Osseous Metaplasia in Oesophageal Leiomyoma-A Rare Case Report
K Mamatha1, BR Yelikar2, Deepthi Chandrika Chintalapudi3, Anil Reddy Konduru4
1 Assistant Professor, Department of Pathology, Shri B M Patil Medical College and Hospital, Vijayapura, Karnataka, India.
2 Head, Department of Pathology, Shri B M Patil Medical College and Hospital, Vijayapura, Karnataka, India.
3 Postgraduate Student, Department of Pathology, Shri B M Patil Medical College and Hospital, Vijayapura, Karnataka, India.
4 Postgraduate Student, Department of Pathology, Shri B M Patil Medical College and Hospital, Vijayapura, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. BR Yelikar, Head, Department of Pathology, Shri B M Patil Medical College and Hospital, BLDE University, Vijayapura-586103, Karnataka, India.
E-mail: balasaheb.yelikar@bldeuniversity.ac.in
Amongst benign mesenchymal tumours of the oesophagus, leiomyomas are the commonest. Leiomyomas account for about two-thirds of all benign lesions of oesophagus. Oesophageal leiomyoma of more than 5 cm in diameter is a rare condition. In symptomatic patients surgical resection is recommended and in asymptomatic patients with small lesions observation is the policy. Extensive calcification or ossification within leiomyoma of oesophagus is an extremely rare finding. As per our knowledge there is no report of osseous metaplasia in oesophageal leiomyoma in literature so far. The present case is of a large oesophageal leiomyoma with osseous metaplasia diagnosed on histopathology.
Benign spindle cell neoplasm, Dysphagia, Upper gastro intestinal tract
Case Report
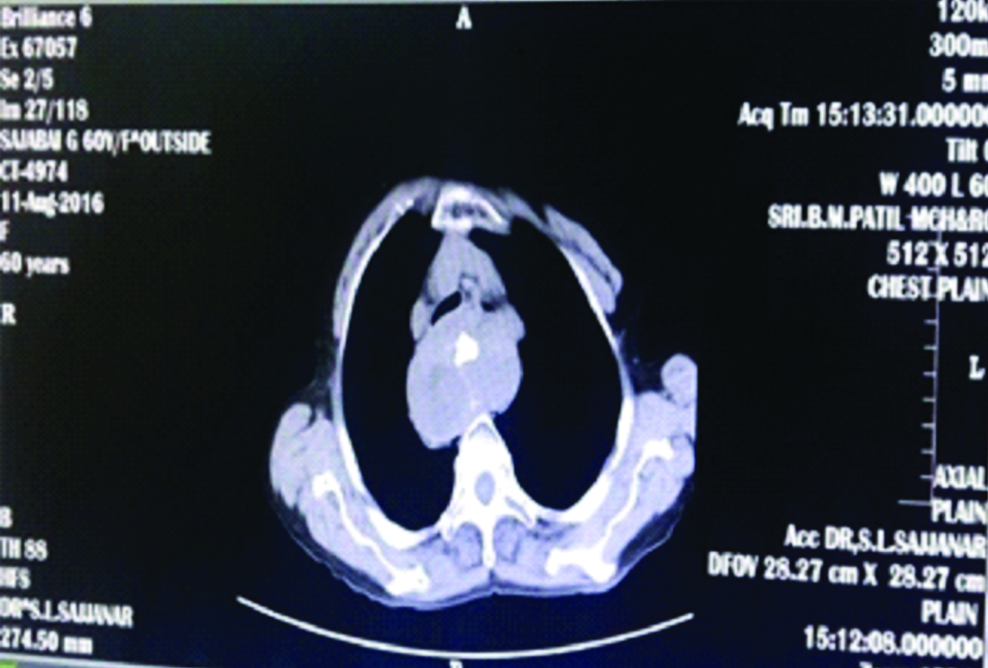
A 60-year-old female presented with complaints of dysphagia to solid food, cough and breathlessness for the past three months. Computed tomography evaluation showed a mass measuring 6×5×3.5 cm in upper oesophagus with features suggestive of small soft tissue density lesion with area of coarse calcification in the centre of the lesion with no obvious invasion. Radiologically, it was reported as benign lesion of oesophagus that could possibly be a leiomyoma and other differential diagnosis like oesophageal gastrointestinal tumour, oesophageal carcinoma, oesophageal leiomyosarcoma and hamartoma could be considered [Table/Fig-1].
CT scan-Soft tissue density lesion with coarse calcification in the center of the lesion.
