Thyroid nodules are a common clinical complication in the adult population globally, and the prevalence of thyroid cancer is up to 5–15% [1-3]. The condition is associated with high cost of diagnosis and treatment [4]. Several imaging modalities have been used in identifying and differentiating benign from malignant thyroid nodules with varying degrees of sensitivity and specificity. One of the non-invasive imaging modality has been high-frequency Ultrasound (US); although it offers excellent images of TNs, it has low sensitivity for Thyroid Cancer (TC), and provides inadequate evidence on the mechanical properties of benign and malignant TNs [5-8]. Further, its performance and accuracy depends on the operator’s experience [5].
Shear wave elastography is a non-invasive imaging modality that offers quantitative measurements of tissue elasticity properties [9]. It provides estimations of tissue shear wave velocity in meter/second (m/s), which is proportional to the characteristics of tissue stiffness. Previous studies have shown the reliability and accuracy of shear wave elastography in indentifying and distinguishing benign from malignant thyroid nodules [10,11]. Acoustic Radiation Force Impulse (ARFI) is a new modality that can evaluate thyroid tissue stiffness quantitatively [12]. There are two types of SW imaging under ARFI excitation: point SWS measurement (or point SWE) and SWS imaging {or two-dimensional (2D) SWE} [13-15]. During ARFI imaging, tissues within the region of interest (ROI) are automatically excited through using short-duration acoustic pulses to generate small (1–10 μm) localized tissue displacements, with the more elastic tissue undergoing more displacement, and vice versa [16,17].
A 2-D shear wave technology generated by means of ARFI known as VTIQ, a non-invasive SWE instrument for analysing TN elasticity, is capable of creating shear wave image, and provide subsequent tissue quantification in one show and allow for identification of place for tissue stiffness measurement (ROI-region of interest) [18]. The application of this technology in differentiating between benign and malignant TNs has been reported elsewhere [13,19].
However, some TNs might not show typical stiffness manifestations on 2D SWS imaging, which would lead to false-positive and false-negative results. The aim of this study was to evaluate the role of VTIQ in distinguishing between benign and malignant thyroid nodules for the diagnostic purposes.
Materials and Methods
This prospective study was conducted for eight months from February 2016 to October 2016 at the Faculty of Ultrasound Diagnosis of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, China. Permission to conduct this prospective study was sought and granted from the Research and Ethics Committee of the Tongji Medical College of Huazhong University of Science and Technology, Wuhan, China. The study was performed in accordance with the Declaration of Helsinki for human study.
Patients: A total of 54 patients who were planned for surgery with a total of 78 TNs were included in the study. The inclusion criteria were: (1) Patients who are 18 years of age or older and of different genders; (2) Patients with single or multiple solid TNs bigger than 0.5 cm in size and scheduled for surgical treatment; (3) Patients with thyroid nodules of ≥0.5 cm with at least two of the following characteristic features hypoechoic, microcalcifications, irregular outline, taller than wider, increased central vascularity, isoechogenecity, and heterogeneity patterns; and (4) No invasive thyroid surgery or FNAB were performed before. Exclusion criteria were: (1) Patients with fluid filled thyroid lesions; (2) Patients with thyroid nodules lesions of 0.5 cm regardless of their characteristic features. Prior to surgery, all eligible study participants were examined using B-mode traditional ultrasound, colour Doppler ultrasound, and shear wave elastography, and the results compared to histopathological findings of the resected thyroid gland tissue.
B-Mode and Doppler Ultrasonography: A B-mode characteristics scan probe of 18L6 High Definition (HD) to scan for TNs of included patients was used. The thyroid glands were evaluated for heterogeneity, and the TNs further evaluated for size, heterogeneity, presence of microcalcifications changes, echoic characteristics (iso-echoic and/or hypo-echoic), and length of the nodules and complexity of the TNs. Microcalcifications changes as tiny (≤1 mm) spot(s) of calcium in the TN without shadowing, and macrocalcifications as dense calcification(s) (>1 mm) that creates distal acoustic shadowing was defined. Based on their Doppler vascular styles, TNs were divided into 4 organizations: no blood flow, peripheral blood flow, peripheral and central blood flow (peripheral > central) and central blood flow (central > peripheral).
