Introduction
Forensic science is the application of knowledge of various branches of science to criminal and civil laws. The present era in forensic science has seen a paradigm shift with utilisation of art and science. It has expanded its arena to include various technological advances and approaches that focus on the overall development of this science. Forensic science now allows alternative branches to come together and work in an integrated approach towards crime scene investigation/disaster victim identification/facial reconstruction.
Multiple approaches have been employed for forensic identification of individuals, of which FFA serves as a controversial yet important adjunct when all quintessential identification techniques cease to show result.
FFA is scientific and artistic recreation of face from skull of deceased person for establishing his/her identity [1]. FFA utilises blending of various disciplines including anthropology, anatomy, dentistry and most importantly craftsmanship to artistically recreate facial structures. Ideally FFA team should be composed of experts from various disciplines, but as of now being managed by anatomist and forensic specialist alone.
A thorough search of literature using search engines (PubMed, Scopus and Google Scholar) and hand search was done to enumerate skills that can be utilised for FFA. After careful appraisal, we propose inclusion of a dental expert (preferably a forensic odontologist) to be a part of FFA team based on their sound scientific knowledge about human anatomy, musculature as well as exposure to various hard tissue and soft tissue landmarks that are taught as a part of BDS (undergraduate) curriculum. In addition, their practical training also includes honing their artistic handiwork with adept use of various hand instruments that may prove extremely beneficial when working on the skull.
Both forensic anthropologists and forensic odontologists can together decipher problems associated with craniofacial identification. They can also collaborate in museum model reconstructions out of skull bones. Both the subjects are very much related and are concerned with the analysis of calcified structures of the body, namely the bones and the teeth. The bones and teeth of the craniofacial complex are key recognition tools for the forensic odontologist. Dental profiling and skull analysis are effectively used to determine the race, age and sex of a person [2].
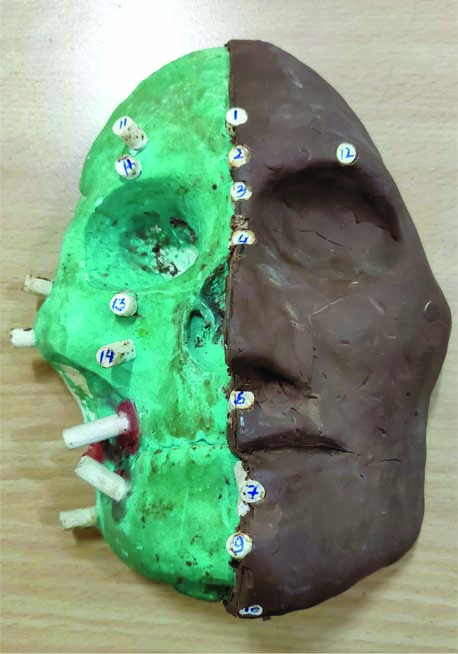
Concept of FFA: Skull acts like a mechanical support and overlying soft tissues cover defines facial appearance. Measuring of soft tissue thickness on hard tissue landmarks of skull leads to generation of metric and non-metric data. This data may be utilised to recreate approximate contour of face, therefore the term facial approximation is used [3]. [Table/Fig-1] Illustrates in-house facial reconstruction at a dental college laboratory on a dental stone replicated skull. Right side shows tissue depth markers. Dental modeling wax has been used in orientation of tissue depth markers.
In-house facial reconstruction using dental stone replicated skull. Right side shows tissue depth markers.
Wilkinson C, 2010 in her review article has enumerated that facial reconstruction technique involves three elements: 1) Anatomical modeling; 2) Morphology determination; and 3) Depiction of resulting face to the public [4]. A forensic odontologist can be involved in each of these stages mentioned and can play a pivotal role in sculpturing the correct reconstruction.
Stage 1 (Anatomical modeling): The first stage in facial reconstruction involves modeling of muscles and relevant anatomical structures on skull, utilising strict anatomical guidelines of origin and insertion and a thorough knowledge of their existing variations [4]. Anatomical milieu is provided to dental undergraduate and postgraduate students in first year of their dental curriculum. They are qualified to interpret normal anatomical features as well as deviation from normal, both theoretically and with hands-on dissection sessions. This knowledge may be put to practical use by forensic odontologist in FFA in location of anatomical points, assessment of corresponding soft tissue thickness and approximation of facial musculature.
