The frequency of treatment of lesions of the liver by various new treatment modalities has increased during the recent years. Wide variations in the branching pattern of the LHV and MHV can pose a problem during surgeries in the liver. Therefore, a comprehensive study about the pattern of branching of these veins is very important.
The left lobe of the liver is mainly drained by the MHV and the LHV which are tributaries from the IVC. The left lobe of the liver has left lateral and left medial segments. The left lateral is again divided into the left lateral superior and lateral inferior sub-segments. The medial segment is divided into medial superior and medial inferior segments. The LHV drains the left lateral superior and lateral inferior segments [1].
The MHV drains the left medial segment of the left lobe and the right anterosuperior segment of the right lobe of the liver. The MHV runs in the lobar fissure. Lobar fissure is an imaginary line which is formed by plane which passes through fossa of gallbladder and along the groove for the inferior vena cava [1].
It has also been seen that MHV can be included in right lobe Live Donor Liver Transplantation (LDLT) which is very safe [2].
The LHV runs in an intersegmental border formed by a plane between left lateral superior and lateral inferior segments of the left lobe [3,4].
Previous studies suggested that a stump of at least 1 cm was necessary for successful clamping and ligature of the veins during various surgeries. So, preoperative assessment of tributary free part of the LHV and MHV before they drain into the IVC is important [5,6].
There are wide variations in the drainage pattern of the LHV and MHV, the knowledge of which is very important to prevent any unforeseen complications during various surgeries.
The LHV and MHV which usually forms common trunk before entering the IVC exhibit variations. Careful assessment of the pattern of confluence of LHV and MHV is pivotal for successful resection of liver [7].
The present study was done on cadaveric livers to find out the variations in the drainage pattern of the LHV and MHV and to see the branching pattern of the tributaries and whether they drained at a distance of more than 1 cm from the IVC.
Materials and Methods
The study was a institution based descriptive study conducted on 60 adult human livers in Lady Hardinge Medical College, Delhi, India, from January 2008 to December 2015. The sample size was decided as per the availability of livers. Any liver with obvious pathology was excluded from the study. The livers were removed from adult human cadavers fixed by the perfusion of 10% formalin solution through the femoral artery and was preserved for minimum one week. Each specimen of liver was dissected precisely from the visceral surface maintaining the diaphragmatic surface and the original shape of the liver intact. The liver parenchyma was removed with the help of dissection forceps.
The LHV and the MHV were studied. Vessels were cut at the point of ramification to view inside the vascular lumen, to confirm the pattern of formation of common trunk by LHV and MHV. The pattern of confluence of middle and LHVs into the inferior vena cava was noted. Any variation in the pattern of confluence was noted. Diameter of hepatic veins were measured (in millimetres) at the point before the formation of common trunk. In cases where separate trunks of LHV and MHV were emptying into IVC, the diameter was measured at point before they entered the IVC. The diameter of common trunk was taken at point before it entered the IVC. The length of common trunk was taken from the point where the LHV and MHV joined to form common trunk till the confluence of the trunk with IVC. The measurements were done using vernier calipers or calibrated divider.
Analysis of the tributaries was done to see whether they were emptying into the common trunk or into the LHV or MHV within a distance of less than 1 cm from the IVC. The tributaries which had diameter >2 mm were taken into account. The LHV and MHV were classified according to the pattern of ramification of the tributaries.
Results
The MHV and the LHV were identified in the left lobe of the livers to see whether they were running in the segmental borders. The LHV was seen to lie in segmental border in 42 (70%) of the livers. In these livers there was one main trunk of LHV running in the segmental plane and tributaries from the left lateral superior and lateral inferior were joining the trunk in random manner. In 18 of the livers, LHV did not lie in the segmental plane (30%). This arrangement was seen in livers where instead of bifurcation pattern of the LHV and MHV, trifurcation pattern was seen. The trifurcation was formed either by LHV, MHV and one of the tributaries of the LHV or by the tributaries of the LHV with the MHV. In some cases, no trunk of the LHV was seen. The MHV was found running along the lobar fissure in all livers. The mean diameter of the MHV was found to be 10.3±2.47 mm. The mean diameter of the LHV was found to be 11.7±2.24 mm.