Shear Wave Elastography: Prior to undergoing SWE, all patients underwent traditional US examinations. SWE was performed using digital VTIQ Software database of Siemens ACUSON S3000 US system with a 9L4 Multi-D transducer (SIEMENS Medical Solution, Mountain View, GERMANY). Standard procedures were followed when performing SWE. The SWV map was acquired two times, and the Shear Wave Velocity size changes carried out subsequently. Tissue velocity was also measured with a small ROI field measuring 1.5 mm in diameter on the region of interest (ROI box size with VTIQ is programmed and cannot be changed). The Shear Wave Velocity of the stiffest area within was measured twice or more (velocity Reading 1 and 2), and the velocity of the thyroid tissue surrounding the nodule (tissue velocity) was measured once to assess the difference. The highest velocity of Reading 1 and Reading 2 within the thyroid nodule was reported as the maximum SWV. Mean Velocity was defined as the average of the two thyroid nodule velocity measurements. SWV was measured twice or more within the TN because the ROI box is relatively small (1.5 mm in diameter).
Histopathology Diagnosis The Histopathological examination served as the reference for the assessment of conventional B-mode, Doppler ultrasound and SWE imaging. After scanning and SWE, all seventy-eight thyroid nodules were examined histologically. Inmunohistochemical staining examination was also carried out.
Statistical Analysis
Statistical analysis was done using SPSS version 20.0 software. Statistical analyses were done by bivariate and multivariate methods. The ROC curve was used to compute for the diagnostic accuracy of SWE. Statistical significance was accepted at the 5% level (p<0.05).
Results
The median age of 54 patients who participated in this study was found to be 45.9±14.4 years (range, 21-79 years). Most of the TNs (N = 70, 89.74%) were observed in women compared to men (N=8, 10.26%). A total of 54 nodules (69.23%) were identified as TC and 24 nodules (30.77%) were found to be of benign origin. The mean age of patients with malignant thyroid nodules was lower (mean±SD; 42.93±12.88 yrs) than those with benign thyroid nodules (54.13±15.39 yrs; p-value <0.0001).
The bivariate analysis was performed to assess for the association between cancer and non-cancer condition with demographic and ultrasound variables (B-mode and Doppler) characteristics [Table/Fig-1]. The maximum SWV for the malignant TNs (6.50±1.13 m/s) was substantially higher than the upper-most SWV of the benign TNs (3.50±0.41 m/s; p < 0.0001). The B-mode ultrasound characteristics (hypoechoic thyroid nodules) were more frequently observed in the thyroid cancer patient’s category (53 TNs, 67.95%) than in those with benign thyroid nodules (4 TNs, 5.13%) (p<0.0001). Other B-mode ultrasound appearances are depicted in [Table/Fig-1].
Demographic variables and ultrasound features for identification of malignant TN.
| Variable | Benign N=24(%, Mean, SD) | Malignant N=54(%, Mean, SD) | p-value |
|---|
| Age (years) | 54.13±15.39 | 42.93±12.88 | <0.0001 |
| Sex |
| Female | 22(91.67%) | 48(88.89%) | <0.0001 |
| Male | 2(08.33%) | 6(11.11%) |
| Maximum SWV | 3.50±0.41 | 6.50±1.13 | < 0.0001 |
| Mean SWV | 2.55±0.41 | 3.49±1.09 | < 0.0001 |
| B-mode ultrasound characteristics |
| Hypoechoic | 4(05.13%) | 53(67.95%) | < 0.0001 |
| Spot Microcalcification | 5(06.41%) | 51(65.38%) | < 0.0001 |
| Irregular margin | 7(08.97%) | 52(66.67%) | < 0.0001 |
| Heterogeneity | 3(03.85%) | 5(06.41%) | 0.6550 |
| Central vascularity | 15(19.23%) | 53(67.95%) | < 0.0110 |
| Isoechogenic | 19(24.35%) | 1(01.28%) | < 0.0001 |
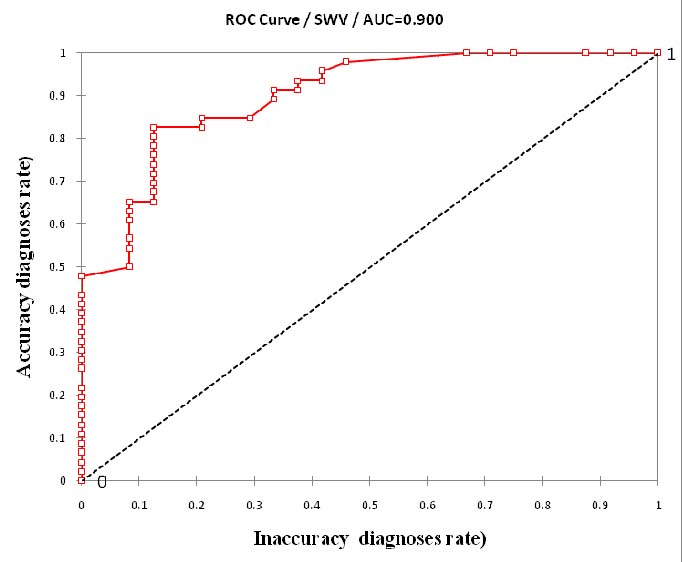
Diagnostic accuracy of Thyroid Cancer using the ROC curve for SWV: The ROC curve was used to determine the diagnostic accuracy of SWV in predicting TC [Table/Fig-2]. The Receiver Operating Characteristics Curve shows Area under the Curve of 0.90. Based on the ROC curve SWV for predicting most of the cancers, a single cut-off of 3.49 m/s has a diagnostic accuracy of 62.96%, positive and negative predictive values of 94.44% and 52.38% respectively.
