Prosthetic rehabilitation of hemimandibulectomy patient, with an overlay denture, restores missing skeletal, dental structures, muscle imbalance, maxillomandibular relationship and occlusion. Conventional management with an acrylic ramp or guide plane guides only the non-resected side of the mandible to occlusion. This case report describes rehabilitation of a 13-year-old hemimandibulectomy patient with tooth supported transitional overlay denture.
Ameloblastoma, Guiding flange, Hemimandibulectomy, Overlay Prosthesis, Occlusal Rehabilitation, Transitional prosthesis
Case Report
A 13-year-old boy reported to department of prosthodontics, Meenakshiammal Dental College and Hospital, complaining of difficulty in chewing and speech. Patient had undergone hemimandibulectomy, 2 years back, due to ameloblastoma, involving the right side of the mandible. He was wearing Palatal guiding flange prosthesis [1].
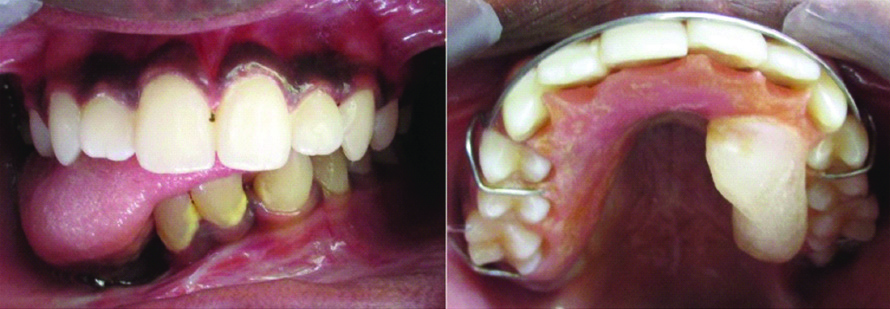
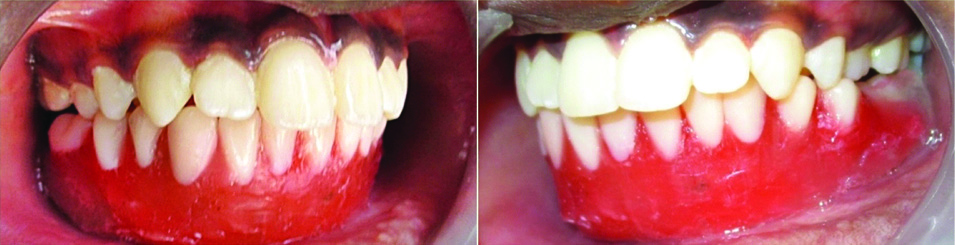
Clinical examination revealed no skeletal and dental component in the right segment of the mandible (fourth Quadrant) from midline, falling under Cantor and Curtis III classification [1,2]. Right lingual sulcus was completely obliterated. Left mandibular skeletal and dental component was deviated extensively towards the right side, without any occlusion. The guiding flange directed the left side of the mandible to a partial occlusion, between the upper and lower, first and second molars [Table/Fig-1]. The prosthesis also interfered with tongue movements, leading to slurred speech. The patient was not comfortable with the extensive palatal coverage of the prosthesis.
Preoperative occlusion with existing palatal guiding flange prosthesis.
