Traumatic Abdominal Wall Hernias-An Uncommon Case Series
G Vijayalakshmi1, L Arun Kumar2
1 Assistant Professor, Department of General Surgery, ESIC Medical College and PGIMSR, Chennai, Tamil Nadu, India.
2 Postgraduate Student, Department of General Surgery, Rajiv Gandhi Government General Hospital and Madras Medical College, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. G Vijayalakshmi, 47, Annaji Nagar, KK Nagar West, Chennai-600078, Tamil Nadu, India.
E-mail: vijayalakshmi.gunasekaran88@gmail.com
A case series of abdominal wall hernia following blunt injury is essential for the understanding of its varied clinical presentation. The purpose of this paper is to emphasise on the fact that abdominal wall hernia is seemingly benign yet completely treatable condition and can be easily missed without proper clinical examination. A timely intervention with proper intraoperative assessment and decision making is needed. Immediate primary tissue repair is the preferred mode of management. Laparoscopic intervention in these scenarios is possible with better knowledge of the mechanism of injury and probable outcomes.
Blunt injury, Mesh repair, Traumatic hernias
Case Series
CASE-1
A 21-year-old male sustained handlebar injury to the abdomen. The site of impact was in the Right Iliac Fossa (RIF). He presented to the emergency department with abdomen pain and palpable defect in the RIF region [Table/Fig-1]. Cough impulse was present. There were no other external injuries and he was haemodynamically stable. Focused Assessment with Sonography for Trauma (FAST) was done to rule out the other injuries. He was taken up for emergency surgery. Incision was made over the site of swelling and defect identified. Mesenteric tear was encountered intraoperatively and repaired. Defect closed by primary tissue repair. Patient had an uneventful recovery. No complications were noted in follow-up period of six months.
Clinical pictures of all four patients at the time of presentation.

Case - 2
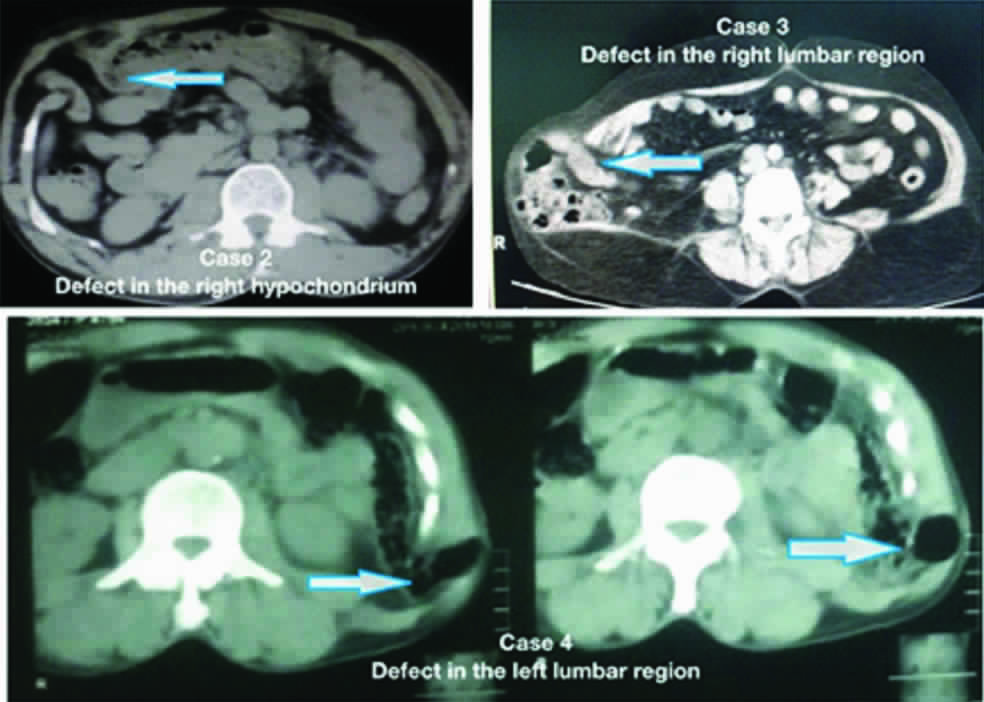
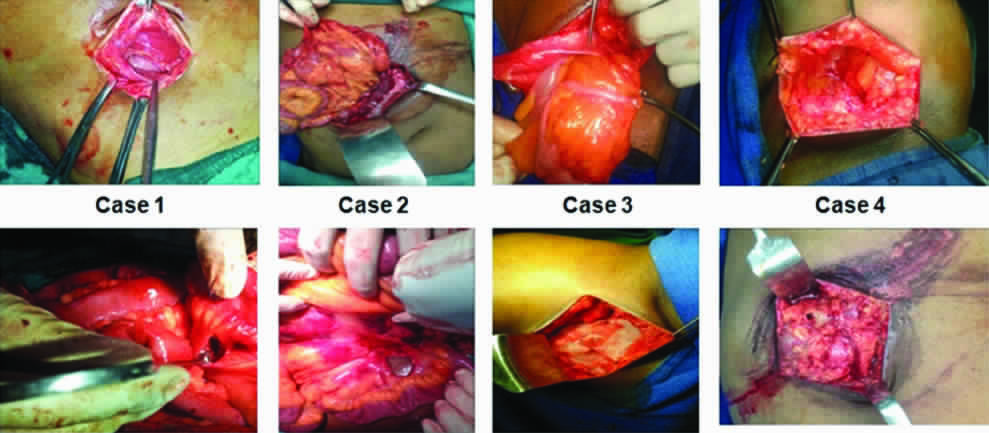
A 27-year-old male patient had a fall from a two-wheeler with impact in the right hypochondrium and was brought to emergency department. Examination revealed generalised tenderness and a palpable defect. Contrast Enhanced Computerised Tomogram (CECT) abdomen was done revealing herniation of bowel through a muscular defect [Table/Fig-2]. He was taken up for emergency laparotomy, done through an incision over the defect. Intraoperatively, mesenteric tear with small bowel contusion was noted. Primary tissue repair was completed [Table/Fig-3]. No complications were noted in the ten days postoperative period.