In addition, forensic odontologists are well versed with dental anatomy that is taught as a part of their undergraduate curriculum. The practical training of dental anatomy involves dental carving by use of various hand instruments to create tooth like structures. This manual dexterity would serve extremely beneficial while moulding of clay and alike materials to create facial features. Routine postings in dental undergraduate clinical departments allows the forensic odontologists to have hands-on experience with manipulation and managing of various dental materials (like clay/plaster/die-stone/acrylic etc.,) materials that may serve as adjuncts for effective replication and orientation of skull and facial approximation.
This stage of anatomical modeling is comparatively easy. This stage has relatively low level of sculptural expertise and higher level anatomical acquaintance involved, however the knowledge and clinical experience imparted to dental undergraduates, as mentioned above, may serve effective in reducing challenges associated with this stage of FFA [4].
Stage 2 (Morphology determination): The morphology of soft tissue envelope over the bony housing in the critical areas of nose, ear as well as mouth governs the overall morphology of face, that may be governed by changes in age as well as gender. Dental undergraduate are well versed with these morphological changes, taught to them theoretically in undergraduate subjects. A special mention in this regard, would be a landmark study by Nanda RS (1990) where longitudinal changes were evaluated in soft tissue of both male and female Caucasian population between 7 and 18 years with age [5]. The results of this study may be taken as reference for selection of facial parameters for reconstruction that show changes with age and gender including nose height, nose depth, nose inclination, upper and lower lip height and thickness, nasolabial inclination, chin thickness and its inclination. This also highlights the importance of familiarity of age and gender of individual prior to beginning the reconstruction.
An additional criterion important for FFA would be knowledge of facial profile of individual as it has a bearing on articulation of maxillary and mandibular jaws as well as occlusion of teeth. This has also been well highlighted in inclusion of subjects for this study, with Class I molar relationship and normal facial profile. This kind of facial articulation is taught at the dental undergraduate level, hence further emphasising the importance of forensic odontologist in improving accuracy of facial approximation.
For approximation of facial features of an individual on skull, the study of balance and harmony of face is important. Dental undergraduates are taught scientific and evolutionary basis of this symmetry called divine proportion or golden proportion or phi (Φ), that is geometrically equal to 1:1.618 or even as a proportional number (...3:2, 5:3, 8:5, 13:8...) [6]. This divine proportion has been the basis of a beauty mask developed by Marquardt SR and Stephen R in 2002, alleging it to be applicable to every attractive face, irrespective of age and race [7]. The strong evolutionary significance of this golden proportion has been carried from Egyptian and Babylon dynasties, representing ideal correlation of parts, be it in their pyramids of Giza or cult constructions or bas-relieves or ornaments, and more recently extending to parts of human body, or to be more exact, teeth and denture [8-10]. This golden proportion also extends to various vertical and transverse parameters of facial skeleton, studied in photographs and radiographs. Further, it extends to macroesthetic entities of smile like visibility of teeth on posed smile and also ratio of vertical and horizontal dimensions of teeth, as proposed by Rickets RM [6]. A forensic odontologist (also a dental professional) who customarily incorporates this proportion during assessment of face and related structures for diagnosis and treatment planning may use this expertise while performing FFA.
In addition, study of facial morphology in light of physical anthropometric data necessitates some terminologies used in craniometry as well as cephalometry which may be used universally by various researchers for undaunted communication in forensics. Of these, most frequently used craniometric measurements are cranial index (which classifies skull types as brachycephalic, mesocephalic and dolichocephalic based on ratio of skull width to skull length), and related facial index (classifying the face as euryprosopic, mesoprosopic and leptoprosopic based on morphological facial height and bizygomatic width), which are most frequently used by dental experts worldwide [11,12].
Dental literature studied by dental undergraduates (or forensic odontologist) gives an all inclusive view about articulation of maxillary and mandibular jaw bases to the skull and their corresponding occlusal patterns. These are critical elements in facial reconstructions since it has significant bearing on facial profile and related soft tissue thickness. First classification for dental irregularities was given by Fox based on labial or lingual locking of upper front teeth to the lower. However, the system of classification which is still applicable was proposed by Angle EH in 1899, wherein Class I denotes normal relationship of upper and lower jaws and teeth while Class II and Class III show abnormal jaw patterns, with lower teeth occluding distal to upper in Class II and occluding mesial to upper in the latter by the width of a bicuspid tooth [13-15]. These patterns of dental and skeletal malocclusion are assessed clinically as well as on cephalograms, which are routinely taught to final year BDS students. Besides, clinical and cephalometric measurements, these malocclusions can also be distinguished by adjunctive measures like rugae pattern [16]. An Integrated Rugoscopy Chart (IRC) has been recently proposed to establish this rugae pattern which may be used in further research in malocclusion [17,18].
