Meuse Valley fog of 1930: An air pollution disasterLancet 2001 357:704-08.10.1016/S0140-6736(00)04135-0 [Google Scholar] [CrossRef]
[7]. Suresh R, Singh VK, Malik JK, Datta A, Pal RC, Evaluation of the performance of improved biomass cooking stoves with different solid biomass fuel typesBiomass and Bioenergy 2016 95:27-34.10.1016/j.biombioe.2016.08.002 [Google Scholar] [CrossRef]
[8]. Mannucci PM, Franchini M, Health effects of ambient air pollution in developing countriesInt J Environ Res Public Health 2017 14:104810.3390/ijerph1409104828895888 [Google Scholar] [CrossRef] [PubMed]
[9]. Martin WJ II, Glass RI, Araj H, Balbus J, Collins FS, Household air pollution in low- and middle-income countries: health risks and research prioritiesPLoS Med 2013 10(6):e100145510.1371/journal.pmed.100145523750119 [Google Scholar] [CrossRef] [PubMed]
[10]. Abeeku Brew-Hammond, Energy for Cooking In Developing CountriesWorld Energy Outlook 2006 FranceInternational Energy Agency (IEA), Head of Publications Service:419-45.10.1787/weo-2006-16-en [Google Scholar] [CrossRef]
[11]. Barnes DF, Openshaw K, Smith KR, Plas R, What makes people cook with improved biomass stoves?World Bank Technical Paper No. 242 1994 [Google Scholar]
[12]. Nandasena S, Wickremasinghe AR, Sathiakumar N, Biomass fuel use for cooking in Sri Lanka: Analysis of Data from National Demographic Health SurveysAm J Ind Med 2012 55(12):1122-28.10.1002/ajim.2102322068890 [Google Scholar] [CrossRef] [PubMed]
[13]. Apte k, Salvi S, Household air pollution and its effects on health. Version 1F1000Res 2016 5:F1000Faculty Rev-259310.12688/f1000research.7552.127853506 [Google Scholar] [CrossRef] [PubMed]
[14]. Azam AG, Zanjani BR, Mood MB, Effects of air pollution on human health and practical measures for prevention in IranJ Res Med Sci 2016 21:6510.4103/1735-1995.18964627904610 [Google Scholar] [CrossRef] [PubMed]
[15]. Zannobetti A, Schwartz J, Arc diabetics more susceptible to the health effects of air borne particles?Am J Respir Crit Care Med 2001 164:831-33.10.1164/ajrccm.164.5.201203911549541 [Google Scholar] [CrossRef] [PubMed]
[16]. Pope CA III, Burnett RT, Thurston GD, Thun MJ, Calle EE, Krewski D, Cardiovascular mortrality and long term exposure to particulate air pollution: epidemiological evidence of general pathophysiological pathways diseaseCirculation 2004 109:71-77.10.1161/01.CIR.0000108927.80044.7F14676145 [Google Scholar] [CrossRef] [PubMed]
[17]. Smith KR, Fuel combustion, air pollution. Exposure and health: situation in developing countriesAnnu Rev Energy Environ 1993 18:529-66.10.1146/annurev.eg.18.110193.002525 [Google Scholar] [CrossRef]
[18]. Tobin MJ, Chada TS, Jenouri J, Birch SJ, Gazeroglu HB, Sackner MA, Breathing patterns; normal subjectsChest 1983 84:202-05.10.1016/S0012-3692(15)33498-X [Google Scholar] [CrossRef]
[19]. Ochs M, Nyengaard JR, Jung A, Knudsen L, Voigt M, Wahlers T, The number of alveoli in the human lungAm J Respir Crit Care Med 2004 169(1):120-24.10.1164/rccm.200308-1107OC14512270 [Google Scholar] [CrossRef] [PubMed]
[20]. Martín NA, Ozone Therapy for patient poisoned by carbon monoxideRevista Española de Ozonoterapia 2016 6(1):165-86. [Google Scholar]
[21]. Wei W, Zhang W, Hu D, Ou L, Tong Y, Shen G, Emissions of carbon monoxide and carbon dioxide from uncompressed and pelletized biomass fuel burning in typical household stoves in ChinaAtmospheric Environment 2012 56:136-42.10.1016/j.atmosenv.2012.03.060 [Google Scholar] [CrossRef]
