Shoulder pain is the second most common problem of the musculoskeletal system affecting approximately 16-21% of the population [1-3]. The most frequent cause of shoulder pain is SIS accounting for 44-60% of all complaints of shoulder pain [1,3-5]. This syndrome occurs when the tendons of the rotator cuff impinge under the coracoacromial arch. Most commonly supraspinatus or infraspinatus tendons are impinged. The syndrome can be caused due to some factors like imbalance of the rotator cuff muscles, weakness of scapular muscles, pathology in tendon or varied shape of the acromion process [4] Impingement syndrome often restricts the shoulder motion and interferes with the patient’s ability to perform daily activities [6,7].
Physiotherapists use a wide range of interventions which include thermotherapy, electrotherapy, therapeutic exercise therapy and manual physical therapy. Though various electrotherapy modalities are commonly used in shoulder pain and impingement but they have no proven benefits in SIS [8,9].
Therapeutic exercises generally have a positive effect in restoring shoulder mobility and retraining of muscle imbalance in SIS [10-12]. Previous studies have found that Maitland passive joint mobilisation along with exercises is effective in treating SIS [10,11]. A case series done on SIS incorporated impairment based exercises, thrust and non-thrust technique in patients with SIS and found improvement in functional outcome measure [3].
Cryotherapy is a type of thermotherapy and for decades has a moderate evidence in reducing the pain and inflammation of SIS [9,12]. The previous study has found the effectiveness of cryotherapy when incorporated with strengthening and stretching exercises in SIS and the researchers have suggested that cryotherapy along with exercises should be compared with manual therapy techniques [13].
Manual therapy has become increasingly important for the treatment of pain and dysfunction in the treatment of musculoskeletal disorders of the shoulder [14]. A study has found the effectiveness of manual therapy along with exercises in SIS [15]. MWM is a widely used manual therapy technique given by Brian Mulligan, which is beneficial in reducing pain and improving functional independence. MWM is also found effective in SIS [16-20].
Though, MWM and cryotherapy, both are individually found effective in SIS, there is no literature which compares the effectiveness of both the treatment strategies. If any one treatment is proved to be effective than other it will be useful for the therapist as it saves time, for the patient as it will be cost-effective and in the research point of view more high-quality studies can be done. It is an interesting study which compares thermotherapy with manual therapy, with both having analgesic effects but in a contrasting mode of application. Thus, there is a necessity to perform a study which compares both the treatment strategies.
Materials and Methods
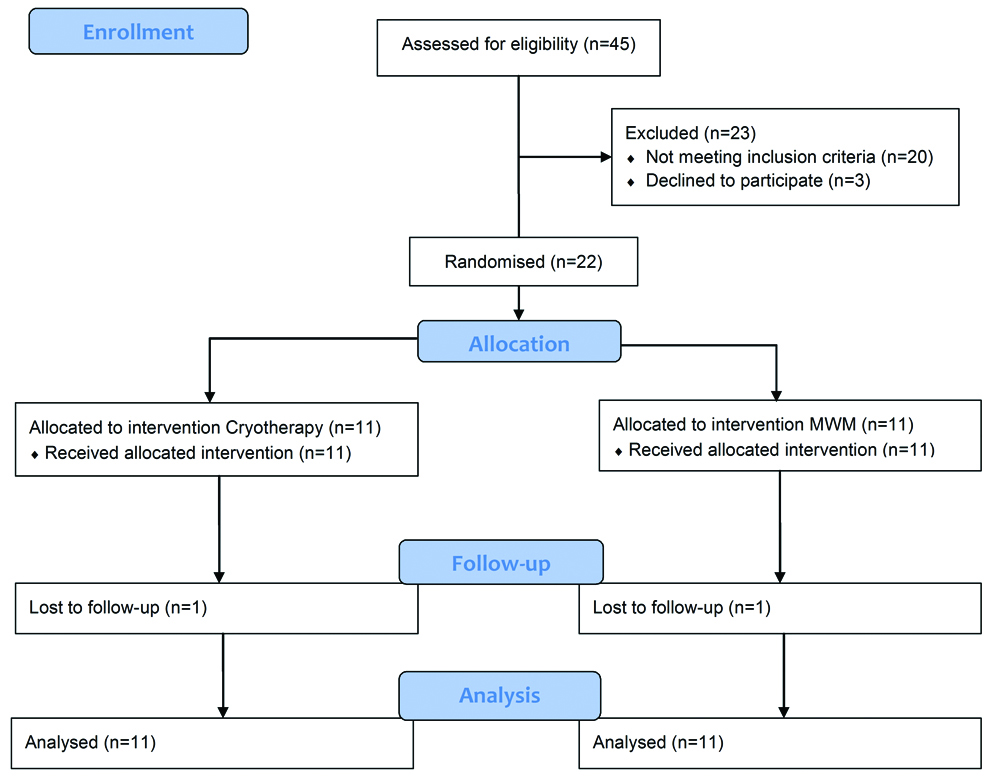
