Laparoscopic Simple Nephrectomy in a Severe Kyphoscoliotic Patient
Sandeep Gupta1, Alankar Jaiswal2, Dilip Kumar Pal3
1 Assistant Professor, Department of Urology, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
2 Post Doctoral Trainee, Department of Urology, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
3 Professor, Department of Urology, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dilip Kumar Pal, Institute of Post Graduate Medical Education and Research, 244, AJC Bose Road, Kolkata-700020, West Bengal, India.
E-mail: urologyipgmer@gmail.com
Laparoscopic surgery in patients with spinal deformity are always challenging to surgeons due to unpredictable position of viscera inside abdomen and lack of working space within the abdomen. We are reporting a case report of laparoscopic simple nephrectomy in a patient with severe kyphoscoliosis who presented with symptoms of flank pain and imaging showed non-functioning kidney.
Hydronephrotic, Hyperextension, Transperitoneal
Case Report
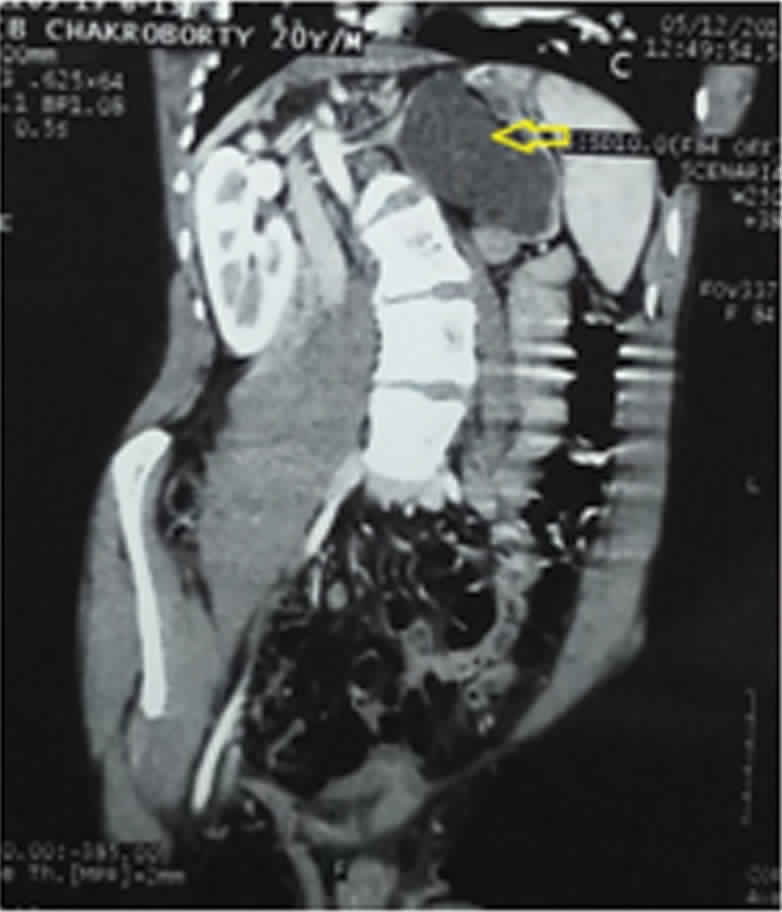
A 20-year-old boy was admitted in our hospital with complaint of left flank pain since six months. There was history of breathelessness since childhood. There was no history of hypertension or any neurological disorders. There was no history of haematuria. He had gross kyphoscoliosis towards right side [Table/Fig-1]. The patient suffered from grade 4 kyphoscoliosis and a spine curvature of 85 degrees. Abdominal and genital examination was unremarkable. Ultrasound examination showed grossly hydronephrotic left kidney with thinned out parenchyma. Computed tomography showed Grade 4 hydronephrosis [1] of left kidney with opposite kidney being normal [Table/Fig-2]. Diethylene Triamine Pentaacetic Acid (DTPA) scan showed absent function on left side. Despite severe kyphoscoliosis, we planned for laparoscopic left trans-peritoneal nephrectomy.
X-ray image of chest and abdomen PA view showing severity of kyphoscoliosis.

CT image of patient showing grossly hydronephrotic left kidney (yellow arrow) with normal right kidney.