CT Abdomen images of the patients showing muscular defect with bowel herniation corresponding to the site of injury.
Intraoperative pictures showing the defect and presence of any associated injury.
Case - 3
A 34-year-old male patient had a road traffic accident with blunt injury on his right lumbar region. On examination, there was a reducible swelling and a palpable defect at the same site [Table/Fig-1]. CECT abdomen was done, showing a lumbar hernia [Table/Fig-2]. He was taken up for emergency surgery. Incision was placed over the swelling, and abdomen opened. No bowel or solid organ injury was noted. Mesh repair was done [Table/Fig-3]. Postoperative recovery was complete and uneventful during the follow up period of six months.
Case-4
A 60-year-old male, was admitted with history of fall from two wheeler and blunt injury to left lumbar region [Table/Fig-1]. No other external injuries were noticed. Examination revealed a palpable reducible swelling. CECT abdomen was done which showed left lumbar hernia [Table/Fig-2]. Emergency surgery was performed. There was no intra abdominal injury. Primary tissue repair was done [Table/Fig-3]. He had uneventful postoperative recovery and was followed up for a period of six months.
Discussion
Traumatic Abdominal Wall Hernia (TAWH) goes by the following definition-“herniation through disrupted musculature and fascia, associated with adequate trauma, without skin penetration and no evidence of any prior hernia defect at the site of injury”. These hernias are rare presentations of blunt trauma to abdomen and prevalence is less than 1% even in dedicated trauma centres [1]. Here, we present four cases of abdominal wall hernia following blunt injury to the abdomen.
TAWH was first described by Selby in 1906. Handlebar hernia is an even rarer entity. It was first described by Dimyan et al., in 1980. TAWHs are rare entities and provide a challenge both in terms of diagnosis and surgical management. The mechanisms responsible for these herniations are not well defined but three possible hypotheses have been postulated. A blunt direct force to the abdominal wall causing disruption or a sudden increase in intra-abdominal pressure force following fall from height and the most commonly accepted theory of an acceleration-deceleration, ‘shear and compressive’ force in high velocity injuries. These forces result in disruption of the muscular wall while the skin being more elastic remains intact [2,3].
