Perforation is an artificial communication between the root canal system and supporting tissues of the teeth. Root perforation complicates the treatment and deprives the prognosis if not properly managed. A wide variety of materials and techniques are available to seal the perforations. Literature shows many reviews on diagnosis, treatment plan and factors affecting the prognosis of perforation repair. Nonsurgical perforation repair should be first sort but difficulties such as extrusion and inadequate sealing of the repair material are encountered. Internal matrix concept for perforation repair provides advantage, as it helps in packing of repair material and also controls the haemorrhage from perforation site. Hydroxyapatite, collaplug, collagen are some of the materials used as matrix for perforation repair. The purpose of this case report was to describe the treatment of subcrestal perforation using absorbable collagen sponge as an internal matrix and biodentin to seal the perforation site.
Case Report
A 21-year-old female patient reported to the Department of Conservative Dentistry and Endodontics, with pain in her lower right back tooth region for past one month with no contributing medical history. She gave a history of root canal treatment in teeth 46 and 47 attempted elsewhere, about five months back and gives history of food lodgement during eating.
Clinical examination revealed there was a dislodged temporary filling in relation to 46 and 47 and 47 was tender on percussion. An intraoral periapical radiograph revealed root canal treated 46. 47 was single rooted with a faint radiolucent line connecting the pulp and periodontium and this radiolucency was subcrestal associated with periodontal ligament space widening [Table/Fig-1].
Preoperative radiograph showing subcrestal perforation in 47.

Based on American Association of Endodontists guidelines (2009), provisional diagnosis of previously initiated root canal treatment with symptomatic apical periodontitis in relation to 47 was made.
The treatment plan was to seal the perforation using absorbable collagen haemostatic sponge as carrier and biodentine to seal the perforation site, to complete the root canal treatment in 47, Dentin reinforcement using biodentine, Post endodontic restoration using full veneer metal ceramic crown in relation 46 and 47.
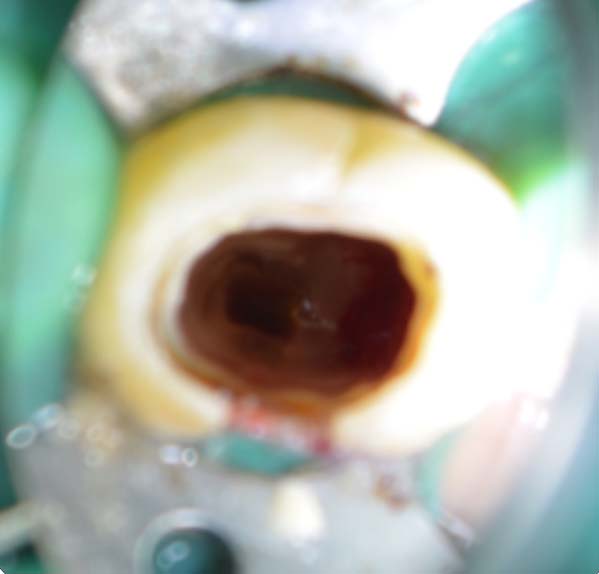
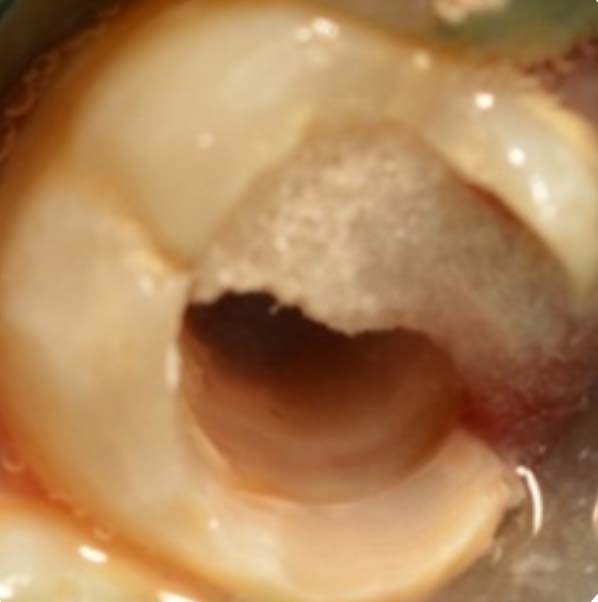
Under 1:2,00,000 dilution of adrenaline in lidocaine (Lignox 2% A), access cavity was refined and the canal orifice was located under rubber dam isolation using a dental operating microscope (Carl Zeiss, Oberkochen, Germany) [Table/Fig-2]. Subcrestal perforation was visualized under 16X magnification. Absorbable collagen sponge (Eucare India Pvt., Ltd., Chennai, India) was chosen to provide complete haemostasis and to act as a controlled barrier, to pack the Biodentin against it. Working length of 18mm was established by 40 K file (Dentsply Maillefer, Ballaigues, Switzerland) using electronic apex locator (Root ZX Mini, J. Morita Corp., Tokyo, Japan) and was confirmed by radiograph method [Table/Fig-3]. Pieces of haemostatic sponge were appropriately cut and carried into the access cavity [Table/Fig-4]. These were progressively placed into the chamber with an appropriate finger plugger (DentsplyMaillefer, Ballaigues, Switzerland) and firmly pressed through the perforation defect. A solid barrier was established. Biodentine (Biodentine, Septodont, France) was mixed and carried to the perforation site with the help of a carrier and packed with an appropriately fitted plugger. Repair of the perforation was carried out by progressive placement and packing of small increments of biodentine and it was allowed to set for 15 minutes.
