Miniscrews are devices used for skeletal anchorage in Orthodontics and they are known for not depending on patients to collaborate fully with the treatment [1-3]. It is recommended for all ages, including patients in the growth phase [1,4], with varied installation sites depending on the direction resulting from movement. The hard palate (midpalatal suture or paramedian region), the alveolar process (maxillary and mandibular), the retromolar area, the maxillary tuberosity, and the lower portion of the zygomatic arch are usually the sites of choice [2-8]. The anatomy of soft tissue, tooth, bone, interradicular distance, morphology of the maxillary sinus, nerve locations, buccolingual bone depth, and lingual and buccal cortical thickness are the main factors considered for choosing the insertion site of miniscrews [2,9].
Miniscrews in the palate are installed both in midpalatal suture and paramedian region [6]; they are easy to install and efficient auxiliaries when absolute anchorage is required [10,11]. Moreover, this site is a safe alternative to replace insertion in the alveolar process for it has a keratinised tissue that makes the location less susceptible to infection and inflammation [5]. The two major considerations for palatal anchorage with miniscrews are bone quantity (measured as height) and bone quality of this anchorage site [10].
Materials and Methods
This pilot cross-sectional study was performed between April/2011 and September/2013 at the Orthodontic Clinic of the Postgraduate Studies of FUNORTE (Florianópolis, SC, Brazil) and approved by the Research Ethics Committee under protocol 173/11, which complied with the Declaration of Helsinki. The Informed Consent Form was not applicable because this is a retrospective study on secondary data.
