A Novel “Over the Wire” Technique for a Case of Difficult Percutaneous Transvenousmitral Commissurotomy
Akshyaya Pradhan1, Pravessh Vishwakarma2, Monika Bhandari3, Rishi Sethi4, Varun Shankar Narain5
1 Assistant Professor, Department of Cardiology, King George’s Medical University, Lucknow, Uttar Pradesh, India.
2 Assistant Professor, Department of Cardiology, King George’s Medical University, Lucknow, Uttar Pradesh, India.
3 Assistant Professor, Department of Cardiology, King George’s Medical University, Lucknow, Uttar Pradesh, India.
4 Professor, Department of Cardiology, King George’s Medical University, Lucknow, Uttar Pradesh, India.
5 Professor, Department of Cardiology, King George’s Medical University, Lucknow, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Monika Bhandari, Flat 103, Block A, Type 5, Doctor’s Residence, Jagat Narain Road, Chowk, Lucknow-226003, Uttar Pradesh, India.
E-mail: drmonikab@gmail.com
Percutaneous Transvenous Mitral Commissurotomy (PTMC) is the preferred treatment for isolated rheumatic valvular mitral stenosis if the valve has suitable anatomy. Following transseptal puncture, entry into left ventricle is the crucial step. This may be difficult in patients with large left atrium and very severe mitral stenosis. We are reporting a case of 23-year-old female suffering from mitral stenosis in which the mitral valve could not be crossed with standard technique, so a novel “over the wire technique” was used to cross the mitral valve and successful valvotomy was performed without any complication.
Accura Balloon, Balloon commisurotomy, Judkin’s Right Catheter, Mitral Stenosis
Case Report
A 23-year-old female, suffering from long standing effort dyspnea and palpitations due to Mitral stenosis for the past seven years. She was referred to the Cardiology Department for evaluation of further intervention. She was having New York Heart Association (NYHA) Class II-III dyspnea [1] despite maximal dose of loop diuretics (Furosemide) & beta blockers (Atenolol) on presentation. Her two dimensional echocardiogram revealed severe mitral stenosis (Mitral valve area by plaminetry- 0.6 cm2/ by presssure half time 0.7cm2) without any significant mitral regurgiation. Her Wilkin’s score [2] was 8/16 and left atrial size was 6.5 cmX5.5 cm. The mean gradient across the mitral valve was 25mmHg. Both commissures were free of any significant calcium. She also had moderate tricuspid regurgitation and moderate pulmonary hypertension. In view of favourable valve anatomy, a decision for PTMC was taken after obtaining an informed consent from the patient.
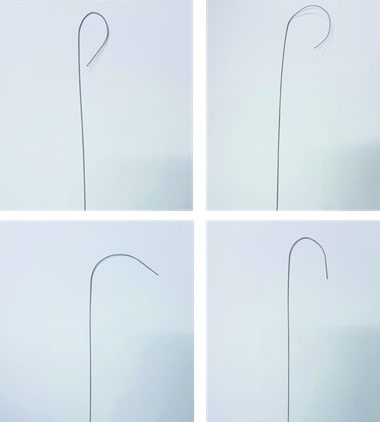
After arterial and venous access was obtained, a 6F pigtail catheter was placed in Aortic sinus to guide transpsetal puncture. Transseptal puncture was done under fluoroscopic guidance using Brockenbrough needle and a Curved spring wire introduced into Left Atrium (LA) following it [Table/Fig-1]. Body weight adjusted Intravenous heparin was administered at this point. We planned to use 26 mm Accura balloon (Vasular Concepts, Bangalore, India) to dilate the mitral valve. Using the standard principles, the prepared, sterile balloon was into LA with ease over the curved spring wire. Pressure recordings were done after pig tail was maneuvered into Left Ventricle (LV). Afterwards, an attempt was made to advance into the LV but the balloon could not cross the mitral valve using the standard sliding technique. We used different shaped stylets but of no avail [Table/Fig-2]. An attempt was made with the “reverse loop” technique, but the balloon failed to cross the mitral valve and enter LV.
After septal puncture curved spring wire placed in LA (white arrow). Pig tail cathter seen in situ in aortic sinus (black arrow);

Different shaped stylets used to cross mitral valve.