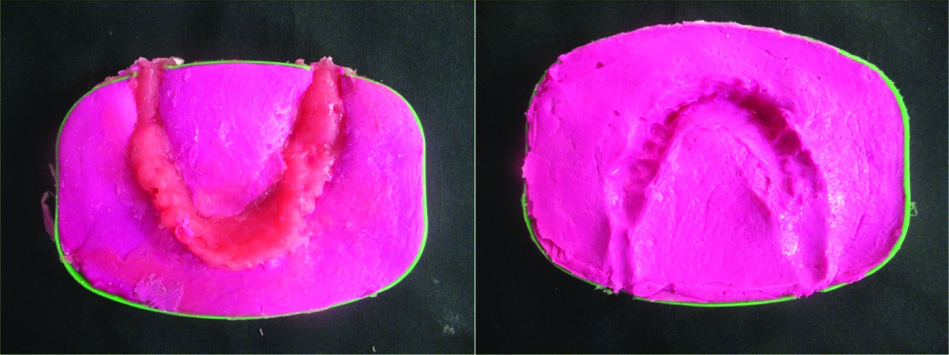
Preliminary alginate impressions were made and study casts were mounted on a mean value articulator with the aid of mush bite [3], a non-precision jaw record done using modelling wax [Table/Fig-2]. This bite records static comfortable position of the remaining mandible, since recording centric is not possible. A diagnostic wax mockup [4] was done, establishing the entire occlusion as well as the lost hard and soft tissues, which was processed to form an Acrylic template by a modified lost wax technique [Table/Fig-3]. A two component plastic box was used in the modified lost wax technique, by which an imprint of the wax mock up was made with alginate [Table/Fig-4]. An inlet and outlet channel was created to the mould space in the box, into which auto polymerised acrylic was injected, allowed to set, and removed [Table/Fig-5].

Diagnostic wax-up in occlusion.
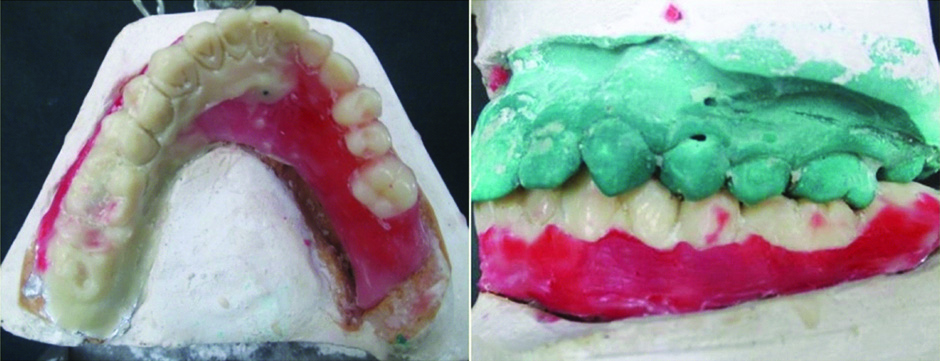
Lost wax technique customised with plastic box and alginate.
Autopolymerised acrylic template.
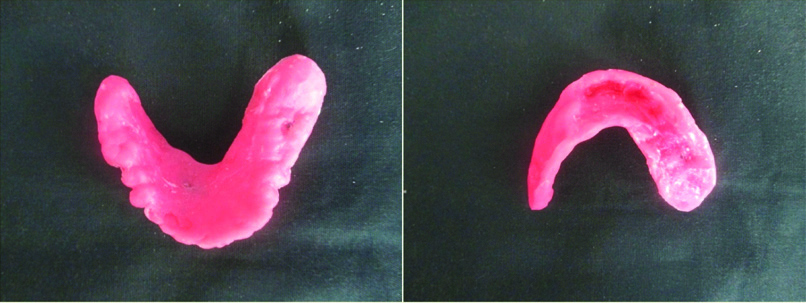
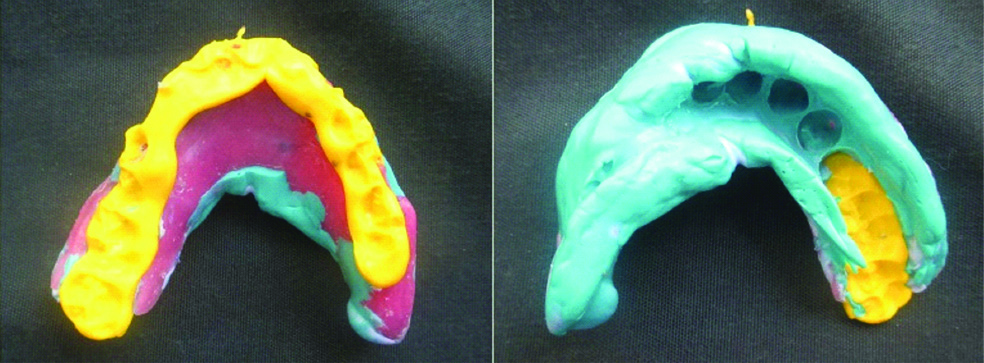
The template was adjusted to fit over the remaining existing teeth, extending over the edentulous region. A trial was done to check the facial profile and occlusion. Closed mouth impression [5,6] was made with the template using polyvinyl siloxane impression material (Aquasil - Dentsply). Bite registration was done using bite registration paste (Jet bite - Coltene), with the template [Table/Fig-6]. Master cast was poured with die stone (Type IV - Kalabhai).
