Dysphagia Lusoria in Twins
R Hariharaprakash1, Padma Badhe2, Amit Dey3
1 Resident, Department of Radiology, Seth GS Medical College and KEM Hospital, Mumbai, Maharashtra, India.
2 Additional Professor, Department of Radiology, Seth GS Medical College and KEM Hospital, Mumbai, Maharashtra, India.
3 MBBS Student, Department of Radiology, Seth GS Medical College and KEM Hospital, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Amit Dey, Main Boys Hostel, Room-112, KEM Hospital, Mumbai, Maharashtra-400012, India.
E-mail: amit5kem@gmail.com
Four-year-old female twins presented to the hospital with chief complaint of vomiting which was immediate post-intake of solid foods. The symptoms started when they were six-month-old. Both of them had increasing intolerance to solid foods and were on semi-solid diet. They were referred to KEM Hospital, Mumbai, Maharashtra, India, for further work up because of history suggestive of a structural anomaly.
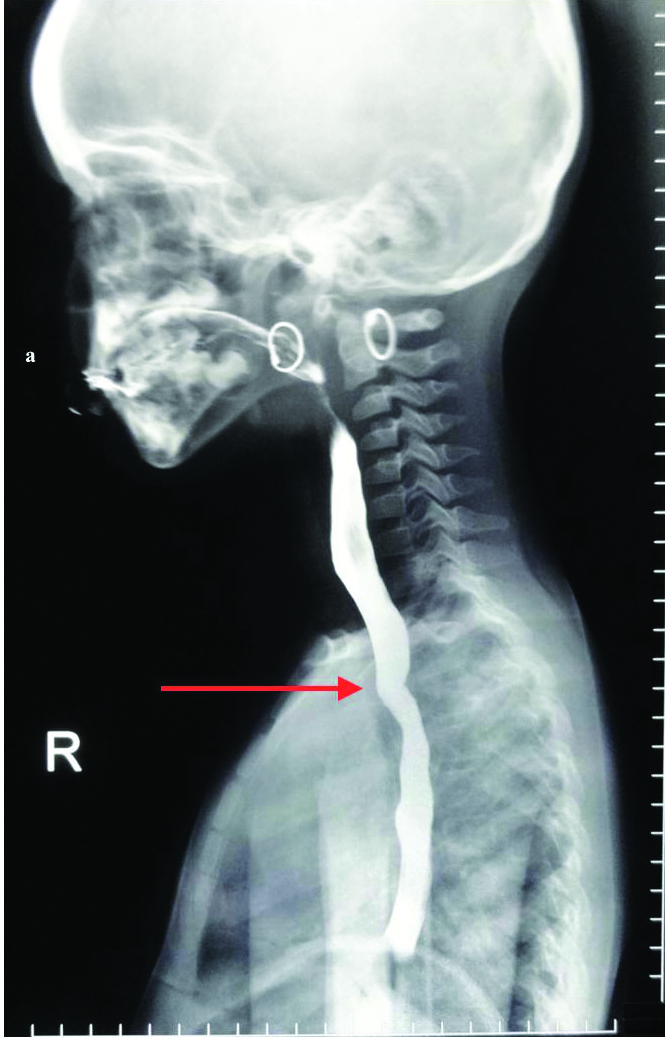
The twins were monozygotic and were weaned unsuccessfully at four months of age with semisolids. The first set of investigations included indirect and direct laryngoscopy, upper oesophago gastroduodenoscopy and oesophageal barometry but all test results were inconclusive. Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) were also done and found to be inconclusive. Echocardiography was done to rule out any cardiac defects and was found to be normal. Finally, barium oesophagogram showed constant narrowing of the oesophagus at the level of the aortic arch without any evidence of mucosal irregularity. The narrowing had an oblique orientation from inferior left to superior right on the posterior aspect of the oesophagus. This was consistent with extrinsic compression by a retro-oesophageal aberrant right subclavian artery in both the patients [Table/Fig-1a,b]. Based on the above findings, operative repair was advised.
Spot film from barium oesophagogram showed constant narrowing of the oesophagus at the level of the aortic arch without any evidence of mucosal irregularity. The narrowing had oblique orientation from inferior left to superior right on the posterior aspect of the oesophagus. This was consistent with extrinsic compression by a retro-oesophageal aberrant right subclavian artery.