The tributaries of the LHV and the MHV were identified. The tributaries of the LHV were left superior and left inferior draining the respective left superior and left inferior segments of the left lobe. The LHV was giving Lateral Medial (LM) branch to the medial intersegmental area which corresponds to the quadrate lobe of the liver. The MHV was seen draining the medial segment of the left lobe and the Right Anterosuperior Segment (RAS) of the right lobe of the liver. Care was taken to see that whether this vein joined the MHV at a distance <1 cm or more from the IVC. In most of the livers the LHV and MHV formed a common trunk, which joined the IVC (n=46, 76.6%). In some cases, they drained independently into IVC (n=12, 20%). In few cases (n=2, 3.33%), trunk of LHV was absent, instead the left lateral and left medial directly entered the IVC without joining to form LHV [Table/Fig-1]. Variations were seen in the pattern by which the tributaries were draining into the LHV and MHV. And also the pattern of drainage of the tributaries differed in different livers.
Incidence of common trunk of LHV and MHV.
| Pattern | Number of cases | Percentage (%) |
|---|
| Common trunk |
| Total | 46 | 76.6 |
| <1 cm | 40 | 66.66 |
| >1 cm | 6 | 10 |
| Separate single trunk of LHV and MHV | 12 | 20 |
| LHV absent | 2 | 3.33 |
As mentioned earlier, a space of 1 cm was necessary for the ligation of the hepatic vein in the transection of the liver, the MHV and LHV were classified into four types according to the patterns of ramifications of the veins within 1 cm from the IVC. The four types were again sub-typed according to the tributaries draining the veins.
Type I (n=6, 10%): The LHV and MHV formed a common trunk. The common trunk had no tributary within less than 1 cm from the IVC, in other words the length of the trunk was >1 cm [Table/Fig-2]. In these livers the LHV was seen running in an intersegmental border between the lateral superior and lateral inferior segment. There were numerous tributaries from the lateral superior and lateral inferior in random fashion.
Type I, Common trunk of LHV & MHV more than 1cm.
LHV: Left Hepatic Vein; MHV: Middle Hepatic Vein; CT: Common Trunk; LPV: Left Portal Vein

Type II (n=30, 50%), was seen having a confluence of LHV and MHV within 1cm from the IVC. This type was further subtyped into three types.
Type IIa (n=22, 73.3%), was formed when middle and LHV was seen forming a common trunk at a distance of less than 1cm from the IVC.
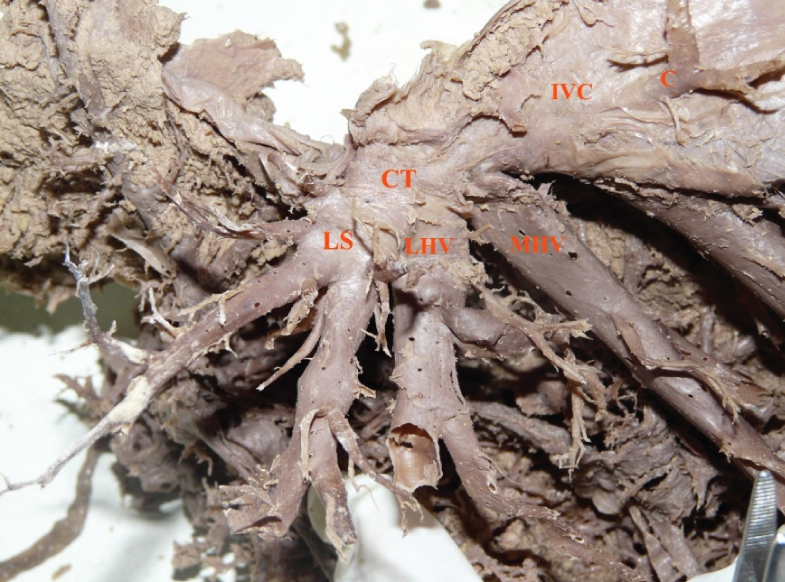
In Type IIb (n=2, 6.66%), common trunk was seen at a distance <1 cm and left superior vein were seen entering the IVC directly. The left superior vein which is coming from the left lateral superior segment of the left lobe is a tributary of the LHV [Table/Fig-3].