Final impression and bite registration.
Face bow transfer was made and cast mounted in Hanau wide vue articulator [Table/Fig-7]. Teeth setting were done establishing occlusion. The patient was able to guide the trial denture into maximum intercuspal position [Table/Fig-8]. Denture processed using injection moulding technique and inserted [Table/Fig-9] [7].
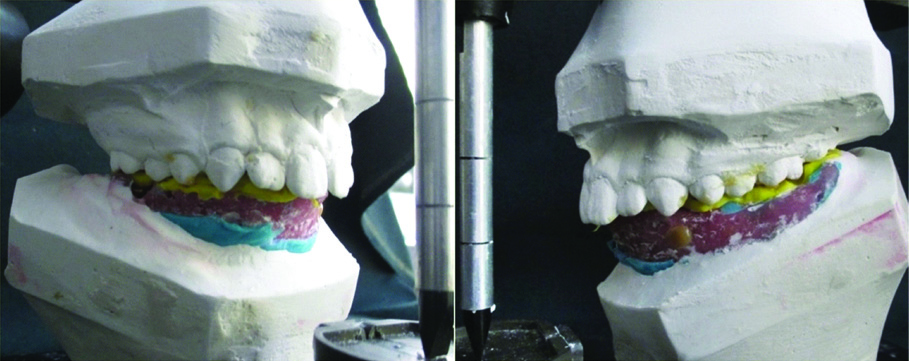
Established complete occlusion with trial denture.
a) Overlay denture, occlusal surface and intaglio surface simulating the dentulous anatomy for friction fit; b) Precise fit of the overlay denture establishing complete occlusion with maxillary teeth.

Follow-up was done for one year, once in every two months. The denture was adjusted to fit comfortably in every visit. After one year it was decided to re-do the denture, due to changes in intraoral morphology in accordance with the growth curve.
Discussion
Resection of the mandible following odontogenic tumours deviate the mandible towards the resected side during function, leading to loss of occlusion, facial asymmetry, impaired masticatory efficiency, speech impairment, resulting in psychological trauma and difficult social life [8].
Guiding flange prosthesis redirects the existing teeth into occlusion, but a segmental occlusion is insufficient and there is a need to restore complete occlusion for effective restoration of function, aesthetics and phonetics. For a 13-year-old patient, the prosthesis should be transitional, considering the growth phase.
The partial occlusal contact, existing between the left maxillary and mandibular molars, were used as reference, recorded by the Mush bite and transferred to the articulator. This position was considered the most comfortable with existing maxillomandibular relationship. The entire occlusal pattern, desired for final restoration, was created using Sculpting wax (Delta) [4]. Occlusion created on the articulator has to be checked intraorally, which necessitated the need for a template, duplicating the created occlusion, more firm and steady to withstand the intraoral forces. The wax pattern was processed to autopolymerised acrylic template, using modified lost wax technique.
The purpose of the autopolymerised acrylic template was:
To evaluate the accuracy of the planned occlusal pattern.
To evaluate sufficient vertical dimension.
To act as a special tray, for the final impression.
To evaluate aesthetics, face-form and contour of the final restoration.