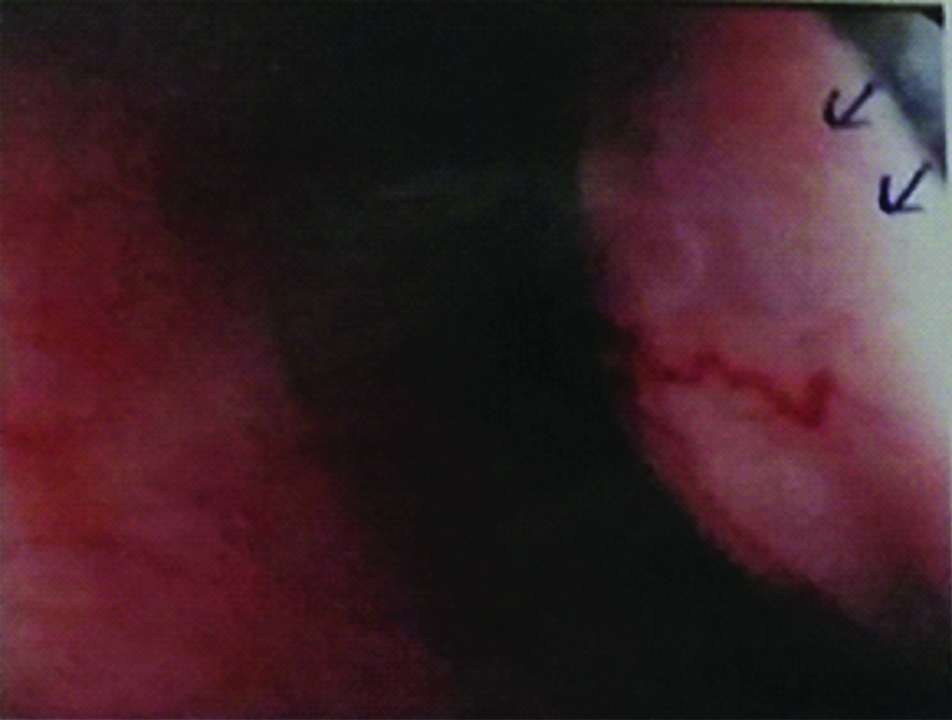
Upper gastro intestinal endoscopy was performed wherein cervical part of the oesophagus showed a large smooth bulge compressing the upper part [Table/Fig-2]. Patient underwent surgery and the resected specimen was sent for histopathological examination.
Endoscopy-large smooth bulge compressing the upper part of oesophagus.
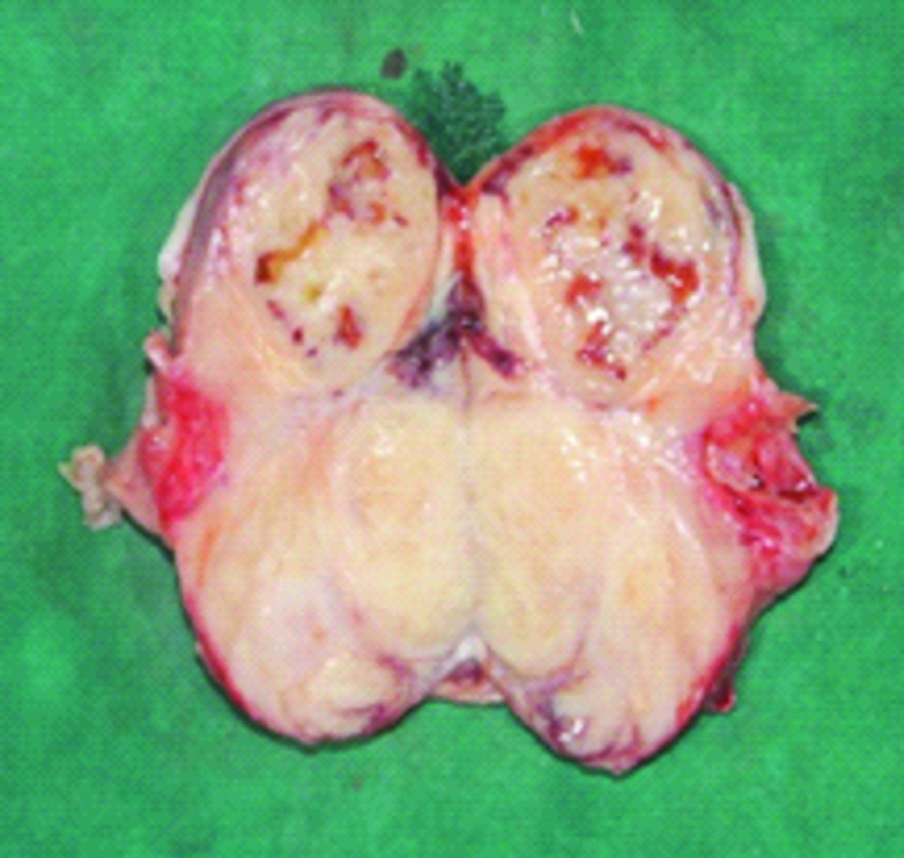
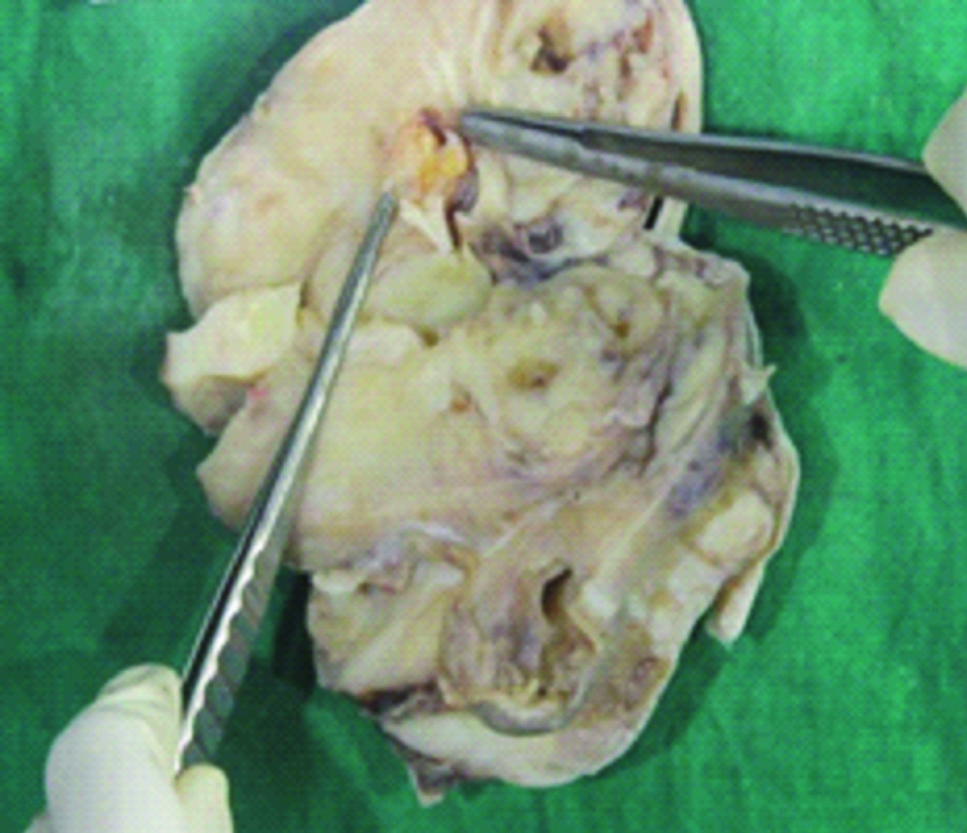
Grossly we received a pale pink capsulated globular tissue mass measuring 8×6×2.5 cm [Table/Fig-3]. Cut surface was lobulated with whorled appearance and consistency of the mass was firm [Table/Fig-4]. Also, noted a cystic area measuring 1×1 cm. An irregular bony fragment measuring 1×0.9 cm which was hard and gritty in consistency noted within the mass [Table/Fig-5].
Globular tissue mass measuring 8×6×2.5 cm.

Well circumscribed lobular, whorled appearance noted, with cystic areas.
Hard bony area measuring 1×1 cm.