Receiver operating characteristic curve using malignant nodule = 1.00 for the accurate diagnosis level.
Frequency of occurrence of TNs by SWV groups predicting diagnostic accuracy Thyroid Cancer: SWV was divided into five groups with 1.0 m/s being the reference interval between each group. The groups are Group 1(1.5-2.5 m/s), Group 2 (2.6-3.5 m/s), Group 3(3.6-4.5 m/s), Group 4(4.6-5.5 m/s) and group 5(5.6-6.5 m/s). The findings are summarized in [Table/Fig-3].
Prevalence of TNs by SWV groups predicting the diagnostic accuracy of thyroid cancer.
| Group | Group velocity(m/s) | Benign TNn(%) | Cancer TNn(%) | Totaln(%) |
|---|
| 1 | 1.5-2.5 | 3 (3.85) | 0 (0.00) | 3 (3.85) |
| 2 | 2.6-3.5 | 17 (21.79) | 4 (5.13) | 21 (26.92) |
| 3 | 3.6-4.5 | 4 (5.13) | 19 (24.36) | 23 (29.49) |
| 4 | 4.6-5.5 | 0 (0.00) | 15 (19.23) | 15 (19.23) |
| 5 | 5.6-6.5 | 0 (0.00) | 16 (20.51) | 16 (20.51) |
| Total | 24 (30.77) | 54 (69.23) | 78 (100.00) |
A multivariate regression model was applied to assess for predictors of thyroid cancer when using SWV. We combined the five SWV group categories and sub-groups to predict accuracy of malignancy for each of the specified SWV groups; sub-groups 1-3 (1.5-4.5 m/s), sub group 4-5 (4.6-6.5 m/s) and compared them with their respective nodules size. A multivariate regression model analysis predicted malignancy for each SWV sub-group and TNs size of shear wave ultrasound measurement with high accuracy and was dependent on the nodule size [Table/Fig-4]. Histological examination revealed 54 (69.23%) malignant nodules of which 51 nodules (94.44%) were papillary carcinomas, 2 (3.70%) follicular carcinomas, and 1(1.85%) was a lymphoma. Of the 24 (30.77%) benign nodules, 19 nodules (79.17) were hyperplastic, 2 (8.33%) follicular adenomas and 3 (12.50%) were Hashimoto thyroiditis.
Multivariate regression model, predicting the diagnostic accuracy of malignancy for each SWV sub-groups and TNs size.
| Size (cm) | Gro-up | Thyroid nodule status | p-value | Diagnostic accuracy, % | Diagnostic inaccuracy, % | PPV,% | NPV,% |
|---|
| Benign n=24 | Malignant n=54 |
|---|
| ≤1 | 1-3 | 8 | 17 | <.001 | 59.09 | 40.91 | 86.67 | 25.93 |
| 4-5 | 0 | 5 | <.001 | | | | |
| >1 | 1-3 | 13 | 20 | <.001 | 81.25 | 18.75 | 92.86 | 41.67 |
| 4-5 | 3 | 12 | <.001 | | | | |
| All | 1-3 | 21 | 43 | <.001 | 62.96 | 37.04 | 94.44 | 52.38 |
| 4-5 | 3 | 11 | <.001 | | | | |
Key: TNs = Thyroid nodules; SWV = Shear wave velocity, PPV = Positive predictive value, NPV = Negative predictive value
Discussion
The aim of this prospective study was to evaluate the use of VTIQ of SWE in differentiating between malignant thyroid nodules from benign nodules. Virtual Touch Imaging is capable of creating SWE and subsequent tissues quantification in one display and allow for identification of regions for assessment of tissue stiffness and thus distinguishing malignant from benign thyroid nodules.