The study was a single-blinded randomised clinical trial (CTRI/2017/09/009847) conducted from March 2011 to February 2012 at the Department of Physiotherapy, KMC, Mangalore, Karnataka, India. The study was approved by the time-bound Ethical Research Committee of Manipal Academy of Higher Education. 22 subjects, 12 men, and 10 women, aged 18-64 (mean 46 years) and diagnosed with shoulder impingement by the physician participated in this study. The subjects were enrolled if the symptoms were present since last three weeks, presence of painful abduction or painful arc (sensitivity: 74%, specificity: 81%) and three positive tests out of five battery of tests. It has been speculated that a single test of positive painful arc is helpful in diagnosing SIS [9,21]. However, a combination of shoulder tests is desirable to provide better diagnostic accuracy in SIS [4,21,22]. Subjects were included if at least three of the five tests were positive: Neer’s Impingement test (sensitivity: 78%; specificity: 58%), Hawkin’s Kennedy (sensitivity: 58%; specificity: 67%), Jobe’s/Empty Can test (sensitivity: 81%; specificity: 89%), Speed test (sensitivity: 68.5%, specificity: 55.5%) and Gerber test/Lift off sign (sensitivity: 42%, specificity: 97%) [13]. Gerber test is said to have the highest diagnostic utility [23] and it has been recognised that if a painful arc test is positive then SIS is very likely to be present, conversely, if Neers test is negative, impingement is very unlikely [9]. A written informed consent was obtained from all the subjects. Subjects were excluded if they had neck pain, shoulder fracture or dislocation, surgery of shoulder in the past one year, tumour or neuromuscular disorders around the shoulder, open wound over shoulder region, any other shoulder pathology, cold hypersensitivity or cold intolerance and circulatory compromise. The sample size of the study is 22 which were calculated by using the formula: 2(zα+zβ)2 σ2/δ2. At 95% confidence level (zα) is 1.96, at 80% power (zβ) was 0.84, the standard deviation (σ) was 9.1 and effect size (δ) was 10.8. The minimum sample size obtained to carry out the study was 11 in each group. The principal investigator enrolled and randomly assigned the subjects to one of the two intervention groups using the block randomisation method. Group ‘A’ received Cryotherapy and exercises and Group ‘B’ received MWM and exercises. Subjects were informed about their treatment protocol. All outcome measures were taken by an assessor who was blinded to the treatment groups, had a clinical experience of three years and was not a part of the study. Blinding or masking of assessor ensured unbiased ascertainment of outcomes. The Consolidated Standards of Reporting Trials (CONSORT) flow chart describing the blueprint of the study is shown [Table/Fig-1].
Measurements
A 10 point VAS was used to assess pain intensity. The tool consists of a 10 cm line which ranges from no pain to the worst pain ever experienced. The subjects marked to indicate the severity of their pain. It has good reliability and validity [24].