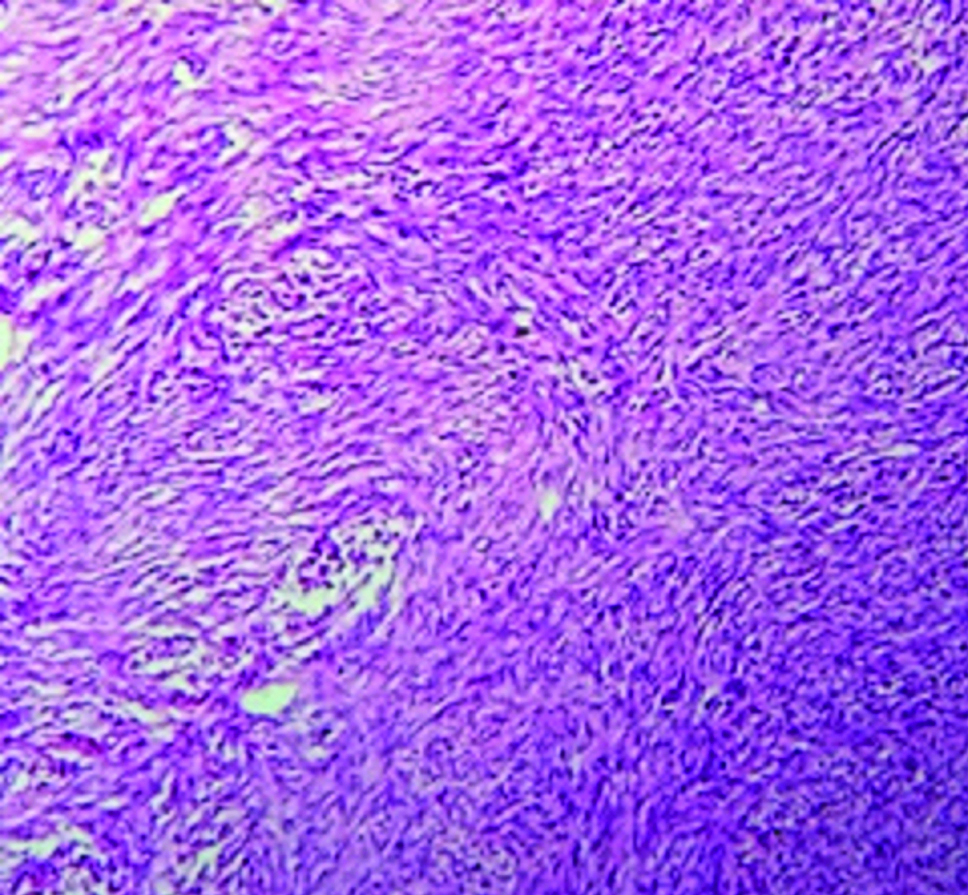
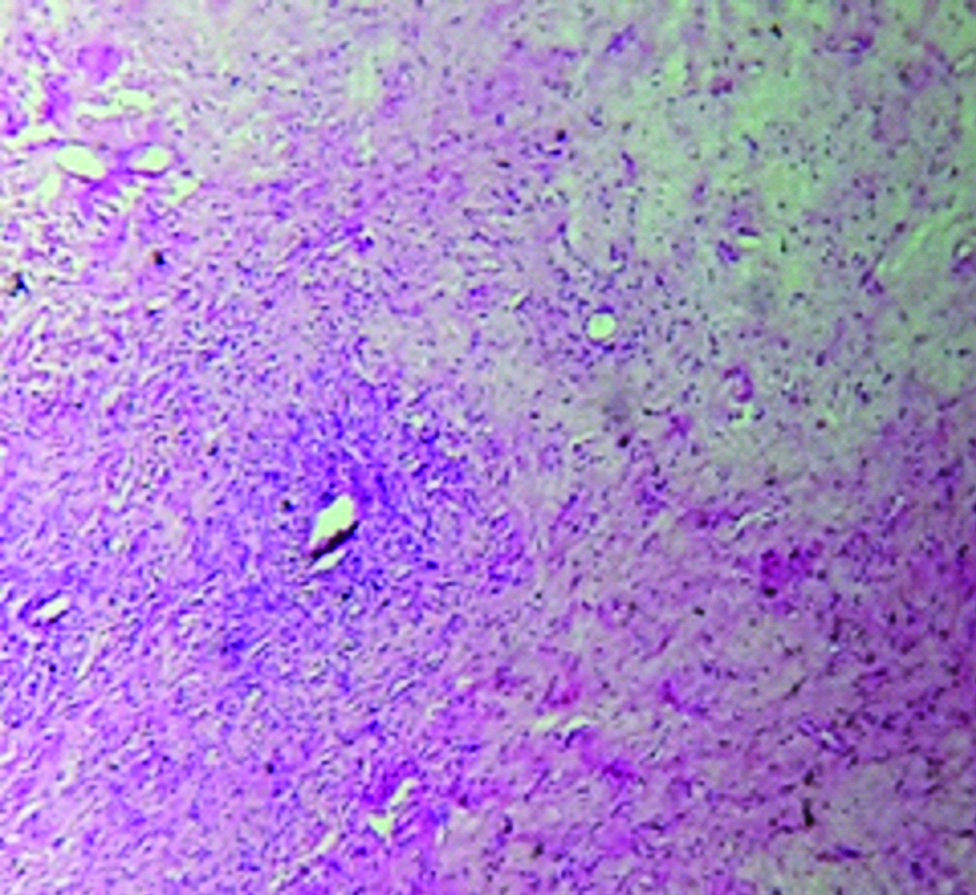
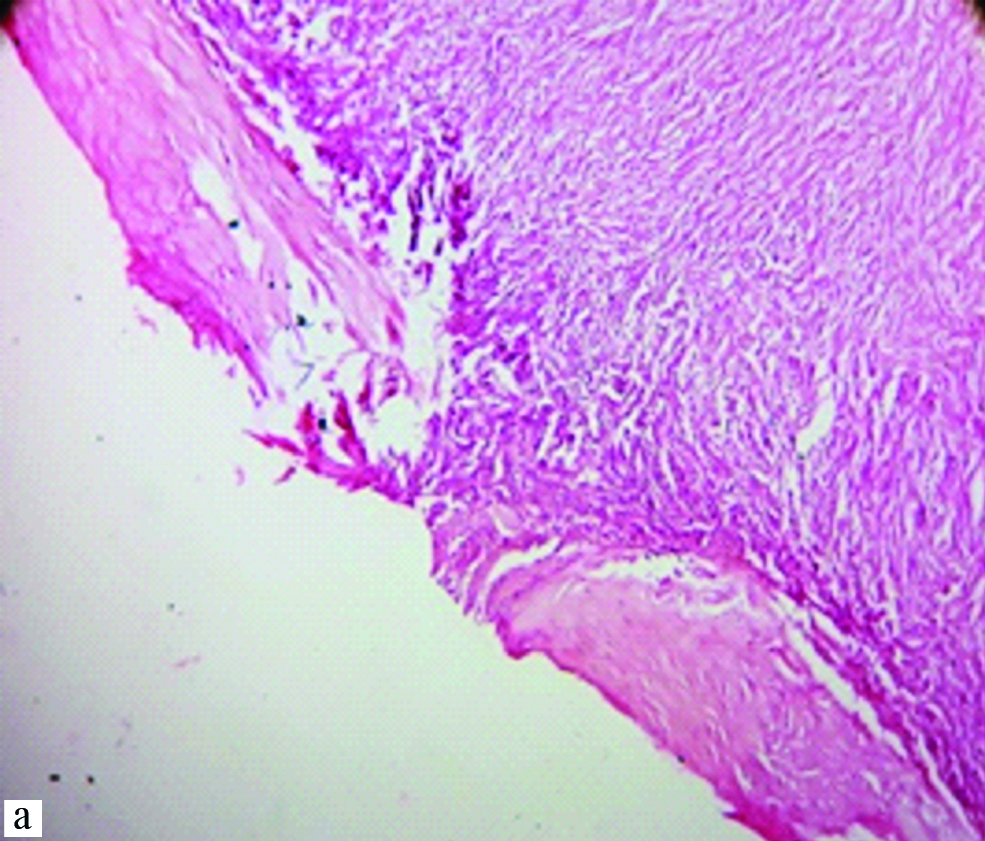
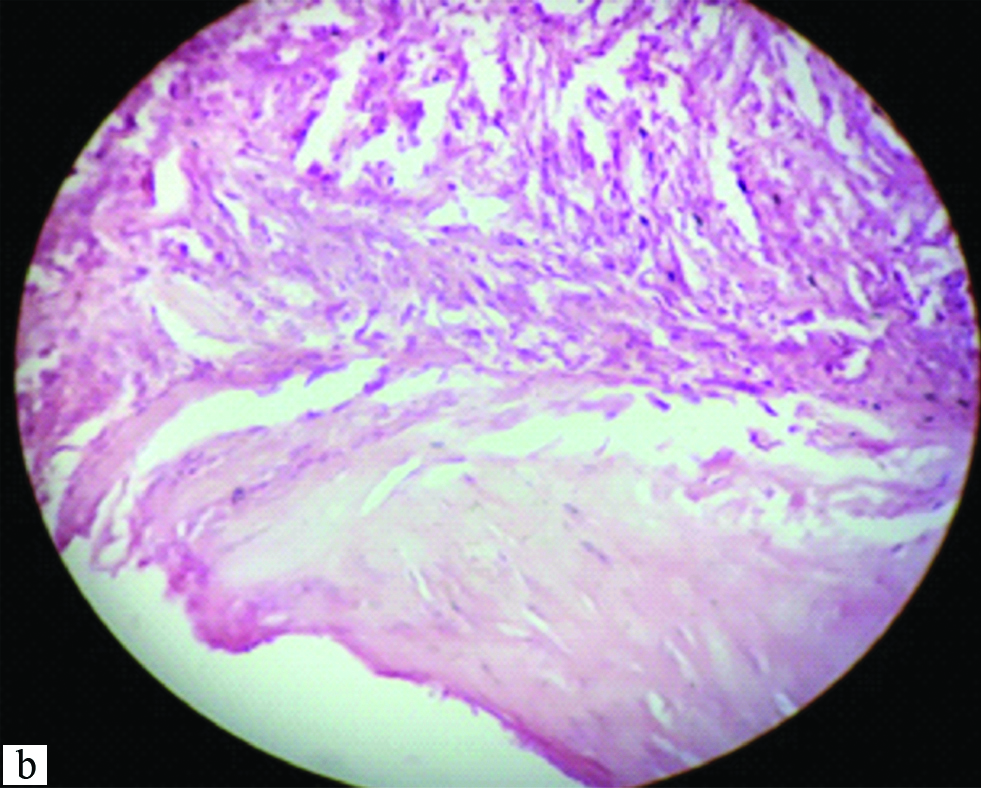
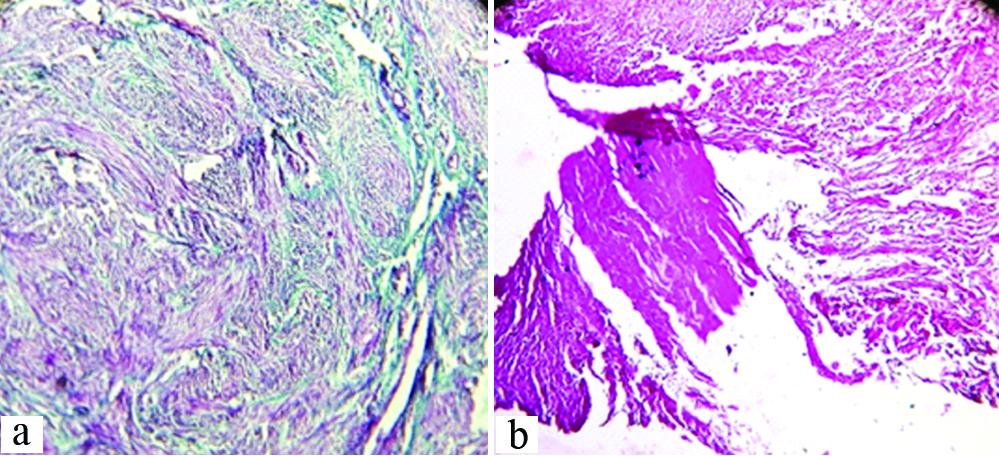
Globular mass showed capsulated tumour tissue comprised of spindle shaped cells arranged in interlacing sheets, bundles and whorled pattern. Individual tumour cells showed elongated nuclei with blunt ends. Intermingled collagenous bundles, extensive areas of hyalinisation and focal matured bony trabeculae surrounded by tumour tissue were noted [Table/Fig-6,7 and 8a,b]. Massons Trichrome stain showed, smooth muscle fibres stained with red, collagen stained with green and nuclei stained with black colour. Bony area stained eosinophilic which ruled out collagenisation [Table/Fig-9a,b].
Microphotograph showing spindle shaped cells in interlacing sheets, bundles and whorled pattern having elongated nucleus with both the ends blunted (H&E, 10X).
Microphotograph showing intermingled collagenous bundles and extensive areas of hyalinization (H&E, 10X).
Microphotograph showing focal matured bony trabeculae surrounded by tumour tissue. In lower magnification (H&E 10X).
Microphotograph showing focal matured bony trabeculae surrounded by tumour tissue. In higher magnification (H&E, 40X)
Microphotographs showing Massonstri chrome stain: Smooth muscle fibres-red, Collagen-green and Bony area-eosinophilic (10X).