Access cavity preparation and location of perforation site in 47.
Working length determination using K file in relation to 47.

Packing of absorbable haemostatic sponge at the perforation site in 47.
Biomechanical preparation was carried out using the step back method. Apical preparation was performed up to size 70 and obturation was performed by cold lateral compaction technique using guttapercha (DentsplyMaillefer, Ballaigues, Switzerland). The guttapercha was sheared upto the level of perforation and the remaining canal and access cavity was sealed with biodentine to reinforce the lost dentin followed by placement of composite restoration (Filtek Z 250, 3M ESPE, St. Paul, Minnesota, USA) for 3mm [Table/Fig-5].
Perforation repair and dentin reinforcement using biodentine.

After one month the patient was recalled and was asymptomatic. Post endodontic restoration was given using full veneer metal ceramic crowns in relation to 46 and 47. At the 6-month recall, clinical examinations showed that the tooth had no pain and no response to percussion, palpation and there were no probing depths and adequate clinical function. Radiographic findings showed adequate sealing of the perforation region [Table/Fig-6].
Six month follow up radiograph.

Discussion
Perforation can be defined as the pathological or iatrogenic communication between the rootcanal space and the periodontal tissues. Iatrogenic errors such as access cavity preparation, search for canal orifices are most commonly associated with root perforations, though non iatrogenic causes such as resorption and caries may also cause perforations. Factors that favour prognosis for treatment of perforations including time elapsed from its occurrence, detection, size, and shape and its location impact the success of the treatment [1,2].
Numerous materials are available to seal the perforation that includes Indium foil, Amalgam, Plaster of Paris, Zinc Oxide Eugenol, Super EBA, IRM (Intermediate Restorative Material), GuttaPercha, Cavit, Glass Ionomer Cement, Metal-Modified Glass Ionomer Cement. Recently Composite, Dentin chips, Decalcified Freezed Dried Bone, Calcium Phosphate Cement, Tricalcium Phosphate Cement, Hydroxyapatite, Calcium hydroxide, Portland Cement, MTA (Mineral Trioxide Aggregate), Biodentine, Endosequence, Bioaggregate and New Endodontic Cement [3].
Root perforations may compromise the treatment outcome and persist as a significant complication if not treated. Ideally, a non-surgical technique through intra-coronal placement of the repair material should be used to treat perforation [4]. Procedural difficulties such as extrusion of the repair material, inadequate sealing of the defect and lack of biocompatibility of repair materials are encountered with such an approach. Lemon RR in 1992 introduced the “internal matrix concept” for treatment of perforations [5]. He recommended the use of matrix of hydroxyapatite sealing the perforation. Collaplug, calcium sulphate, plaster of paris are used as internal matrix in the literature [6,7].
Collagen materials are being highlighted as carrier material in dentistry for revascularization, due to its space-maintaining and bio-absorbable property [8,9]. Absorbable haemostatic sponge is able to contain plenty of fluids in limited volume, and it could be removed with no residual fibre or debris [10,11]. Most important point is that collagen dose not interfere with bone and soft tissue healing, because it is biologically absorbed even when it is left in the surgical cavity [12,13]. Open-apex teeth with placement of an apical matrix using collagen sponge against which MTA apical plug had favourable prognosis [14]. One major disadvantage of absorbable collagen sponge is it lacks the property of osseoinduction and osseoconduction.
Calcium hydroxide had numerous disadvantages as a perforation repair material. To overcome the disadvantages, MTA is used since 1990. MTA has certain disadvantages like poor handling properties and long setting time. To overcome all these disadvantages biodentine came to use due to its properties like ease of handling, faster setting time, biocompatibility and early mineralization [15].
Biodentine is a calcium silicate-based bioactive material of powder-liquid system. It is calcium silicate based cements in which liquid contains calcium chloride accelerating setting time. The calcium silicate interacts with water leading to the setting and hardening of the cement. Hydration of the tricalcium silicate produces a hydrated calcium silicate gel and calcium hydroxide. It is easy to handle owing to its ease of manipulation and a short setting time approximately 12 minutes, has high alkaline Ph [16]. It has properties such as tissue regeneration and early mineralisation, anti-bacterial properties, biocompatible, good push out bond strength. Biodentine has elastic modulus of 22.0 Gpa and is similar to that of dentine at 18.5, Compressive strength of about 220 MPa is equal to average for dentine of 290 MPa Microhardness of biodentine at 60 HVN is same as that of natural dentin. Guneser MB et al., reported that biodentine showed considerable performance as a perforation repair material compared to MTA [17].