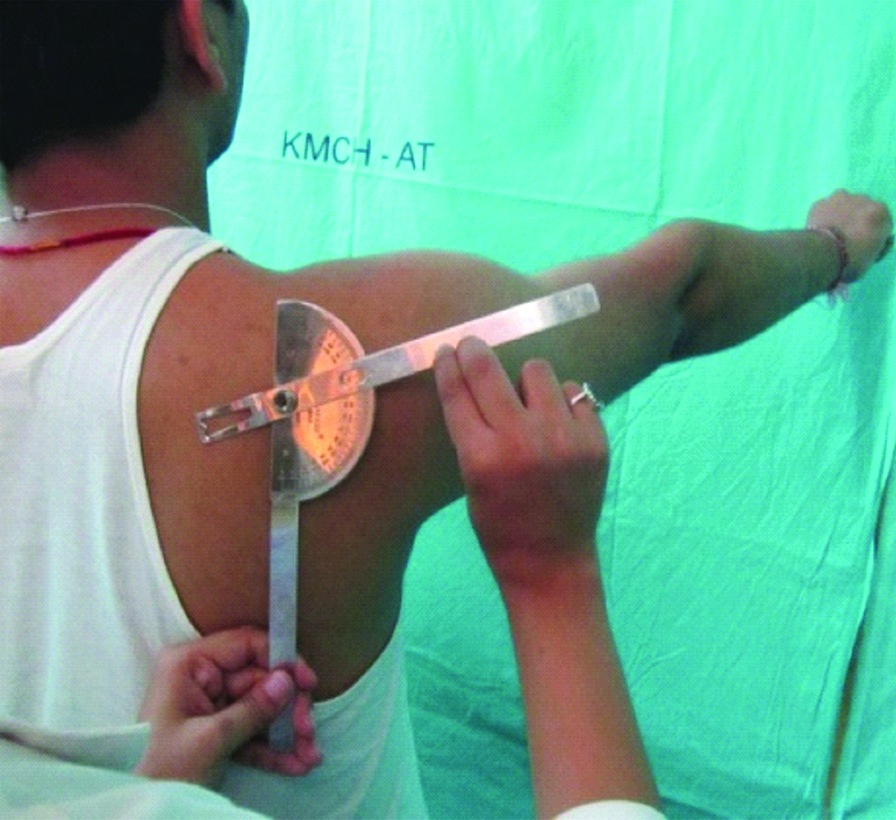
A universal goniometer was utilised to gauge the ROM in the plane of the scapula. This has demonstrated good intra-rater reliability. The plane of the scapula is defined as 30° anterior to the frontal plane. It is calculated by placing fulcrum over the superior aspect of the shoulder, the stationary arm was kept parallel to the coronal plane and the moving arm was maintained at 30° forward from that coronal plane [18]. The patient was instructed to abduct the affected limb in that plane [Table/Fig-2]. The range of motion was recorded by placing the axis of goniometer over the centre of the glenohumeral joint, stationary arm parallel to the lateral border of the scapula and moving arm along the humerus [Table/Fig-3]. The numerically SPADI is a self-administered questionnaire developed to measure the pain and disability associated with shoulder pathology. The SPADI consists of 13 items in two subscales: pain (5 items) and disability (8 items). The scale ranges from 0 which denotes no pain and 10 indicates worst pain ever. The total pain and disability score was divided by 130 and then presented in percentage.
Calculating plane of scapula.