Type IIb, Common trunk of LHV and MHV at less than 1 cm from IVC. Left superior joining the common trunk at distance less than 1cm from the IVC. LHV: Left Hepatic Vein; MHV: Middle Hepatic Vein; IVC: Inferior Vena Cava; LS: Left Superior Vein; CT: Common Trunk

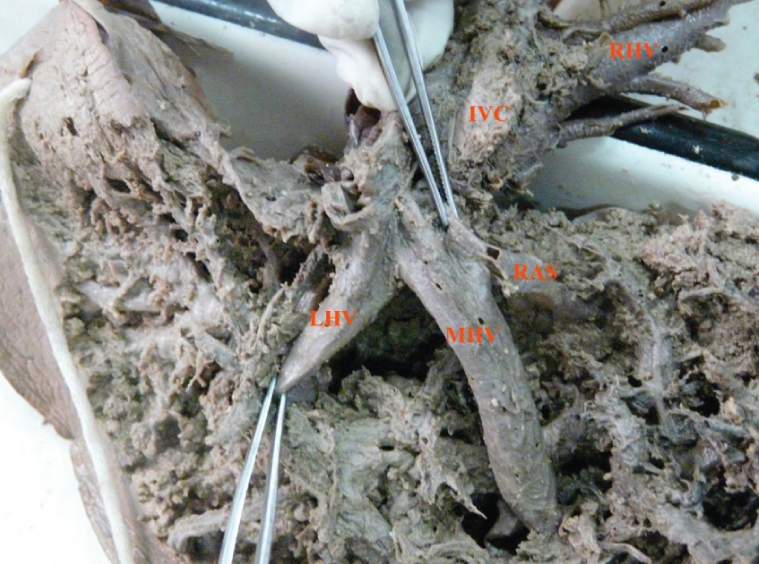
In Type IIc (n=6, 20%), common trunk had length <1cm, but a branch from RAS segment of the right lobe of liver was seen into flowing into MHV at a distance of less than 1 cm from the IVC [Table/Fig-4].
Type IIc, Common trunk of LHV and MHV and RAS at distance less than 1 cm from the IVC.
LHV: Left Hepatic Vein; MHV: Middle Hepatic Vein; RAS: Right Antero-Superior Vein
In Type III, the pattern of confluence seen was trifurcation pattern. This type was further subdivided into types IIIa and IIIb.
In Type IIIa (n=10, 83.3%), a confluencing pattern which looked more like a trifurcation pattern was seen within a distance of 1 cm from the IVC. In this case, the confluence was formed by joining of MHV, LHV and a large vein from the left lateral superior subsegment, the left superior vein. The left superior was seen draining the left lateral superior segment of the left lobe. Here the common trunk was formed by all these three veins and the length of the trunk was <1 cm [Table/Fig-5].
Type IIIa, Trifurcation pattern formed by LS, LHV and MHV at a distance less than 1cm.
LS: Left Superior; LHV: Left Hepatic Vein; MHV: Middle Hepatic Vein
In type IIIb: (n=2, 16.6%) In this type the main trunk of the LHV was not seen. Instead, a trifurcation pattern was seen formed by a vein from the left lateral segment, a vein from the left medial segment and the MHV. The left lateral and left medial veins did not join to form LHV, but joined the MHV to form a trifurcation pattern [Table/Fig-6].
Type IIIb, Trifurcation pattern formed by Left Lateral (LL), Left Medial (LM) and MHV.

Type IV had independent trunks of LHV and MHV draining separately into IVC. This type was further subtyped into two types, Type IVa and IVb.