Surgical Procedure
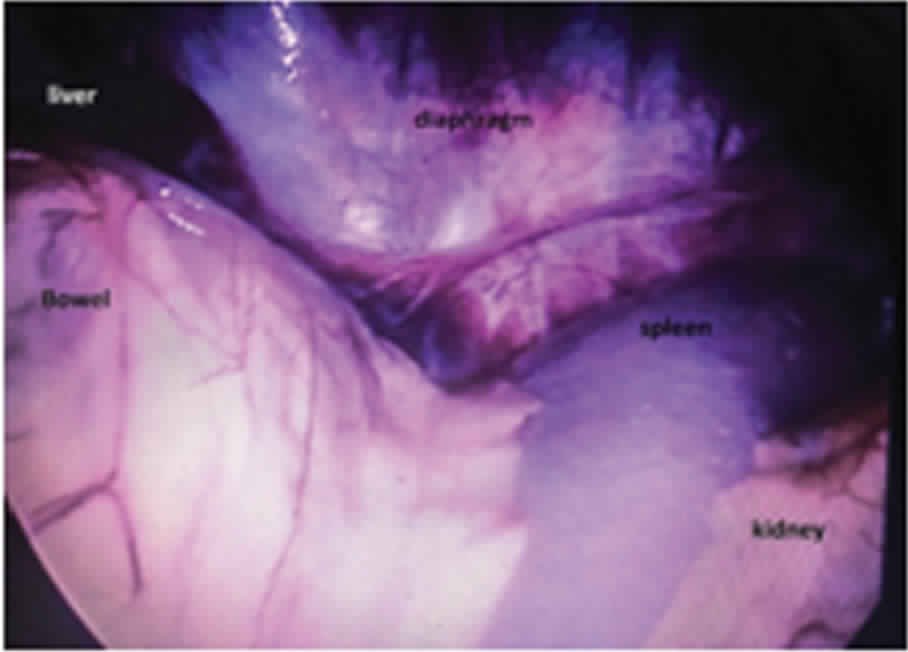
Patient was posted for surgery after taking proper informed consent. The patient was intubated in lateral position because he could not be kept in complete supine position. Care was taken to avoid hyperextension of spine. Under general anaesthesia, position of patient was right lateral with table bent at ends [Table/Fig-3]. We performed Hasson’s open technique [2] for introduction of first 10 mm port which was used as camera port. The pneumoperitoneum was established and a pressure of 14 mm Hg was maintained. One additional 5 mm trocar on the left and a 10 mm trocar on the right were inserted under vision. Position of ports is shown in [Table/Fig-4]. After entering abdomen with no difficulty, position of viscera is shown in [Table/Fig-5]. After access and pneumoperitoneum, firstly, left colon was mobilized by dissecting line of Toldt and deflected medially and then left ureter identified and dissected upwards. In this case, kidney and ureter were found more medial and superior than normal. The safest way to explore the renal hilum was to explore and suspend the ureter first. After dissection, the left kidney was identified and dissected, and it was found to be small in size. Left gonadal vein was clipped and cut. Then left renal artery and vein were separately dissected, clipped and cut. Then, left ureter was clipped and cut. One drain was placed in renal fossa. Hemostasis was achieved and ports were closed. The operation was completed successfully without need of conversion. Total operation time was 180 minutes and blood loss was 100 mL. The drain was removed on second postoperative day and patient was discharged on fourth postoperative day. Patient was followed up after one month of surgery, and then at three months and six months, and was doing well.
Patient’s position during intubation.

Port positions in patient (centre one is camera port 10 mm, left port is 10 mm working port and right one is 5mm working port).

Picture showing position of viscera inside abdomen.
Discussion
Kyphoscoliosis is an abnormal curvature of spine in both coronal and sagittal plane. Usually this disease is associated with many syndromes such as Ehlers Danlos syndrome, Friedrich’s ataxia, Duchenne muscular dystrophy and Syringomelia. Kyphoscoliosis is graded by measuring Cobb’s angle and classified as mild (11–25 degrees), moderate (25–50 degrees), or severe (>50 degrees) [3]. The Cobb’s angle can be correlated with the pulmonary function tests where Cobb’s angle above 60 degrees is associated with progressive pulmonary and cardiac failure.
Laparoscopic nephrectomy in a kyphoscoliotic patient is a challenging procedure both from surgical as well as anaesthetic point of view. It is the standard procedure which is done in case of symptomatic non-functioning kidney. It can be done either by open approach or laparoscopic approach. Laparoscopic approach can be either transperitoneal or retroperitoneal. We have described transperitoneal approach above. Regarding anaesthesia, intubation and patient positioning is a major issue. Regarding surgery, determining kidney location and performing hilar dissection can be a difficult proposition. Complications during and after transperitoneal laparoscopic surgery in urology remain low and are not superior to those observed during and after open surgery [4]. Transperitoneal approach has a advantage of more working space in relation to retroperitoneal approach [5].