The inclusion criteria of this study were cone-beam computed tomographies of young individuals of both genders, aged 9 to 15 years, with mixed or permanent dentition, seeking orthodontic treatment. Excluded from the study were individuals who had already been subjected to previous orthodontic/orthopaedic treatment, and presented syndromes, severe skeletal abnormalities, and lip and/or palate fissures. Additionally, patients with absence of teeth (except for third molars), impacted teeth in the maxilla, and severe dental crowding (assessed by the quantitative method of the Little index) [14] were also excluded, which resulted in a sample of 16 patients (5 males and 11 females with mean age 12.3 years).
All cone beam computed tomographies (ICat VisionTM, Imaging Sciences International, Penn Road, Hatfield, PA, USA) were performed by the same operator, who was previously trained. Tomographies were standardised with 120 kVP, 37 mAs, image acquisition time of 14.7 seconds for 0.2 voxel, and power of 12 Vdc 20 mA 220V~5A.
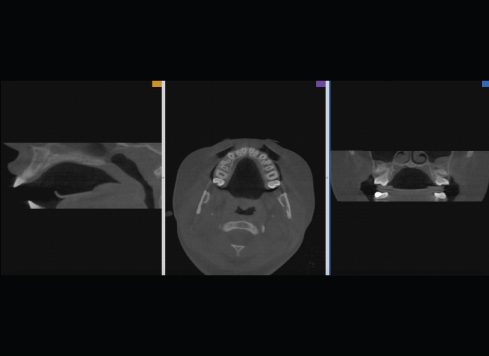
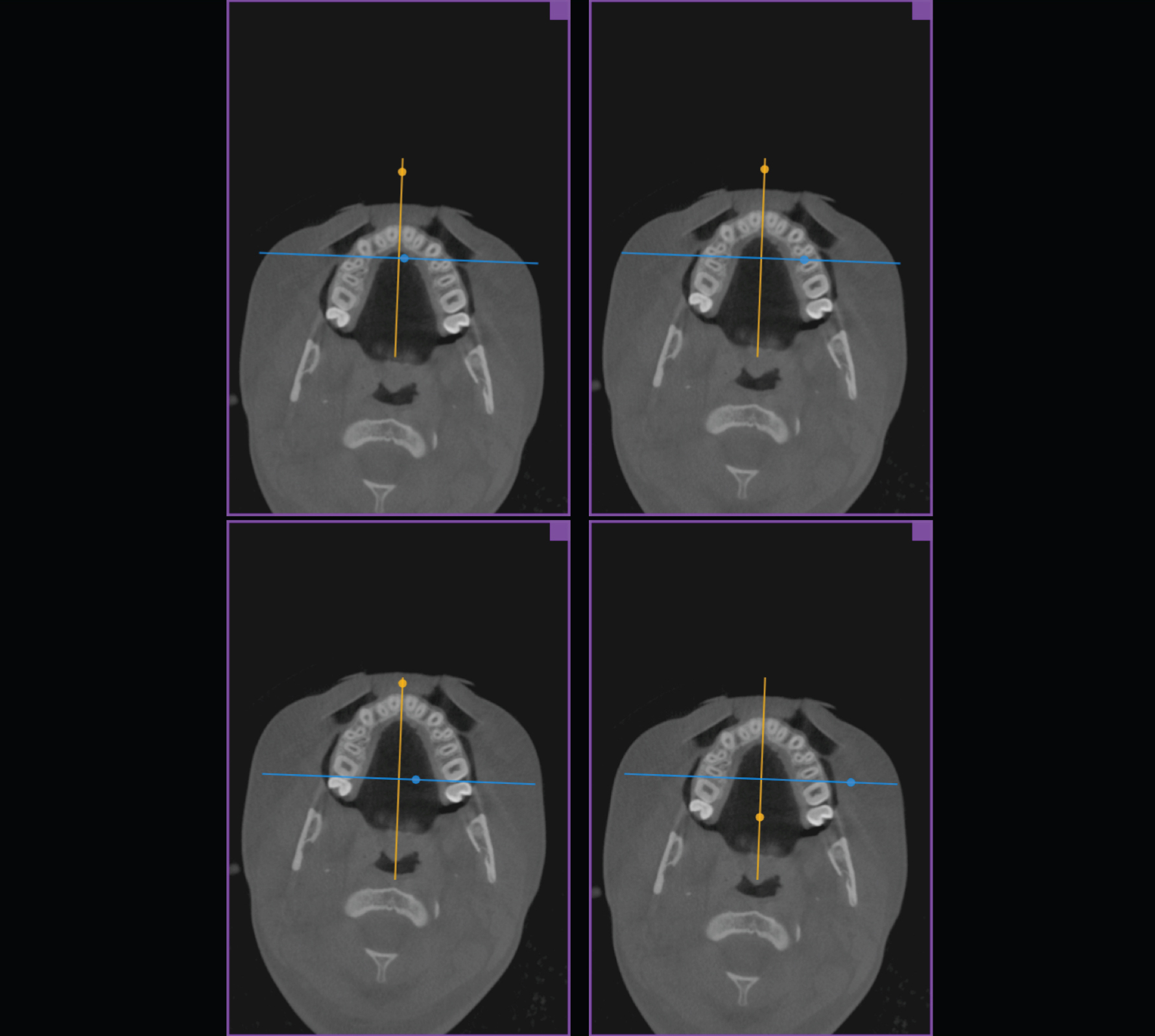
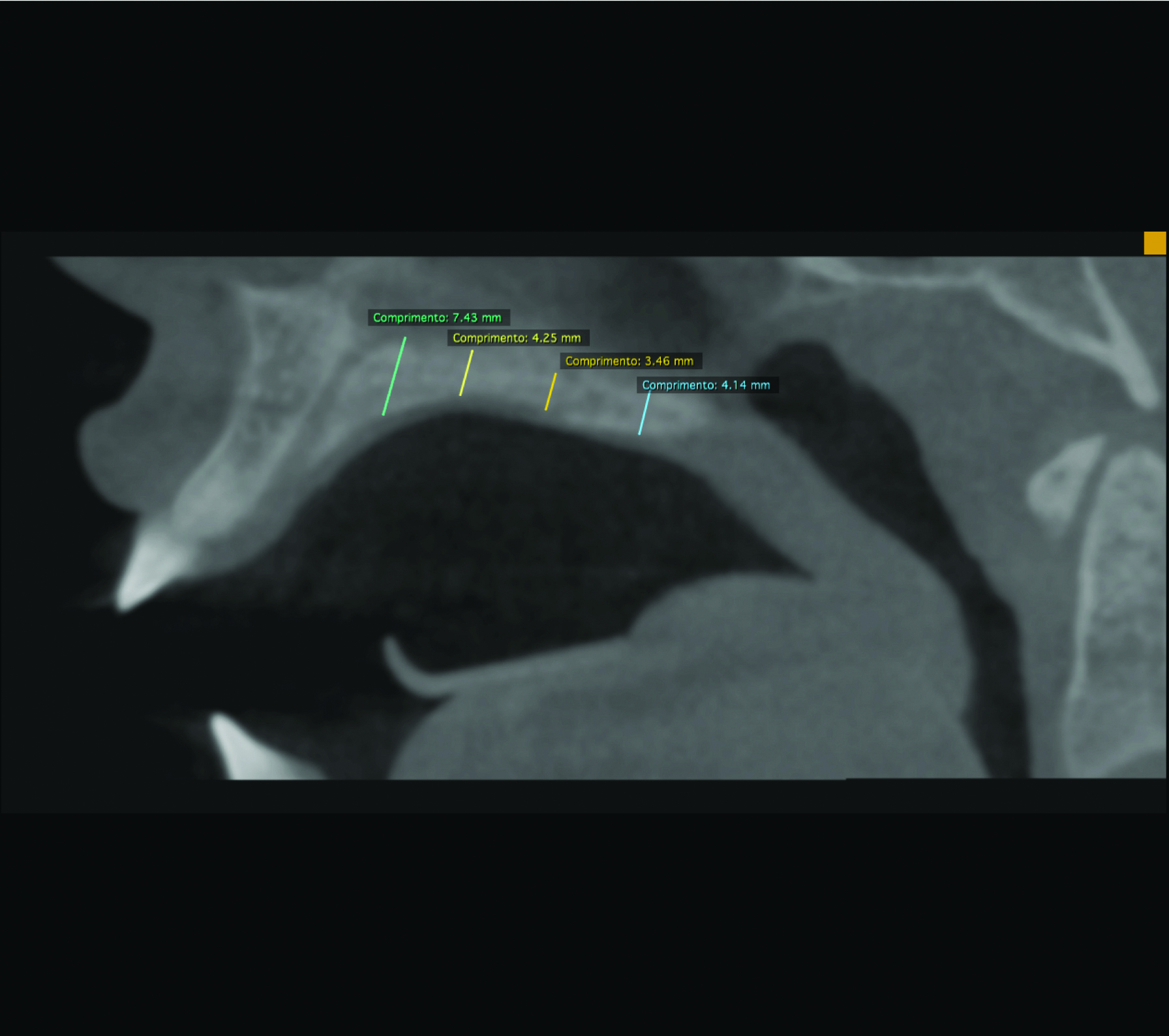
The measurements obtained in midpalatal suture area were made with the RadiAnt DICOM Viewer software, version 1.1.8.4646 (Medixant, Poznan, Poland) by the axial and coronal tomographic sections that resulted in sagittal images located exactly in the measurement area [Table/Fig-1]. Four interest areas were defined in the midpalatal suture through a line about the maxilla, to later measure palatal thickness: mesial of the first premolar (P1), mesial of the second premolar (P2), mesial of the first molar (P3), and distal of the first molar (P4) [Table/Fig-2]. Subsequently, sagittal images with previously marked lines, perpendicular to the palatal plane, were used to measure palate thickness of upper to lower cortical bone [Table/Fig-3].
Tomographic image of midpalatal suture location through axial (centre) and coronal (right corner) sections, resulting in the sagittal image (left corner).