A more detailed knowledge about skeletal Class II and Class III patterns would aid the forensic team in resurrection of morphologic interrelations of cranium, facial skeleton as well as teeth. Class III has been attributed to protruding chins, deficient premaxilla or overdeveloped ramus or due to inter-dentitional patterns related to functional adaptation of upper and lower teeth. [19-21]. On the other hand, Class II has been related to a more posterior position of body of mandible to the maxilla and a more acute mandibular plane angle than Class I subjects [22]. Even roentgenographic studies provide evidence of posteriorly positioned chin, mandibular length shorter than SN length and decreased lower posterior facial height in skeletal Class II while Class III shows increased gonial angle, decreased ramal width and acute occlusal plane to lower border of mandible [23-25].
Dental research based studies are instrumental in providing tissue thickness data for individuals of different ethnicity, age, sex, body-mass and facial profile, that prove essential for performing FFA. Forensic odontolgist may also be a coordinator or design CBCT or other radiologic population based studies for generation of mass local database, that may ultimately be translated on for FFA skull with help of anatomist along with forensic anthropologist.
Stage 3 (Depiction of resulting face to the public): This particular stage involves adornment of face with recognisable traits related to skin colour, age related changes, wrinkles, facial hair, also eye colour, hair or clothing. The proficiency of forensic odontologist in various dental age estimation techniques may prove beneficial in this stage as prediction of age may be the first step towards applicability of age related changes on the skin. Demirjian a radiographic technique based on stages of development of teeth, is still considered to be the gold standard in age estimation of growing individuals, although various other techniques have also been proposed. The colour of teeth as elements of recognition are also correlated to the skin colour as well as race, that are well studied in dental undergraduate prosthodontic curriculum while selection of hue, chroma of teeth for denture patients.
Conclusion
The use of odontology in facial reconstruction endeavors artistic sculpturing of facial features over the cranium, mandible and associated dentitions with sound scientific basis as well as practical experience with various hand instruments and dental materials. FFA operates under the theoretical framework that facial features follow the contour of the underlying bones. Since the skull bone does not yield soft tissue details, hence the final result is only approximation of the actual face.
In order to achieve greater accuracy in FFA, it is suggested by the authors that the forensic artist should work in collaboration with a forensic anthropologist and a forensic odontologist, using the most current tissue depth data applicable to different ethnic populations and contemporary practices [26,27]. [Table/Fig-2] summarises skills and attributes of Indian dentists having applicability in forensic facial reconstruction. Reddy G et al., in a review article have highlighted how orthodontist can play a major role in identification of victims or suspects by maintaining proper diagnostic records [28].
Skills and attribute of Indian dentists having applicability in forensic facial reconstruction.
| S No. | Skills and attribute | Which year of BDS undergraduate course* | Applicability |
|---|
| 1. | Extraoral and intraoral photography | Third year and final year, Oral Medicine and Radiology, Orthodontics | -3D superimposition-Photographic landmarks and analysis can be easily comprehended |
| 2. | Radiographic records (routine dental records) |
| Lateral cephalogram | Third year and final year, Oral Medicine and Radiology, Orthodontics | -Location of cephalometric landmarks-Hard tissue and soft tissue analysis for facial reconstruction-Cephalometric metric population based database for different ethnic populations |
| CBCT | Final year, Oral Medicine and Radiology, Orthodontics | -Accuracy in locating hard tissue landmarks-Accurate soft tissue thickness metric records-CBDT metric population based database for different ethnic populations |
| 3. | Dental records | Third year and final year, Oral Medicine and Radiology, Orthodontics | -Different malocclusions, their dental and related skeletal pattern, articulation of jaws, any related pathologies |
| 4. | Dental carving | First year, Dental Anatomy and Dental Histology | Dexterity of using hand instruments for creating tooth structures as well as manipulating clay for facial reconstruction |
| 5. | Anatomy and musculature origin and insertion | First year, General Human Anatomy | -Well versed with various facial bones-Anatomical landmarks location-Facial expression and accuracy of muscle reconstruction on the face |
| 6. | Growth changes | First year, General Human Anatomyfinal year, Orthodontics | Changes on face with growth in facial skeleton, musculature |
*As per Dental Council of India (DCI) undergraduate dental curriculum
Disclaimer
The FFA figures used in this article are just to stimulate a discussion on the title. Facial soft tissue thickness data derived in study by Sahni D et al., was used for reconstruction on dental stone replica of skull [29]. In no way any work was done directly on human/animal bones. The information in this article is both factual and fictional since they are personal opinion formulated by authors after reviewing literature.