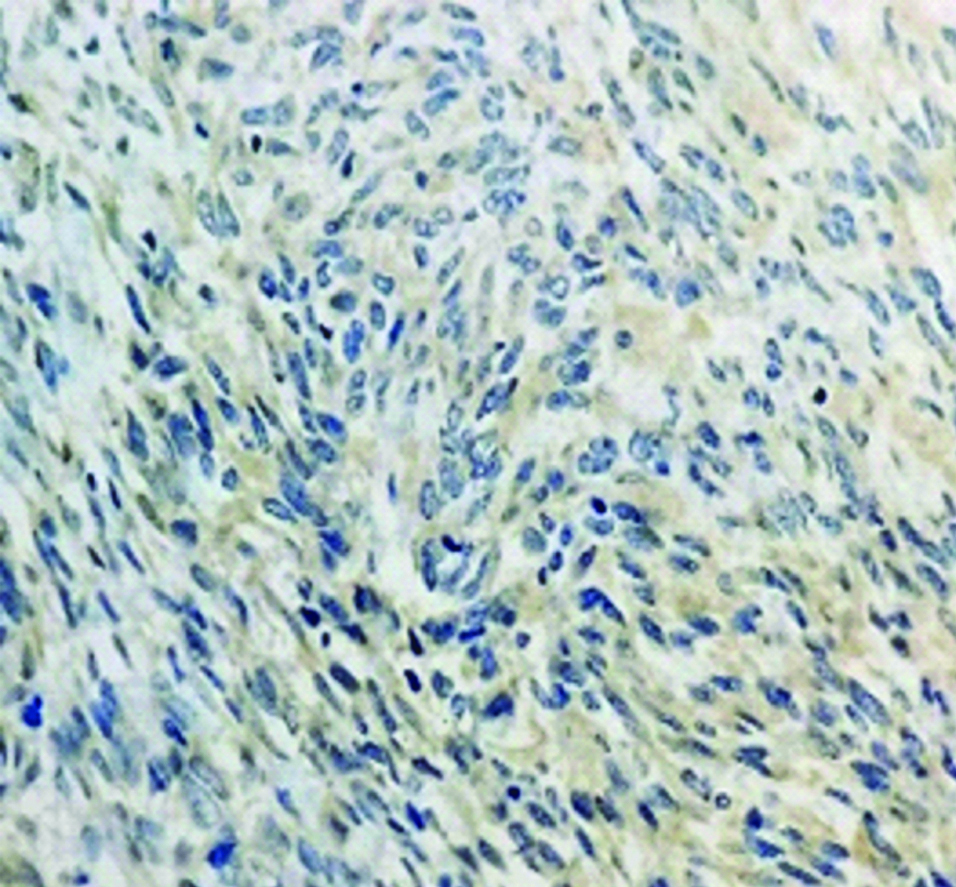
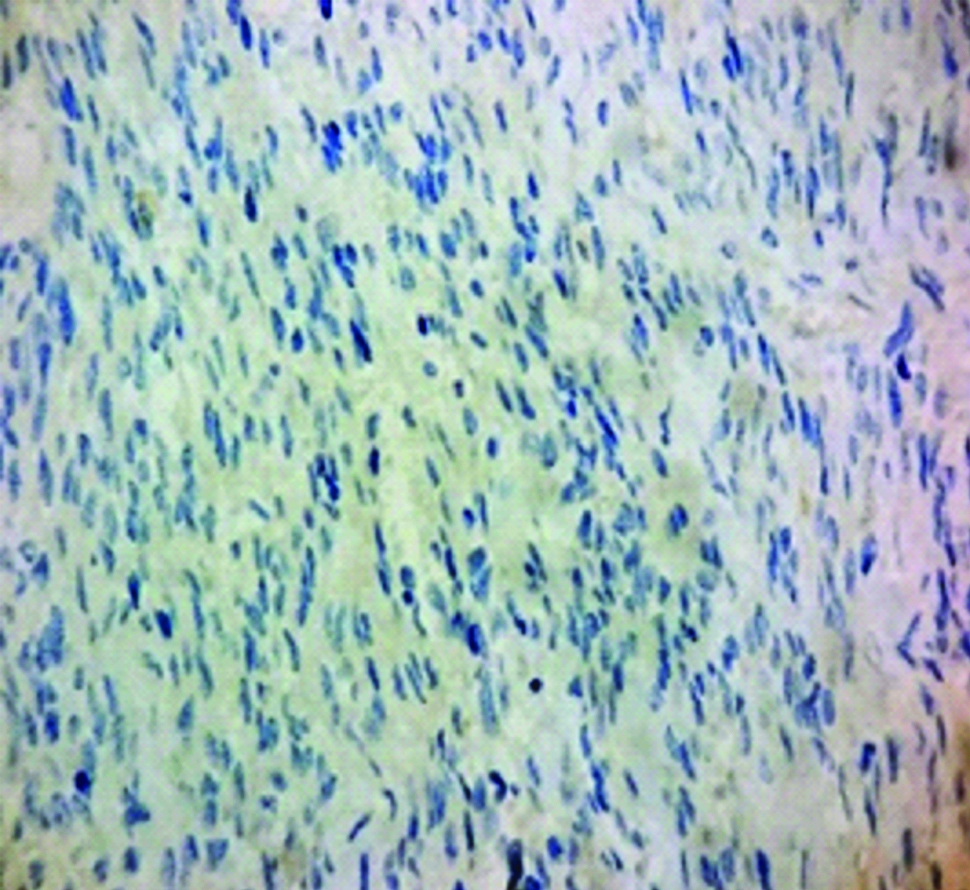
Based on these features a differential diagnosis of leiomyoma and Gastro intestinal stromal tumour was considered. Immunohistochemistry study was negative for DOG 1 and CD117 [Table/Fig-10,11]. Accordingly, final diagnosis of leiomyoma with osseous metaplasia was rendered.