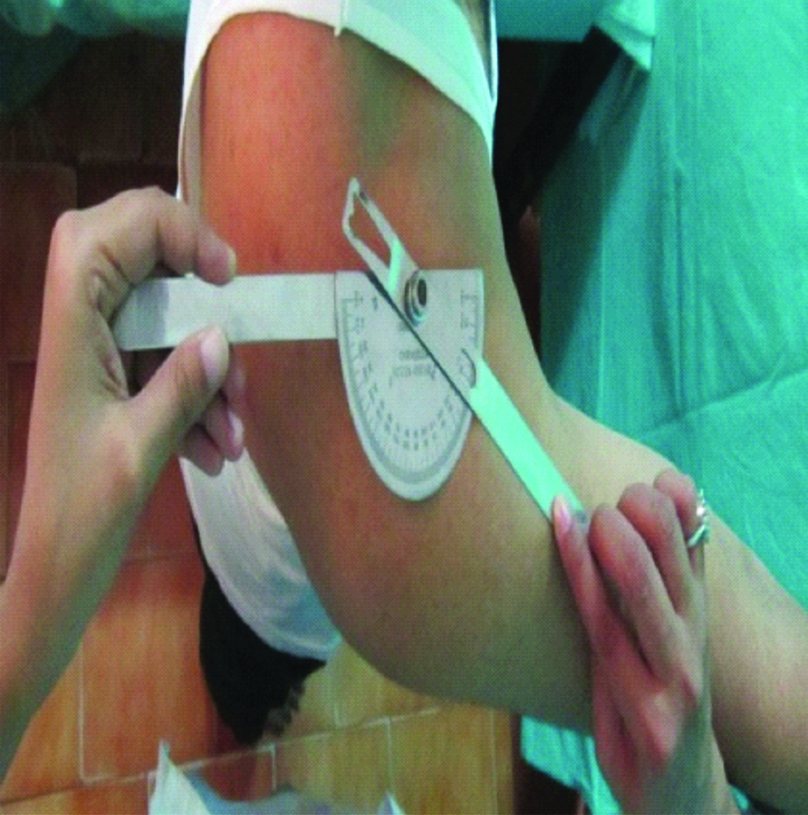
Range of motion in the plane of scapula.
Intervention
Group A: Treatment included two cold packs containing silica and covered with vinyl. The temperature of the cold pack was maintained at -5°C. The patient was positioned in supine lying. Clothing was removed from the shoulder region and the cold packs were wrapped in a damp towel. One cold pack was placed on the anterior aspect of shoulder and the other one was placed on the posterior aspect of the shoulder. In the session, cold packs were applied on the affected shoulder for 20 minutes [13,25].
Group B: The therapist stood behind the patient on the opposite side to the affected shoulder. One hand was placed over the scapula and another hand was placed over the anterior aspect of the head of the humerus. A sustained posterolateral glide was then applied to the head of the humerus, while the patient was asked to simultaneously elevate the affected arm into abduction till the point of perceived pain [Table/Fig-4] [18]. Three sets of ten repetitions were given with rest period of 30 seconds between each set. The treatment in both the groups was given daily once, for six days.
Therapist maintaining posterolateral glide over the glenohumeral joint.

Impairment based exercises: The impairment-based exercises were also given to the patients of both the groups. Manual muscle testing was performed for lower and middle trapezius, serratus anterior, infraspinatus, and deltoid. The tightness was checked for upper trapezius, pectorals, and levator scapula. These muscles were selected as these muscles are normally found weaker and tighter in patients with SIS [26]. The weak muscles were given, isometric strengthening exercises consisting of three sets of 15 repetitions each with a hold period of 5-10 seconds and stretching exercises for tight muscles were given for three repetitions of 30 seconds hold with 30 seconds of rest between the repetitions [27]. The treatment was done for a total of six sessions in both the groups. All the outcome measures were documented before starting the intervention, immediately after the intervention (except SPADI) and also after the six sessions of treatment.
Statistical Analysis
All statistical analysis was done using SPSS version 16.0. The level of significance of <0.05 was considered to be statistically significant at 95% confidence interval. An intention to treat analysis was performed where the last-observation-carried-forward method was used. Missing observations for participants who withdrew were replaced with their last observed value. Analysis between the groups was done by Mann-Whitney U test and within the group by comparing pre and post values using Wilcoxon signed rank test.