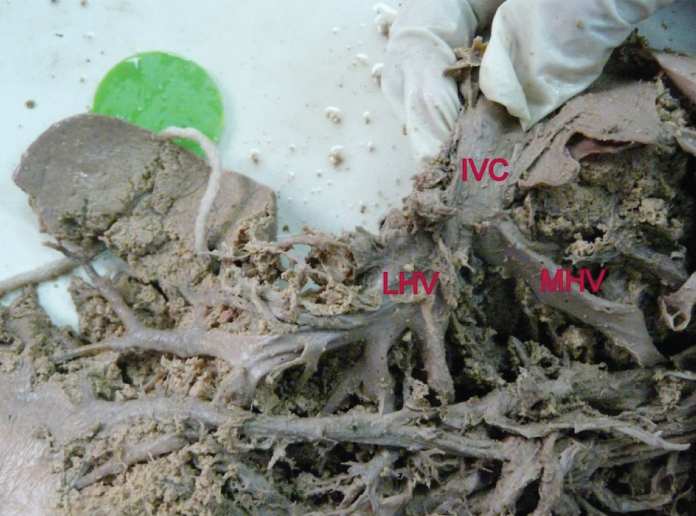
Type IVa (n=6, 50%): In this type, the common trunk of LHV and MHV was not seen. The LHV and MHV were draining independently directly into the IVC. There were no tributaries of LHV and MHV draining into them at a distance less than 1cm from the IVC [Table/Fig-7].
Type IVa, MHV and LHV draining separately into IVC.
Type IVb (n=6, 50%): Independent left and MHVs were seen but RAS vein coming from the right anterosuperior segment of the right lobe of liver was flowing into the MHV at distance less than 1cm from the IVC [Table/Fig-8].
Type IVb, MHV and LHV draining separately into IVC with RAS draining into MHV at a distance less than 1cm. LM: Left Medial.

Drainage of caudate lobe: The drainage of the caudate lobe was classified according to the number of veins draining the caudate lobe. The veins were usually coming from the IVC directly. The size of the veins ranged from pin hole sized to 6 mm in diameter. They were classified into:
Type I (n=36, 60%): was seen having one vein draining into IVC;
Type II (n=20, 33.3%): was seen having two veins draining into IVC;
Type III (n=4, 6.66%): was seen having multiple veins draining into IVC.
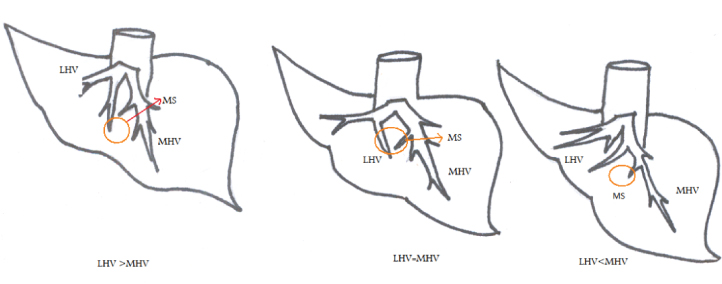
Drainage of intersegmental area: The drainage of the medial segmental area was noted carefully. The quadrate lobe of the liver falls in this segment of the left lobe. The medial segment is further subdivided into medial superior and medial inferior segments. The tributaries of LHV and the MHV were seen draining this area. In some livers, the contribution from the LHV seemed to be more but in others contribution from the MHV was dominant. In 10% cases it was shared equally by MHV and the LHV [Table/Fig-9].
Drainage of medial superior area.
MS: Medial Superior Area, LHV: Left Hepatic Vein, MHV: Middle Hepatic Vein
Discussion
In the present study, it was seen that the location of the hepatic veins was useful in identifying the segments. The MHV was lying along the lobar fissure. The same was found in the studies done by other researchers [8,9].
It has been reported in previous study that MHV can serve as landmark for right and left hepatectomy because MHV lies in the midplane of liver. So, proper evaluation of MHV is crucial for safe liver resection [10].