Tomographic axial sections showing marked areas for P1, P2, P3, and P4, clockwise from the upper left corner.
Tomographic sagittal image with measurements of P1, P2, P3, and P4.
Statistical Analysis
Paired Student’s t-test was used to evaluate intra-examiner systematic error. For the casual error, the Dahlberg formula [15] was used (√∑d2/2n). All measurements were performed twice with a time interval of 15 days.
Data obtained in the study were descriptively analysed and gender differences were compared with the ANOVA test. The IBM SPSS Statistics software (SPSS for Windows, version 20.0, Armonk, NY: IBM Corp.) was used for data analysis, at 95% confidence interval.
Results
The intra-examiner error at 5% significance level showed no statistically significant difference among measurements made at different moments and the method error ranged from 0.1 to 0.2.
The average vertical bone thickness in each midpalatal suture area was 12.18 mm±3.35 for P1, 6.60 mm±2.12 for P2, 4.97 mm±0.72 for P3, and 6.36 mm±0.88 for P4. [Table/Fig-4] shows average vertical bone thickness according to gender. The greatest vertical bone thickness in midpalatal suture area was found in P1 in both male (13±2.45) and female (11.72±3.7) and the lowest for both genders was found in P3, male (5.44±0.70) and female (4.76±0.66). No significant difference observed between two genders in any midpalatal suture area.
Average thickness (mm) and standard deviation of palatal areas according to gender.
| | Women | Men | Difference | P |
|---|
| Mean±SD | Mean±SD | Mean±SD |
|---|
| P1 | 12.18±3.35 | 11.72±3.70 | 13.2±2,45 | -1.48 | 0.5* |
| P2 | 6.60±2.12 | 6.20±2.29 | 7.52±1,53 | -1.32 | 0.2* |
| P3 | 4.97±0.72 | 4.76±0.66 | 5.44±0,70 | -0.67 | 0.1* |
| P4 | 6.36±0.88 | 6.55±0.84 | 5.94±0,93 | 0.61 | 0.5* |
SD indicates standard deviations.