Conclusion
Perforation repair is a frustrating problem to the dentist. So through idea regarding its restorability is essential which includes knowledge of site, size, time of perforation and various materials used. The purpose of this article is to present a case report in which absorbable collagen sponge was used as an internal matrix, and biodentine was used to seal the perforation. Immediate repair with good repair material and trying to be less invasive as possible ensures successful outcome despite complexity of the condition.
[1]. Tsesis I, Fuss Z, Diagnosis and treatment of accidental root perforationsEndod Top 2006 13(1):95-107.10.1111/j.1601-1546.2006.00213.x [Google Scholar] [CrossRef]
[2]. Matsumoto T, Nagai T, Ida K, Ito M, Kawai Y, Horiba N, Factors affecting successful prognosis of root canal treatmentJ Endod 1987 13(5):239-42.10.1016/S0099-2399(87)80098-5 [Google Scholar] [CrossRef]
[3]. Kakani AK, Veeramachaneni C, Majeti C, Tummala M, Khiyani L, A review on perforation repair materialsJ Clin Diagn Res 2015 9:ZE09-13.10.7860/JCDR/2015/13854.650126501031 [Google Scholar] [CrossRef] [PubMed]
[4]. Regan JD, Witherspoon DE, Foyle D, Surgical repair of root and tooth perforationsEndod Top 2005 11(1):152-78.10.1111/j.1601-1546.2005.00183.x [Google Scholar] [CrossRef]
[5]. Lemon RR, Nonsurgical repair of perforation defects. Internal matrix conceptDent Clin North Am 1992 36:439-57. [Google Scholar]
[6]. Zou L, Liu J, Yin S, Li W, Xie J, In vitro evaluation of the sealing ability of MTA used for the repair of furcation perforations with and without the use of an internal matrixOral Surg Oral Med Oral Pathol Oral Radiol Endod 2008 105(6):e61-65.10.1016/j.tripleo.2008.01.03818417384 [Google Scholar] [CrossRef] [PubMed]
[7]. Alhadainy HA, Himel VT, An in vitro evaluation of plaster of Paris barriers used under amalgam and glass ionomer to repair furcation perforationsJ Endod 1994 20(9):449-52.10.1016/S0099-2399(06)80036-1 [Google Scholar] [CrossRef]
[8]. Petrino JA, Boda KK, Shambarger S, Bowles WR, McClanahan SB, Challenges in regenerative endodontics: a case seriesJ Endod 2010 36(3):536-41.10.1016/j.joen.2009.10.00620171379 [Google Scholar] [CrossRef] [PubMed]
[9]. Ferris DM, Baumgartner JC, Perforation repair comparing two types of mineral trioxide aggregateJ Endod 2004 30(6):422-24.10.1097/00004770-200406000-00011 [Google Scholar] [CrossRef]
[10]. Chvapil M, Collagen sponge: theory and practice of medical applicationsJ Biomed Mater Res 1977 11:721-41.10.1002/jbm.820110508893491 [Google Scholar] [CrossRef] [PubMed]
[11]. Stein MD, Salkin LM, Freedman AL, Glushko V, Collagen sponge as a topical haemostatic agent in mucogingival surgeryJ Periodontol 1985 56(1):35-38.10.1902/jop.1985.56.1.353856007 [Google Scholar] [CrossRef] [PubMed]
[12]. Mannai C, Leake D, Pizzoferrato A, Ciapetti G, Sangiorgi C, Histologic evaluation of purified bovine tendon collagen sponge in tooth extraction sites in dogsOral Surg Oral Med Oral Pathol 1986 61(4):315-23.10.1016/0030-4220(86)90408-1 [Google Scholar] [CrossRef]
[13]. Jang Y, Kim H, Roh BD, Kim E, Biologic response of local haemostatic agents used in endodontic microsurgeryRestor Dent Endod 2014 39(2):79-88.10.5395/rde.2014.39.2.7924790919 [Google Scholar] [CrossRef] [PubMed]
[14]. Graziele Magro M, Carlos Kuga M, Adad Ricci W, Cristina Keine K, Rodrigues Tonetto M, Linares Lima S, Endodontic management of open apex teeth using lyophilized collagen sponge and MTA cement: report of two casesIran Endod J 2017 12(2):248-52. [Google Scholar]
[15]. Priyalakshmi S, Ranjan M, Review on biodentine-a bioactive dentin substituteIOSR J Dent Med Sci 2014 13:13-17.10.9790/0853-13131317 [Google Scholar] [CrossRef]
[16]. Han L, Okiji T, Uptake of calcium and silicon released from calcium silicate-based endodontic materials into root canal dentineInt Endod J 2011 44(12):1081-87.10.1111/j.1365-2591.2011.01924.x21777256 [Google Scholar] [CrossRef] [PubMed]
[17]. Guneser MB, Akbulut MB, Eldeniz AU, Effect of various endodontic irrigants on the push-out bond strength of biodentine and conventional root perforation repair materialsJ Endod 2013 39(3):380-84.10.1016/j.joen.2012.11.03323402511 [Google Scholar] [CrossRef] [PubMed]