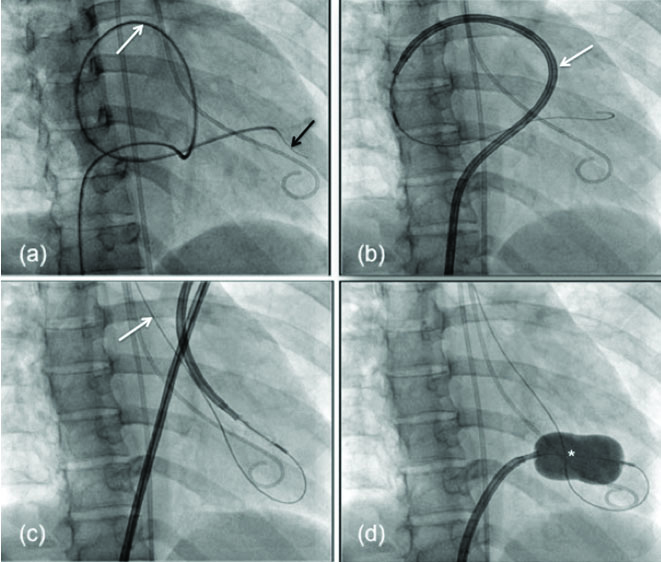
Following several failed attempts, we first exchanged the LV stylet with a 0.035”, 260 cm long exchange length hydrophilic glide wire (Terumo Inc., Japan) and then introduced judkins right diagnostic catheter over that wire and the balloon was removed. Using catheter support we introduced the hydrophilic wire first into LV making a reverse loop in LA [Table/Fig-3a]. The Accura PTMC balloon catheter then tracked over the hydrophilic glide wire into LA [Table/Fig-3b]. The same wire was advanced into the aorta across the aortic valve to support the balloon catheter passage across mitral valve [Table/Fig-3c]. The balloon took the reverse loop course of wire in the LA and crossed the mitral valve easily. The balloon was inflated at mitral valve to perform balloon commisurotomy [Table/Fig-3d]. Successful commissurotomy was documented with haemodynamic measurement and subsequent echocardiography [Table/Fig-4] without any complications. The normal procedural time is around 30 minutes but because of difficulty of the case, almost 30 minutes extra procedural time was needed for its successful completion.
(clockwise): 3a. Exchange length wire (black arrow) placed in LV using Judkins right catheter (white arrow) making a reverse loop in LA. 3b. Accuraballon (arrow) taken over the wire and placed in LA 3c. Balloon crossed into Left Ventricle with wire advanced into aorta for support (arrow) 3d. Balloon inflation (*) across mitral valve for final commisurotomy.
Haemodynamic and Echocardiographic recordings before and after PTMC.
| Haemodynamic Variables | Pre PTMC | Post PTMC |
|---|
| LA pressure (Mean) | 45 mm Hg | 25 mmHg |
| LA- LV Gradient (End Diastolic) | 20 mm Hg | 5 mmHg* |
| Mitral Valve area (echocardiographic) | 0.8cm2 | 1.45 cm2 |
| Mitral Reguritation(echocardiographic) | Trivial | Mild |
(LA- Left Atrium; LV- Left Ventricle; PTMC- Percutaneous Transmitral Commisurotomy)
*- gradient approached zero in long cardiac cycles after induced ventricular premature contractions.
The patient was discharged next day with low dose oral loop diuretics, oral betablocker and oral penicillin V. She was doing well on first and second visits at 2 weeks and 6 weeks respectively with improvement in dyspnea to NYHA class Ion low dose diuretics.
Discussion
PTMC is the preferred treatment for isolated rheumatic valvular mitral stenosis if the valve has suitable anatomy. During the procedure there are two crucial steps, first one being septal puncture and then entry into LV entry. The standard technique entails, placing the PTMC balloon (Inoue or Accura) in the LA following which a preshaped stylet is introduced into the balloon tip to guide the balloon into the LV. Low or medial position of septal puncture, altered left atrial geometry due to LA enlargement, or critical mitral stenosis may result in difficult LV entry. In our case, a dilated LA and low septal puncture led to difficulty in crossing the mitral valve.
Various modifications of the standard technique has been described for difficult LV entry like reverse loop technique, double loop technique, vertical approach using left ventricular pressure as a guide for LV entry [3-6]. An over the wire double-balloon technique of PTMC has been described, though with a slightly higher risk of left ventricular perforation [7]. Over the wire, single balloon technique using either the femoral or jugular approach has revealed good outcomes [8]. The over the wire multitrack system had fair results but the technique requires two balloons being simultaneously inflated in proper position making the technique challenging [9]. The Judkins right catheter, Amplatz right catheter or Swan – Ganz catheter may facilitate introducing the wire into the LV [10,11]. The hydrophilic wire is usually exchanged with stiffer wire for better support. Injury to the mitral chordal apparatus and the risk of ventricular arrhythmia are possible with the stiff wire, hence we elected to use the hydrophilic glide wire without exchanging for a stiffer wire. The techniques already described are to make a veno-arterial loop or place the wire tip at descending aorta [12,13].