Results
The study included 22 subjects, out of which there were 46% were females and 54% were males. At the beginning of the study, there was no significant difference (p>0.05) between the two groups based on age or the outcome measures VAS, SPADI (Mann-Whitney U test) and ROM (Independent t-test) [Table/Fig-5]. One subject per group was not followed up. All 22 subjects were analysed using intention to treat analysis. In between the groups analysis there was no significant difference after the six treatment sessions, using Mann-Whitney U test for VAS and SPADI, and Independent t-test for ROM (p>0.05) [Table/Fig-6]. However, a statistically significant difference exists within both the groups by comparing pre and post, at the end of six treatment sessions using Wilcoxon Signed Rank test [Table/Fig-7]. This means there was an equal improvement seen in both the groups. There also exists a significant difference immediately after the application of MWM (p<0.05) in terms of VAS and ROM [Table/Fig-8]. The trial was stopped post completion of recruitment of subjects. A long-term follow-up was not performed.
Baseline details of the subjects in the study.
| Baseline Variables | Age (Years) | Vas (cm) (Pre) | Rom (Degree) (Pre) | SPADI (%) (Pre) | p-value |
|---|
| Mean (SD) | Mean (SD) | Median (IQR) | Mean (SD) | Mean (SD) | Median (IQR) | |
|---|
| Group A | 41.91 (11.22) | 5.636 (1.206) | 5 (5-7) | 107.27 (13.29) | 48.09 (22.49) | 43.07 (29.23-79.20) | >0.05 |
| Group B | 50.09 (11.36) | 5.90 (1.136) | 6 (5-7) | 100.91 (9.95) | 48.59 (14.10) | 20.76 (17.69-27.69) |
Comparison of outcome measures between the groups at the end of sixth day treatment session.
| Outcome Measure | VAS (cm) (Post) | ROM (degree) (Post) | SPADI (%) (Post) | p-value |
|---|
| Mean (SD) | Median (IQR) | Mean (SD) | Mean (SD) | Median (IQR) | |
|---|
| Group A | 2.54 (1.128) | 3 (2-3) | 129.09 (16.55) | 20.32 (8.72) | 20.76 (17.69-27.69) | >0.05 |
| Group B | 3.54 (2.33) | 3 (2-6) | 124.54 (16.9) | 30.82 (21.85) | 23.07 (7.69-59.23) |
Tests used for between the group analysis:
For VAS: Mann-Whitney U Test; For ROM: Independent T-Test; For SPADI: Mann-Whitney U Test
IQR: Inter quartile range
Comparison of outcome measures within the groups at the end of sixth day treatment session.
| Outcome Measures | VAS Mean Diff. | p-value | ROM Mean Diff. | p-value | SPADI Mean Diff. | p-value |
|---|
| Group A | 3.096 | <0.05 | 21.82 | <0.05 | 27.77 | <0.05 |
| Group B | 2.36 | <0.05 | 23.63 | <0.05 | 17.77 | <0.05 |
Within The Group Analysis:
For VAS: Wilcoxon Signed Rank; For ROM: Paired T-Test; For SPADI: Wilcoxon Signed Rank
Comparison of outcome measures within the group at the end of first day treatment session.
| Outcome Measures | VAS | ROM | p-value |
|---|
| Mean (SD) | Mean Diff. | Median (IQR) | Mean (SD) | Mean Diff. |
|---|
| Group A | 5.18 (1.60) | 0.456 | 5 (4-6) | 110.4 | 3.13 | >0.05 |
| Group B | 5 (1.18) | 0.9 | 5 (4-6) | 107.7 | 6.79 | <0.05 |
Within The Group Analysis:
For VAS: Wilcoxon Signed Rank; For ROM: Paired T-Test
IQR: Inter Quartile Range
Discussion
Shoulder impingement syndrome is a common reason for shoulder pain and functional disability [10]. This is the first study which was conducted to compare the effectiveness of cryotherapy and MWM along with stretching and strengthening exercises in SIS patients. We aimed to find out and compare the immediate and effects at the end of six treatment session between both the groups. In the present study, we concluded that at the end of six treatment sessions both the groups were equally benefitted with respect to pain, ROM, and functions; however, we found noteworthy immediate improvement in pain and ROM in MWM group only, which could be because of the prompt correction of the positional fault present in shoulder impingement subjects. Studies on shoulder impingement have demonstrated abnormal or excessive superior/ anterior translation of the humeral head in the glenoid fossa leading to pain, and functional impairment. Application of a posterior-lateral glide (MWM) to the shoulder may immediately correct this fault and allow optimal pain-free motion to occur [18-20]. Kachingwe AF et al., also found immediate improvement in VAS and ROM following MWM in shoulder impingement patients [15]. Teys P et al., on patients with shoulder pain found immediate improvement in ROM post MWM, when compared with sham and control group [18]. Delgado-Gil JA et al, also found immediate improvement in pain and range of motion post MWM in SIS patients [20]. A recent study done on SIS, treated with MWM also demonstrated similar outcomes, in accordance with the results of the current study [17].