[22]. Goldsmith RL, Oakey J, Simms NJ, Gaseous emissions during concurrent combustion of biomass and non-recyclable municipal solid wasteChem Cent J 2011 5:410.1186/1752-153X-5-421284885 [Google Scholar] [CrossRef] [PubMed]
[23]. Mladenovic MR, Dakic D, Nemoda SD, Paprika MJ, Komatina MS, Repic BS, The combustion of biomass – The impact of its types and combustion technologies on the emission of nitrogen oxideHem Ind 2016 70(3):287-98.10.2298/HEMIND150409033M [Google Scholar] [CrossRef]
[24]. Pravallika P, Sharvani N, Ahamed RN, Study of pulmonary function tests in women exposed to biomass fumesIndian Journal of Applied Research 2015 5(4):781-84. [Google Scholar]
[25]. Verwijst T, Shoot mortality and dynamics of live and dead biomass in a stand of Salix viminalisBiomass and Bioenergy 1991 1(1):35-39.10.1016/0961-9534(91)90049-I [Google Scholar] [CrossRef]
[26]. Sood A, Indoor fuel exposure and the lung in both developing and developed countries: An updateClin Chest Med 2012 33(4):649-65.10.1016/j.ccm.2012.08.00323153607 [Google Scholar] [CrossRef] [PubMed]
[27]. Behera D, Chakrabarti T, Khandujal KL, Effect of exposure to domestic cooking fuels on bronchial asthmaIndian J Chest Dis Allied Sci 2001 43:27-311. [Google Scholar]
[28]. Revathi M, Kutty K, Annamalai N, Pulmonary function tests in rural women exposed to biomass fuelsJ Pulmon Resp Med 2012 2:7 [Google Scholar]
[29]. Agarwal A, Patil SN, Pulmonary function tests in rural women exposed to biomass fumesIndian Journal of Basic & Applied Medical Research 2013 2(7):673-78. [Google Scholar]
[30]. Reddy TS, Guleria R, Sinha S, Sharma SK, Pande JN, Domestic cooking fuel and lung functions in healthy non-smoking womenIndian J Chest Dis Allied Sci 2004 46:85-90. [Google Scholar]
[31]. Levi MO, Aymerich JG, Villar J, Sarmiento AR, Antó JM, Gea J, Wood smoke exposure and risk of chronic obstructive pulmonary diseaseEur Respir J 2006 27(3):542-46.10.1183/09031936.06.0005270516507854 [Google Scholar] [CrossRef] [PubMed]
[32]. Behera D, Jindal SK, Malhotra HS, Ventilatory function in nonsmoking rural Indian women using different cooking fuelsRespiration 1994 61(2):89-92.10.1159/0001963138008994 [Google Scholar] [CrossRef] [PubMed]
[33]. Kiraz K, Kart L, Demir R, Oymak S, Gulmez I, Chronic pulmonary disease in rural women exposed to biomass fumesClin Invest Med 2003 26:243-48. [Google Scholar]
[34]. Po JYT, FitzGerald JM, Carlsten C, Respiratory disease associated with solid biomass fuel exposure in rural women and children: systematic review and meta-analysisThorax 2011 66:232-39.10.1136/thx.2010.14788421248322 [Google Scholar] [CrossRef] [PubMed]
[35]. Rinne ST, Rodas EJ, Rinne ML, Simpson JM, Glickman LT, Use of biomass fuel is associated with infant mortality and child health in trend analysisAm J Trop Med Hyg 2007 76(3):585-91.10.4269/ajtmh.2007.76.58517360888 [Google Scholar] [CrossRef] [PubMed]
[36]. Lahari T, Ray MR, Health impacts of biomass fuel use in rural IndiaIJMR 2001 62:625-28. [Google Scholar]
[37]. Liu S, Zhou Y, Wang X, Wang D, Lu J, Zheng J, Biomass fuels are the probable risk factor for chronic obstructive pulmonary disease in rural south chinaThorax 2007 62:889-97.10.1136/thx.2006.06145717483137 [Google Scholar] [CrossRef] [PubMed]