For this patient, the maxillomandibular relationship, derived from the template, coincides with the Maximum Intercuspation (MI) of the planned prosthesis. Following facebow transfer and articulation in semi-adjustable articulator, the trial denture made, delivered a more accurate MI intraorally. For more precision, injection moulding technique was used for processing the denture. Inclusion of metal components could have strengthened the denture base, and reduced its flexure, but to reduce the stress accumulation over the remaining mandible, it was not considered. The patient was trained to guide the prosthesis to occlusion, during functional movements.
Tooth supported overlay dentures can be transitional and cost effective without any metallic components. The friction fit of the denture, provided excellent retention and stability, as well as improved dental and facial aesthetics. There was re-establishment of occlusal contacts, which provided better proprioception, better clinical conditions of masticatory muscles, co-ordinated mandibular movements with a good masticatory efficiency [9].
However, the disadvantages of the overdenture is its bulkiness, interference with tongue movements, can trigger caries or periodontal problems of the underlying teeth. The patient has to be trained in effective oral hygiene maintenance and speech.
Considering the age of the patient, it is recommended to periodically review and replace the prosthesis, in accordance with the growth phase. After a year there was difficulty in wearing the denture, it was suggested to be re-done, establishing the required aesthetic and functional parameters. During the first year, patient was very comfortable, with a good masticatory efficiency, facial aesthetics and a good self-esteem.
Conclusion
Success factors in rehabilitation of hemimandibulectomy patients with mandibular overdenture include restoration of occlusion, which restores mastication, phonetics, facial aesthetics and symmetry. Although transitional, it restored a healthy psychology and confidence for the patient.
[1]. Gopi A, Singla NK, Saini DK, Legha VS, Guide the Mandible back home: Guide flange prosthesisJ Orofac Res 2013 3(4):290-93.10.5005/jp-journals-10026-1115 [Google Scholar] [CrossRef]
[2]. Cantor R, Curtis TA, Prosthetic management of edentulous mandibulectomy patients. Part I. Anatomic, physiologic, and psychologic considerationsJ Prosthet Dent 1971 25:446-57.10.1016/0022-3913(71)90236-8 [Google Scholar] [CrossRef]
[3]. Bansal S, Palaskar J, Critical evaluation of various methods of recording centric relationJ Indian Prosthodont Soc 2008 8(4):185-91.10.4103/0972-4052.49180 [Google Scholar] [CrossRef]
[4]. Gauri M, Ramandeep D, Waxing techniques to develop proper occlusal morphology in different occlusal schemesJ Indian Prosthodont Soc 2011 11(4):205-09.10.1007/s13191-011-0090-923204728 [Google Scholar] [CrossRef] [PubMed]
[5]. Sahukar SK, Closed mouth impression techniqueJ Indian Dent Assoc 1967 39(8):113-16. [Google Scholar]
[6]. Heymer ME, A new practical procedure for the preparation of complete dentures with closed mouth impression, function impression and bite registrationDeutesche zahnarztliche Zeitschrift 1970 25(2):242-46. [Google Scholar]
[7]. Gharechahi J, Asadzadeh N, Shahabian F, Gharechahi M, Dimensional changes of acrylic resin denture bases: conventional versus injection-molding techniqueJ Dent (Tehran) 2014 11(4):398-405. [Google Scholar]
[8]. Beumer J, Marunick MT, Silverman S, Garrett N, Rieger J, Abemayor E, Rehabilitation of tongue and mandibular defects. In: Beumer J, Marunick MT, Esposito SJ, editorsMaxillofacial Rehabilitation: Prosthodontic and surgical management of cancer related, Acquired, and congenital defects of the head and neck 2011 3rd edChicagoQuintessence Publications Co:61-154. [Google Scholar]
[9]. Aruna U, Thulasingam C, Prosthodontic management of segmental mandibulectomy patient with guiding flange appliance and overlay dentureJ Indian Prosthodont Soc 2013 13(4):593-99.10.1007/s13191-012-0208-824431797 [Google Scholar] [CrossRef] [PubMed]