We did not find any immediate recovery in the cryotherapy group, which contradicts the findings of the study done by Krukowska J et al., where they utilised cryotherapy for painful shoulder syndrome. They have found immediate alleviation in pain and enhancement of ROM [12]. However, their study consisted of a heterogeneous group of patients, whereas in the current study we had a homogenous group of patients.
In the present study, we also reported, equal improvement in the outcome measures post six treatment sessions in both the groups. Both cryotherapy and MWM allays pain by activating the analgesic descending pathway of the central nervous system such as endorphins [28,29]. Cryotherapy additionally has inhibitory physiological impacts which help in diminishing pain [12]. Apart from acting through pain gate mechanism, MWM also alleviates pain and improves ROM by reversing the positional fault or the mal-tracking precipitated by an injury or strain [19].
CSP guidelines and a previously done study on SIS emphasised the efficacy of cryotherapy in pain [9,13]. The investigators found cryotherapy along with strengthening and stretching exercises was effective in reducing pain and improving functional activities shoulder impingement. However, the study lacked a comparison group [13]. In the current study, we compared cryotherapy with MWM.
In addition to the individual mechanisms of techniques, improvement in both the groups could be also because of the incorporation of impairment based exercises to all the patients regardless of their groups [3].
Shoulder impingement syndrome is pertinent to poor flexibility and weakness of pectorals, rotator cuff and periscapular muscles leading to upward translation of the humeral head during abduction and reducing the subacromial space [26]. A muscle imbalance within deltoid and rotator cuff also causes impingement. With the weakness of infraspinatus, the compressive force on the glenohumeral head is reduced leading to instability and impingement [3,26]. In the current study, out of 22 patients, 18 had weakness of serratus anterior, lower trapezius, middle trapezius, and tightness of upper trapezius and pectorals, rest 4 patients had weakness of rotator cuff muscles. According to their impairment exercises were given.
Our protocol thus included both strengthening and stretching of muscle according to the impairments present in each patient which could have addressed the problem causing reduced subacromial space and thereby relieving symptoms [3]. A previous study incorporated daily eccentric strengthening exercises of the rotator cuff in SIS patients and found diminution in pain intensity and betterment in functional activities [13].
Limitation
We understand that a small sample size is one of the main limitations of the study. Future studies can incorporate a third group comprising of only exercises and a longer duration follow study can be done.
Conclusion
There was no difference between the two groups at the end of six sessions. At the end of six treatment sessions both the therapies showed similar results. However, for an immediate improvement with regard to pain and range of motion MWM can be given to patients with SIS.
Tests used for between the group analysis:
For VAS: Mann-Whitney U Test; For ROM: Independent T-Test; For SPADI: Mann-Whitney U Test
IQR: Inter quartile range
Within The Group Analysis:
For VAS: Wilcoxon Signed Rank; For ROM: Paired T-Test; For SPADI: Wilcoxon Signed Rank
Within The Group Analysis:
For VAS: Wilcoxon Signed Rank; For ROM: Paired T-Test
IQR: Inter Quartile Range