The diameters of the MHV and LHV were noted and compared to various previous studies [Table/Fig-10] [11-13]. Previous researchers found that before transection of the veins it is important to close the veins with running suture [6].
Comparison of diameters of LHV and MHV with other researchers [11-13].
| Studies Done | LHV | MHV |
|---|
| Present study | 8-16 mm (11.7±2.24mm) | 6-16 mm (10.3±2.47 mm) |
| Appel M et al., [11] | 10 mm | 10 mm |
| Wind P et al., [12] | 8.7±1.8 mm | 8.6±2 mm |
| Ortale JR et al., [13] | 10.7±2.4 mm | 10.0±2.5 mm, |
LHV: Left Hepatic Vein; MHV: Middle Hepatic Vein
The hepatic veins were classified according to the distance of the first tributary from the IVC which should be at least 1 cm as the previous researchers highlighted in their studies that a length of minimum 1 cm should be present for the proper ligation of the hepatic veins before their transaction [5,14]. Lacerations of hepatic veins have to be prevented because it can cause massive bleeding which can lead to cardiac arrest or air embolism [15].
Researchers also suggested that prevention of the pushing of cancer cells into the veins can be prevented by ligation of veins prior to transection of liver [16].
The middle and LHVs presented as a common trunk in 76.6% of the livers (46 cases) in the present study. The prevalence of common trunk was compared with that of other researchers [5,15,17-20] [Table/Fig-11]. The difference in the percentages in present study and the other workers could be because of difference in the sample size and the population from which the cases were taken. The high prevalence of the combined trunk of the left and MHVs makes these veins vulnerable to injury during surgery. So, the knowledge of these veins is very important during surgeries of liver.
Comparison of frequency of common trunk with other researchers [5,13,17-20].
| Studies done | Prevalence (%) |
|---|
| Present study | 76.6 |
| Baird RA et al., [17] | 96 |
| Nakamura S et al., [5] | 84.34 |
| Cheng YF et al., [18] | 70 |
| Ortale JR et al., [13] | 77.5 |
| Fang CH et al., [19] | 61 |
| Wenli XU et al., [20] | 52 |
Embryological basis for the presence of common trunk: The reason for high incidence of the common trunk (76.36%) can be hypothesised on basis of embryological development of these veins. Veins known as the right vitelline veins give rise to the right hepatic vein in the right lobe of the liver and the left vitelline veins give rise to one vein on the left side. It is possible that the vein on the left side is the common trunk which is formed by the confluence of the middle and the LHVs. Hence, this can be one hypothesis for the presence of the common trunk. The above mentioned embryological basis for the presence of the common trunk has not been mentioned in the studies done by any of the researchers. It can also be hypothesised that if a communication of sinusoid (vene revehentes) near the left vitelline vein (LHV) persists, it can attribute to the formation of independent trunks of MHV and the LHV.
An alternative explanation for the presence of the different patterns of the hepatic veins of the left lobe could be described on the basis of Dickson’s AD explanation [21]. He postulated that there are two main anastomoses present in relation to the development of the portal and hepatic veins. These are the sub-diaphragmatic (cranial part of the liver) and sub-hepatic anastomosis (caudal part of the liver) between the vitelline veins. The sub-diaphragmatic anastomosis contributes to formation of the LHV and common hepatic vein. Persistence of vene revehentes in the left part of the sub-diaphragmatic anastomosis could lead to formation of independent trunks of MHV and LHV.
In the present study, the length of common trunk from the inferior vena cava till the confluence of LHV and MHV was seen to fall between 4 to 18 mm, 9±3.3 mm. The diameter of common trunk in present study was comparable to that of others researchers [5,6,9,13,17,22] [Table/Fig-12]. There was a slight difference in the diameter of the common trunk in present study with that of earlier studies. It was found to lie between 10 to 22 mm (14.6±3.38 mm) in the present study which was not same as that of Nakamura S and Tsuzuki T (17±5 mm) [5].