Diagnosis is usually evident by clinical examination. The most common differential diagnosis is abdominal wall hematoma. In unclear cases imaging like Ultrasound (USG) of abdomen or CECT abdomen can aid in the diagnosis. CT of abdomen is also indicated to rule out other associated solid organ injuries and intra abdominal injuries in case of high velocity injuries or in an unstable patient [4]. Most cases do not have significant intra abdominal injuries. Most common reported injuries are serosal tears and mesenteric tears. Very few have sustained bowel perforations, usually ileal. In this series USG was done in one patient and CT abdomen in the other three cases.
Prompt surgery is usually advised even in stable patients. Studies comparing primary vs. delayed repair shows no benefit in the latter [5]. Another controversy has been regarding the placement of incision-midline laparotomy vs. incision over the hernial site. Several case series have shown that incision can be taken directly over the hernia aids in proper reinforcement of the hernia defect [6]. Formal laparotomy can be done in emergent situations or in case of proven associated bowel injury. Similarly primary repair with non absorbable or delayed absorbable sutures is found to be sufficient. In elderly patients, mesh repair is preferred because of the weakness in anterior abdominal wall in order to prevent recurrence. We have done primary repair through the hernial wound in all our patients. Laparoscopic repair have been found to be effective in isolated injuries and in delayed repairs [7].
Complications in terms of wound infection or recurrence of hernia are rare and have not been reported. Mortality or morbidity is due to associated injuries [8]. All our patients were doing well with no complications at six months of follow up.
Conclusion
TAWHs are uncommon and require high index of suspicion. USG and CT are the preferred imaging modalities. Surgery is the main stay of management. Early intervention is ideal. Layer by layer primary suture repair through incision over the hernial defect is preferred in cases of isolated hernias.
[1]. Netto FA, Hamilton P, Rizoli SB, Nascimento Jr B, Brenneman FD, Tien H, Traumatic abdominal wall hernia: epidemiology and clinical implicationsJ Trauma 2006 61:1058-61.10.1097/01.ta.0000240450.12424.5917099509 [Google Scholar] [CrossRef] [PubMed]
[2]. Nishimura T, Nakao A, Okamoto A, Fujisaki N, Kotani J, A case of traumatic abdominal wall hernia with delayed bowel obstructionSurg Case Rep 2015 1(1):1510.1186/s40792-015-0023-726943383 [Google Scholar] [CrossRef] [PubMed]
[3]. Mahajana A, Ofer A, Krausz MM, Traumatic abdominal hernia associated with large bowel strangulation: case report and review of the literatureHernia 2004 8:80-82.10.1007/s10029-003-0155-814634840 [Google Scholar] [CrossRef] [PubMed]
[4]. Lane CT, Cohen AJ, Cinat ME, Management of traumatic abdominal wall herniaAm Surg 2003 69:73-76. [Google Scholar]
[5]. Wilson KL, Davis MK, Rosser Jr JC, A traumatic abdominal wall hernia repair: a laparoscopic approachJSLS 2012 16:287-91.10.4293/108680812X1342798237734623477181 [Google Scholar] [CrossRef] [PubMed]
[6]. Yadav S, Jain SK, Arora JK, Sharma P, Sharma A, Bhagwan J, Traumatic abdominal wall hernia: delayed repair: advantageous or taxingInt J Surg Case Rep 2013 4:36-39.10.1016/j.ijscr.2012.10.00423103630 [Google Scholar] [CrossRef] [PubMed]
[7]. Munshi IA, Ravi SP, Earle DR, Laparoscopic repair of blunt traumatic abdominal wall herniaJSLS 2002 6:385-88. [Google Scholar]
[8]. Kumar A, Hazrah P, Bal S, Seth A, Parsad R, Traumatic abdominal wall hernia: a reappraisalHernia 2004 8:277-80.10.1007/s10029-003-0203-414735329 [Google Scholar] [CrossRef] [PubMed]