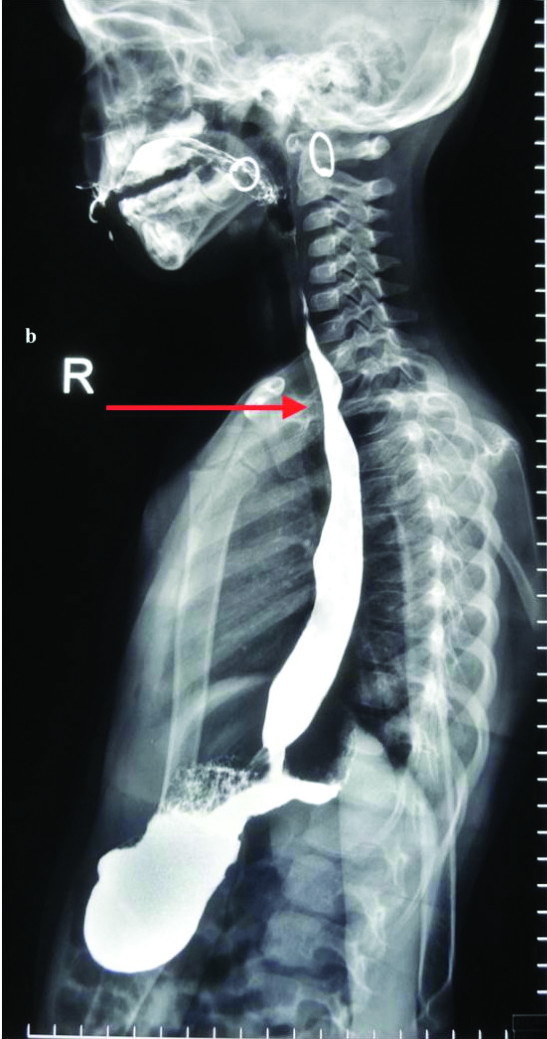
Spot film from barium oesophagogram in other twin showing similar finding consistent with aberrant right subclavian artery.
A reconstructive bypass surgery was performed with a single supra clavicular incision. The subclavian artery was divided 1 cm distal to the aortic arch. The distal portion was then anastomosed to the carotid artery. Both the children had an uneventful follow-up at one month.
Discussion
An aberrant right subclavian artery, which occurs in 0.5% to 1.8% of the population, is one of the most common embryological abnormality [1]. Thus, dysphagia lusoria is not uncommon however it has never been shown to co-occur in twins to the best of our knowledge. Most cases are asymptomatic but may become symptomatic when a “ring” completely encircles the trachea or the oesophagus leading to dysphagia lusoria [2-4]. This report examplifies the diagnosis of this condition with minimum investigations and limited radiation exposure. Any beak like posterior oesophageal wall indentation on oesophagogram unless proven otherwise should be considered vascular in origin [5]. This case also highlights the incidence of co-occurring anomalies in twins along with the genetic preponderance of vascular anomalies like dysphagia lusoria. Patients with dysphagia lusoria, that is uncomplicated by aneurysm can be successfully treated by surgery with a single supraclavicular approach. In conclusion, diagnosis of dysphagia lusoria can be managed properly with positive long-term results.
[1]. Carrizo GJ, Marjani MA, Dysphagia lusoria caused by an aberrant right subclavian arteryTexas Heart Institute Journal 2004 31(2):168-71. [Google Scholar]
[2]. Richardson JV, Doty DB, Rossi NP, Ehrenhaft JL, Operation for aortic arch anomaliesAnn Thorac Surg 1981 31:426-32.10.1016/S0003-4975(10)60994-0 [Google Scholar] [CrossRef]
[3]. Polguj M, Chrzanowski Ł, Kasprzak JD, Stefańczyk L, Topol M, Majos A, The aberrant right subclavian artery (arteria lusoria): the morphological and clinical aspects of one of the most important variations-a systematic study of 141 reportsScientific World Journal 2014 2014:29273410.1155/2014/29273425105156 [Google Scholar] [CrossRef] [PubMed]
[4]. Brown DL, Chapman WC, Edwards WH, Coltharp WH, Stoney WS, Dysphagia lusoria: aberrant right subclavian artery with a Kommerell’s diverticulumAm Surg 1993 59:582-86. [Google Scholar]
[5]. Barone C, Carucci NS, Romano C, A rare case of oesophageal dysphagia in children: aberrant right subclavian arteryCase Reports in Pediatrics 2016 2016:253937410.1155/2016/253937426904341 [Google Scholar] [CrossRef] [PubMed]