In the present study, the maximum SWV for predicting malignant thyroid nodules was observed to be higher than in benign TNs. For a tumour size of >1 cm, our single cut-off SWV for predicting TC, based on the ROC curve, was found to be 3.49 m/s with a diagnostic accuracy of 81.25%; and predictive values for detecting malignant and benign lesions of 92.86% and 41.67%, respectively. Our multi-regression analysis when measuring the efficiency of SWE as compared to other B-mode and Doppler ultrasound characteristics before histopathology examination showed that the SWE characteristics were the strongest predictors of malignant, better than the other malignant characteristics such as hypoechogenicity, irregular margin, and spot microcalcifications. Short Wave Elastography may predict malignant potential of a thyroid nodule and assist in pre-operative thyroid nodule plans prior to surgery.
This high accuracy demonstrated by SWE technology in predicting thyroid malignancy from thyroid nodules is dependent on the size of the nodule that is nodules larger than 1 cm in diameters. On the contrary, in their study, Rago T et al., reported that the predictive values of ultrasound elastography measurement was independent of the TNs size with the sensitivity of 100% and specificity of 100% being observed in 9 TNs that has a diameter of t >0.8 cm [20].
Previous studies have evaluated the Q-elastography in the pre-surgical diagnosis of TNs with indeterminate cytology. Cantisani V et al., observed that the ultrasound elastography predicted malignancy with a sensitivity of 83% and specificity of 93% in nodules that had diameter of ≤1cm [21]. Another study of virtual touch tissue quantification of acoustic radiation force impulse found that the VTQ of ARFI in thyroid nodule ≤1 cm is not satisfactory [22]. Trimboli P et al., reported that a Real-Time Elastography (RTE) is a valuable tool for detecting malignant thyroid lesions with sensitivity similar to the traditional ultrasound and colour flow Doppler features [23]. By adding RTE evaluation, the sensitivity of ultrasound in detecting malignant TNs is markedly increased, and is more reliable in selecting thyroid nodules that do not need cytology. Furthermore, both technologies might be useful in predicting malignant TNs of different diameter.
This variation in the size of nodules diameter can possibly be accounted for in shear wave elastography’s technology. The Virtual Touch Quantification (VTQ) that was used with these past studies creates shear wave data without providing a stiffness map imaging of the TN so that the region of greatest interest can be designated for numerical assessment. The VTIQ, that had been used in our study is capable of creating shear wave image map and subsequent tissues quantification in one display and allows for detection of a region of measurement in the thyroid nodules [24]. Another study demonstrated that VTIQ could correctly predict malignant thyroid nodules of diameters of 1cm or more [25]. In the present study, results were congruent with the study done by Benson J et al., which showed that the diagnostic accuracy of VTIQ in predicting TC is dependent on the nodule size that has a diameter of more than 1cm [25].
We divided TNs into five different predetermined groups based on the SWE. The diagnostic rate for predicting malignant and benign thyroid nodules was 21.79% and 5.13%, respectively. These clinically predetermined groups correlated well with the ROC determined cut-off of 3.49 m/s. The ROC curve of SWV for predicting thyroid cancer with a single cut-off at 3.49 m/s has a diagnostic accuracy of 62.96%; and PPV and NPV of 94.44% and 52.38%, respectively for differences in thyroid nodules sizes.
Zhang YF et al., and Cantisani V et al., who on separate occasions evaluated the role of SWE in the differential diagnosis of benign and malignant thyroid nodules by using virtual touch tissues quantification of acoustic radiation force impulse showed that the cut-off for distinguishing malignant from benign TNs were 2.87 m/s and 2.05 m/s, respectively, which is comparatively lower than the value of 3.49 m/s reported in present study (SWV in the interval reference of 1.0 m/s) [19,21]. However, Azizi G et al., in their study found that the SWV has a single cut-off of 3.54 m/s in predicting malignant thyroid nodule and sensitivity and specificity of 79.27% and 71.52%, respectively [26]. They also reported the PPV and NPV of 26.75% and 96.34%, respectively. The reported cut-off value of SWV reported in their study is slightly higher than the value of 3.49 m/s that was obtained in this study.
These variations are likely to be due to the area of the thyroid nodules selected for SWV measurement. The elasticity of thyroid nodules is different from one area of the thyroid nodule to another. The maximum average SWV depends on the hardest areas assessed for measurement. This variation could also be due to the sample selection in which, the more serious the case involved in the study, the higher velocity and subsequently the higher the single cut-off of ROC curve.
Limitation
The low number of subjects evaluated was one of the limitations of the study. Large prospective study with a larger sample is required to confirm the findings. Future studies focusing on the role of shear wave elastography in thyroid cancer progressive disease should be considered.
Conclusion
The results of this study indicated that that VTIQ, a non-invasive form of SWE was important in the diagnosis and differentiation of malignant and benign thyroid nodules of diameter greater than 1 cm.
Key: TNs = Thyroid nodules; SWV = Shear wave velocity, PPV = Positive predictive value, NPV = Negative predictive value