*Indicates no significant difference observed between two genders
Discussion
It was found that palatal vertical bone thickness analysed in young patients is greater in the anterior region, mesial to the first premolar, for both men and women. The mean values found in areas P1, P2, and P3 are higher for the male gender, but this difference was not statistically significant.
The success rate of miniscrews ranges from 70% to 89% [16-18]; however, when inserted in the palate, this rate may be close to 100% [17,18]. The success rate of miniscrews may be affected by a few factors [16] such as patients, surgical procedure, and orthodontic force, among others [16,19]. Although, these factors are not fully clarified [16], for Ludwig B et al., the determinant factor is the quality of bone adjacent to the device, installed either in the alveolar process or in the palate [5]. Regarding vertical bone thickness of midpalatal suture, Wehrbein H et al., suggested the area between first premolars is the most recommended for installing miniscrews [20]. The present study shows that the anterior palatal region has the greatest vertical bone thickness, corroborating some authors [5,21,22]. It is important to consider the presence of incisive foramen, which should be avoided when inserting mini-implants [5,10].
Although the posterior region has less vertical thickness, this does not contraindicate the installation of miniscrews, because according to Winsauer H et al., the bone characteristics presented in this location provide enough stability even under dynamic loads between 0.5 and 3 N or rotational forces [10]. These authors [10] also suggest that miniscrews with 2 mm of diameter, and 10, 12, or 14 mm of length, require approximately 5 mm of supporting bone for anchorage. It was observed in the present study that in young patients, despite the existent individual variations, the midpalatal suture presented adequate vertical bone thickness, also in the posterior region, except for the mesial region of first molars, in which the mean value obtained for patients of the female gender was 4.76 mm±0.66. In this case, shorter miniscrews would be recommended.
Holm M et al., verified palatal thickness in different areas, including paramedian regions, in patients aged 9 to 30 years, and found that mean values obtained for patients aged 9-13 years were lower than that for older patients [21]. Gracco A et al., analysed palatal vertical bone thickness in 3 different age groups: 10-15 years, 15-20 years, and 20-44 years, and found no statistically significant differences among these groups [22]. Although the scope of the present study was not to compare the palatal vertical thickness of young patients with that of adult patients, it was possible to observe that the characteristics found are similar to those of other studies [5,13,23] that analyse adult patients.
Fayed MMS et al., analysed anatomic characteristics (buccolingual bone thickness, mesial and distal space, and lingual/palatal and buccal cortical thickness) of different areas of the alveolar process in patients of both genders, and found statistically significant differences [2]. Particularly in the palatal region, Holm M et al., observed that patients of the male gender presented measurements that averaged 1.2 mm more than patients of the female gender [21]. Gracco A et al., found no differences between genders [22]. The findings of this investigation show that the thicknesses evaluated were greater for the male gender, but not significant. This similarity between measurements of palatal thickness for genders may have occurred due to limited sample size, individual variability, and because patients were young and still growing.
The results obtained in this study, as the ones of other studies; show that the palate characteristically presents thicker areas than others, which are indicated for the installation of longer miniscrews, desirable for better primary stability [19]. This anatomical knowledge does not rule out the need to analyse each patient individually, thus it is recommended to perform CBCT before inserting miniscrews in the palate, in order to diagnose not only the bone thickness of the area but also to identify the presence of inadequate bone or other complicating factors [10,21,24]. Aided by a density selection unit (HU), the area analysed showed a prevalence of D3 bone (HU 375-750), according to the classification by Misch (2008) [25]. This bone characteristic is typical of the anterior maxillary region and it may challenge the stability of the miniscrew.
Limitation
The main limitation of the present study is the small sample. Future studies should be conducted with a larger sample, also considering the ethnic and racial variations.
Conclusion
Considering the limitations of the study, it may be concluded that vertical bone thickness of midpalatal suture area of young patients is greater in the mesial region of first premolars, and although patients of the male gender have presented greater thicknesses, they were not statistically significant. Due to the variability presented in growing individuals, it is recommended CBCT to be performed before inserting miniscrews in the palate, for better planning and use of bone thickness for anchorage.
SD indicates standard deviations.
*Indicates no significant difference observed between two genders