Comparison of length of common trunk with other researchers [5,6,9,13,17,22].
| Studies done | Length |
|---|
| Present study | 4-18 mm (9±3.3 mm) |
| Ortale JR et al., [13] | 2.8-16 mm (7.1±2.8 mm) |
| Honda H et al., [6] | 7.1±2.8 mm |
| Nakamura S et al., [5] | 2-17 mm (10±5 mm) |
| Adson MA [22] | 2 cm |
| Baird RA et al., [17] | 0.2-2.2 cm (mean 1 cm) |
| Woodburne RT et al., [9] | 1 cm |
In the present study, four types were identified. Type I (10%) consisted of cases, in which the length of the common trunk more than 1 cm. In other words, these were the cases in which safe ligation of the vein could be considered. This finding was very close to that reported by Nakamura S and Tsuzuki T (10.8%) [5]. In rest of the cases, due to the short distance of the tributaries from the inferior vena cava and also due to short common trunk, the LHV is vulnerable to injury during the extended right lobectomy and the MHV during the left lobectomy.
Researchers in their study reported that selective clamping of the LHV was possible if the length of this vein was at least 6 mm long before entering the IVC. The selective clamping of this vein is difficult due to high frequency of common trunk shared with the MHV and of a short extra-parenchymatous segment [18].
Type IIa, (73.3%) of cases, corresponded to the Type IIa of earlier study (26.5%) which was a little lower than that as seen in present study [5]. The Type IIb was present in 6.66% of cases, which was almost double the number of cases as compared to the previous study, in which it was 1.2%. This type was referred to as Type IId, in Nakamura S and Tsuzuki T study [5].
Type IIc was seen in about 10% the cases. This type was different from IIc described by previous researcher. Despite, extensive research of literature, no reference of this type of variation was found anywhere. As this was a type found in the present study, it requires a special mention and was found in 10% of population studied. Care should be given to this type while doing left lobectomy. Type III, in present study was represented by 16.6% of the cases. This value was much higher than quoted in the earlier studies. In previous study, this type mentioned was quoted as a Type IIIb (9.96%) [5].
There was another type that was found in the present study, which was named as Type IIIb. It was present in 3.32% cases. This variation has not been mentioned in the literature. Prior knowledge of this variation could be of tremendous importance during left lobectomy. In another study done, separate insertion of LHV and MHV was reported in 26.5% of cases [6].
The medial intersegmental area was found to be drained by the left and the MHVs. This was important in left lobectomy as the drainage of this area can be hampered during the resection of the liver if only one single large vein is contributing in the drainage of this area. In majority of the cases, the LHV drained this intersegmental area. The next in frequency was that the drainage area was shared equally by LHV and the MHV. In 10% cases, MHV was predominant. These findings were similar to that of previous researcher [5].
However, some researchers found that the LHV drained this area in 58% cases, MHV in 25% cases. In 17% cases the drainage was shared by the LHV and MHV [23].
In another study done, in 10.7% the medial segmental area was drained by either the common trunk of LHV and MHV or by direct branches from the IVC. The LHV drained the area in 69.3% cases and MHV in 18.7 cases [20].
Limitation
Due to tough connective tissue of the dissected specimen, further deep dissection of the liver was difficult. We intend to use radiological parameters to present study in future. We intend to study about the angle formed by the the hepatic veins with common trunk and with the IVC in future studies.
Conclusion
There are wide variations in the drainage of the left lobe of liver. These variations affect the course of treatment in the left lobe of liver. The variant type of anatomy seen in the types IIc and IIIb have not been highlighted in previous studies. Careful study of drainage of liver by RAS vein is very important in Types IIc to avoid any unforeseen complication while performing lobectomy of the liver.
In cases like IIIc, where the main trunk of LHV was not seen, instead the left lateral, left medial and MHV formed confluence, the selective clamping of veins during left lobectomy might be tedious. So, a comprehensive study of the variant anatomy of the liver is mandatory before carrying out any procedure in the liver to prevent any unexpected complication.
LHV: Left Hepatic Vein; MHV: Middle Hepatic Vein