In this case, we placed the wire tip in the descending aorta but by making reverse loop in LA using Judkins catheter and then exchanging it with Accura balloon catheter. Except for a few Ventricular Premature Contractions (VPC) during hydrophilic wire passage, there were no arrhythmias during balloon crossing. The presence of mechanical aortic prosthetic valve or LV mass or thrombus, are contraindications for this technique.
Conclusion
PTMC remains the mainstay of treatment of isolated mitral stenosis. There are two essential steps in PTMC; transeptal puncture and the balloon crossing into LV. Difficult balloon entry in the LV due to altered LA and septal anatomy can present technical challenges. The modified over wire technique may be a useful in such patients during PTMC when other techniques are not successful.
(LA- Left Atrium; LV- Left Ventricle; PTMC- Percutaneous Transmitral Commisurotomy)
*- gradient approached zero in long cardiac cycles after induced ventricular premature contractions.
[1]. The Criteria Committee of the New York Heart AssociationNomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels (9th ed.) 1994 BostonLittle, Brown & Co:253-256. [Google Scholar]
[2]. Wilkins GT, Weyman AE, Abascal VM, Block PC, Palacios IF, Percutaneous balloon dilatation of the mitral valve: an analysis of echocardiographic variables related to outcome and the mechanism of dilatationBr Heart J 1988 60(4):299-308.10.1136/hrt.60.4.2993190958 [Google Scholar] [CrossRef] [PubMed]
[3]. Ramamurthy S, Bahl VK, Manchanda SC, Successful Inoue balloon valvotomy in a difficult case of mitral stenosis using multiple modifications of technique: alternative method for loop formation of the Inoue balloon catheterJ Invasive Cardiol 2001 13(11):755-57. [Google Scholar]
[4]. Trehan V, Mehta V, Mukhopadhyay S, Yusuf J, Kaul UA, Difficult percutaneous transvenous mitral commissurotomy: a new technique for left atrium to left ventricular entryIndian Heart J 2004 56(2):158-62. [Google Scholar]
[5]. Hung JS, Lau KW, Vertical approach – a modified method in balloon crossing of mitral valve in Inoue balloon mitral valvuoplastyJ Invasive Cardiol 1998 10(9):548-50. [Google Scholar]
[6]. Safi AM, Kwan T, Clark LT, Successful percutaneous balloon mitral Valvuloplasty using left ventricular pressure as a guide to cross the mitral valve – a case reportAngiology 2000 51(1):83-86.10.1177/00033197000510011310667647 [Google Scholar] [CrossRef] [PubMed]
[7]. Manjunath CN, Srinivasa KH, Patil CB, Venkatesh HV, Bhoopal TS, Dhanalakshmi C, Balloon mitral valvuloplasty: our experience with a modified technique of crossing the mitral valve in difficult casesCatheter CardiovascInterv 1999 46(1):117-18.10.1002/(SICI)1522-726X(199901)46:1<117::AID-CCD30>3.0.CO;2-Q [Google Scholar] [CrossRef]
[8]. Dani S, Patel TM, Chag MC, Thakore SB, Patel TK, Difficult mitral valvuloplasty: an over the wire modification of Inoue techniqueJ Invasive Cardiol 1995 7(5):148-51. [Google Scholar]
[9]. Bonhoeffer P, Esteves C, Casal U, Tortoledo F, Yonga G, Patel T, Percutaneous mitral valve dilatation with the Multi-Track systemCatheter CardiovascInterv 1999 48(2):178-83.10.1002/(SICI)1522-726X(199910)48:2<178::AID-CCD11>3.0.CO;2-5 [Google Scholar] [CrossRef]
[10]. Meier B, Modified Inoue technique for difficult mitral balloon commissurotomyCathet Cardiovasc Diagn 1992 26(4):316-18.10.1002/ccd.18102604141394421 [Google Scholar] [CrossRef] [PubMed]
[11]. Deora S, Vyas C, Shah S, Percutaneous transvenous mitral commissurotomy – a modified over-the-wire technique for difficult left ventricle entryJ Invasive Cardiol 2013 25(9):471-73. [Google Scholar]
[12]. Mehan VK, Meier B, Impossibility to cross a stenotic mitral valve with the Inoue balloon: success with a modified techniqueIndian Heart J 1994 46(1):51-52. [Google Scholar]
[13]. Ates I, Ulucan S, Kaya Z, Doğru M, Katlandur H, Keser A, New technique of challenging cases of percutaneous balloon mitral Valvuloplasty: the venoarterial loopingAnatol J Cardiol 2015 15:426-29.10.5152/akd.2015.612725993719 [Google Scholar] [CrossRef] [PubMed]