IHC-DOG 1 negative (40X).
IHC-CD117 negative (40X).
Discussion
Leiomyoma is a benign neoplasm of smooth muscle. These tumours occur anywhere in the body where smooth muscle is present. The most common sites are genitourinary tract, gastrointestinal tract and skin [1,2].
Benign tumours in oesophagus constitute to about 1% of all the tumours in oesophagus. Leiomyoma is the most common benign tumour of oesophagus with a 2:1 male predominance [3,4].
Most common presenting symptoms are difficulty in swallowing and retrosternal burning sensation. Dysphagia becomes more apparent when the tumour diameter crosses 4.5-5 cm [5,6]. The autopsy series incidence of oesophageal leiomyoma is reported as one in 1119.4 autopsies as per Seremetis M et al., [5].
Oesophageal leiomyomas are commonly located in the lower third accounting for 56%, followed by the middle third constituting to 33% and very rarely in the upper third (11%) of oesophagus. This is in line with the distribution of smooth muscle in the oesophgus as mentioned by Seremetis M et al., in their analysis of 838 cases of leiomyomata of oesophagus – a worldwide literature reviews till the end of 1971 [4,5]. The present case falls in the rarest form of leiomyoma, location wise and even sex wise incidence.
The osseous metaplasia of leiomyoma is very rare and is commonly seen in the uterine leiomyoma. But the occurrence of osseous metaplasia in the oseophageal leiomyoma is extremely rare [5].
Infection, necrosis, hyaline degeneration, calcification, myxoid degeneration is the most common secondary degenerative changes seen in cases of leiomyoma. Calcified and ossified leiomyoma are uncommon but have been reported in the genitourinary tract, soft tissues of the extremities, skin and head and neck [1].
Muscle fibres are replaced by collagen, hyaline material, calcium and mucopolysacharide either solitarily or as a combination resulting in the form of reduced blood supply which leads to the secondary changes [1].
Metaplasia occurs due to factors like chronic inflammation, irritation or noxious stimuli [2]. Lipomatous metaplasia is well documented in the literature pertaining to leiomyoma in general [1]. Cartilagenous and osseous metaplasia in leiomyoma in extrauterine sites like oral, endometrial and uterine sites are rarely reported [2]. Microscopically, calcification in leiomyoma is a very rare finding where in the largest series as part of a review of world literature mentions calcification in six cases out of 838 [5]. Ossification can be due to mesenchymal cells undergoing metaplasia or it can be due to degenerative change [1].
Conclusion
Ossification in leiomyoma of oesophagus is extremely rare entity reported in the literature. Awareness of this entity in the oesophagus is important as variety of lesions can mimic like ossified leiomyoma both clinically and radiologically.
[1]. Montague LJ, Fitzpatrick SG, Islam NM, Cohen DM, Bhattacharyya I, Extensively ossifying oral leiomyoma: A rare histologic findingHead and Neck Pathol 2014 8(3):311-16.10.1007/s12105-013-0497-124142598 [Google Scholar] [CrossRef] [PubMed]
[2]. Chander B, Shekhar S, Osseous metaplasia in leiomyoma: A first in a uterine leiomyomaJ Can Res Ther 2015 11:66110.4103/0973-1482.13810426458678 [Google Scholar] [CrossRef] [PubMed]
[3]. Punpale A, Rangole A, Bhambhani N, Karimundackal G, Desai N, de Souza A, Leiomyoma of oesophagusAnn Thorac Cardiovasc Surg 2007 13(2):78-81. [Google Scholar]
[4]. Sun X, Wang J, Yang G, Surgical treatment of oesophageal leiomyoma larger than 5 cm in diameter: A case report and review of the literatureJ Thorac Dis 2012 4(3):323-26.10.1097/JTO.0b013e3182381515PMC3378205 [Google Scholar] [CrossRef] [PubMed]
[5]. Seremetis M, Lyons W, Deguzman V, Peabody J, Leiomyomata of the esophagus. An analysis of 838 casesCancer 1976 38(5):2166-77.10.1002/1097-0142(197611)38:5<2166::AID-CNCR2820380547>3.0.CO;2-B [Google Scholar] [CrossRef]
[6]. Mutrie C, Donahue D, Wain J, Wright C, Gaissert H, Grillo H, Esophageal leiomyoma: a 40-year experienceThe Annals of Thoracic Surgery 2005 79(4):1122-25.10.1016/j.athoracsur.2004.08.02915797036 [Google Scholar] [CrossRef] [PubMed]