There is difficulty in access to intra-abdominal organs in patients with severe kyphoscoliosis as the organs are covered by low-lying thoracic cage. But in some papers, there are reports where access to intra-abdominal organs became possible despite fixed rigidity and anatomical difficulty [6-8].
Altered anatomy in case of severe kyphoscoliotic patient is the major cause of conversion in laparoscopic surgery [9]. In these types of patients, easiest way to reach upto kidney is to identify ureter first, hold it and trace it upto renal hilum. A rigorous preoperative visualization of the vascular anatomy is obligatory to prevent major vascular injury, which has a reported incidence of 2% in transperitoneal laparoscopic nephrectomy [10].
Altered anatomy also causes difficult intubation in these patients which causes major problem in giving anaesthesia to patients. Preoperative optimization of respiratory condition in these patients is necessary as usually these patients are suffering from restrictive lung disease. Postoperative period warrants a good intensive care and incentive spirometry to optimize this.
Conclusion
Laparoscopic surgery in a kyphoscoliotic patient is a challenging procedure. In experienced expert hands, it can be done, keeping in mind the possible difficulties and complications both during and after operation. It is not, however, an absolute contraindication to laparoscopy.
[1]. Beetz R, Bökenkamp A, Brandis M, Hoyer P, John U, Kemper MJ, Diagnosis of congenital dilatation of the urinary tract. Consensus Group of the Pediatric Nephrology Working Society in cooperation with the Pediatric Urology Working Group of the German Society of Urology and with the Pediatric Urology Working Society in the Germany Society of Pediatric SurgeryUrologe A 2001 40(6):495-507. [Google Scholar]
[2]. Hasson HM, A modified instrument and method for laparoscopyAm J Obstet Gynecol 1971 110:886-87.10.1016/0002-9378(71)90593-X [Google Scholar] [CrossRef]
[3]. Bowens C, Dobie KH, Devin CJ, Corey JM, An approach to neuraxial anaesthesia for the severely scoliotic spineBr J Anaesth 2013 111(5):807-11.10.1093/bja/aet16123661407 [Google Scholar] [CrossRef] [PubMed]
[4]. Vallancien G, Cathelineau X, Baumert H, Complications of transperitoneal laparoscopic surgery in urology: review of 1,311procedures at a single centerJ Urol 2002 168:23-26.10.1016/S0022-5347(05)64823-9 [Google Scholar] [CrossRef]
[5]. Breda A, Finelli A, Janetschek G, Complications of laparoscopic surgery for renal masses: prevention, management, and comparison with the open experienceEur Urol 2009 55:836-50.10.1016/j.eururo.2009.01.01819168276 [Google Scholar] [CrossRef] [PubMed]
[6]. Kuroki T, Tajima Y, Tsuneoka N, Adachi T, Kanematsu T, Rib-lifting method for retraction of the low-lying costal arch in laparoscopic cholecystectomy of gallbladder torsion with KyphoscoliosisHepatogastroenterology 2009 56:1268-69. [Google Scholar]
[7]. Chowbey PK, Panse R, Khullar R, Sharma A, Soni V, Baijal M, Laparoscopic cholecystectomy in a patient with ankylosing spondylitis with severe spinal deformitySurg Laparosc Endosc Percutan Tech 2005 15:234-37.10.1097/01.sle.0000174571.66301.8d16082313 [Google Scholar] [CrossRef] [PubMed]
[8]. Sato T, Yamaguchi S, Ozawa S, Ishii T, Tashiro J, Hosonuma T, Is laparoscopic surgery a contraindication in patients with severe senile kyphosisHepatogastroenterology 2010 57:1095-98. [Google Scholar]
[9]. Ivey BS, Lucas SM, Meyer CA, Conversions in laparoscopicrenal surgery: causes and outcomesJ Endourol 2011 25:1167-73.10.1089/end.2010.072521671761 [Google Scholar] [CrossRef] [PubMed]
[10]. Kim BS, Yoo ES, Kwon TG, Complications of transperitoneal laparoscopic nephrectomy: a single-center experienceUrology 2009 73:1283-87.10.1016/j.urology.2009.01.01719362334 [Google Scholar] [CrossRef] [PubMed]