This proposal was partially presented by first author of this manuscript as a scientific poster in September 2017 at Triennial IOFOS Conference on Forensic Odontology held at Leuven.
*As per Dental Council of India (DCI) undergraduate dental curriculum
[1]. Fernandes CM, Pereira FD, da Silva JV, Serra Mda C, Is characterizing the digital forensic facial reconstruction with hair necessary? A familiar asssessors’ analysisForensic Sci Int 2013 229:164.e1-e5.10.1016/j.forsciint.2013.03.03623622792 [Google Scholar] [CrossRef] [PubMed]
[2]. Luntz L, History of forensic dentistryDent Clin North Am 1977 21(1):07-17. [Google Scholar]
[3]. Iscan MY, Introduction of Techniques for Photographic Comparison: Potential and Problems. In: ISCAN, MY, Helmer RO (eds.)Forensic Analysis of the Skull: Craniofacial Analysis, Reconstruction, and Identification 1993 New York, Wiley- Liss:57-70.ISBN 0471560782 [Google Scholar]
[4]. Wilkinson C, Facial reconstruction-anatomical art or artistic anatomy?J Anat 2010 216(2):235-50.10.1111/j.1469-7580.2009.01182.x20447245 [Google Scholar] [CrossRef] [PubMed]
[5]. Nanda RS, Meng H, Kapila S, Goorhuis J, Growth changes in the soft tissue facial profileAngle Orthod 1990 60(3):177-90. [Google Scholar]
[6]. Ricketts RM, The biologic significance of the divine proportion and Fibonacci seriesAm J Orthod 1982 81:351-70.10.1016/0002-9416(82)90073-2 [Google Scholar] [CrossRef]
[7]. Marquardt SR, Stephen R, Marquardt on the Golden Decagon and human facial beauty. Interview by Dr GottliebJ Clin Orthod 2002 36:339-47. [Google Scholar]
[8]. Vadachkoriia NR, Gumberidze NSh, Mandzhavidze NA, “Golden proportion" and its application to calculate dentitionGeorgian Med News 2007 (142):87-94. [Google Scholar]
[9]. Vegter F, Hage JJ, Clinical anthropometry and canons of the face in historical perspectivePlast Reconstr Surg 2000 106:1090-96.10.1097/00006534-200010000-0002111039382 [Google Scholar] [CrossRef] [PubMed]
[10]. Farkas LG, Munro IR, Anthropometric facial proportions in Medicine 1986 SpringfieldCharles C. Thomas Publisher [Google Scholar]
[11]. Ricketts R, A foundation for cephalometric communicationAm J Orthod 1960 46(1):230-57.10.1016/0002-9416(60)90047-6 [Google Scholar] [CrossRef]
[12]. Franco FCM, Araujo TM, Vogel CJ, Quintão CCA, Brachycephalic, dolichocephalic and mesocephalic: Is it appropriate to describe the face using skull patterns?Dental Press J Orthod 2013 18(3):159-63.10.1590/S2176-9451201300030002524094027 [Google Scholar] [CrossRef] [PubMed]
[13]. FoxOrthodontia: its origin, evolution, and culmination as a specialityDent Cosmos 1803 62:14[Cited by Hellman 1920] [Google Scholar]
[14]. Angle EH, Classification of malocclusionDent Cosmos 1899 41:248 [Google Scholar]
[15]. Sanborn RT, Differences in the facial skeletal patterns of Class III malocclusion and normal occlusionThe Angle Orthodontist 1955 25(4):208-22. [Google Scholar]
[16]. Kapoor P, Ragini Kaur H, Rugoscopy: a diagnostic appurtenance for malocclusion or just a forensic aid?-a pilot studyJournal of Forensic Research 2015 6(2):110.4172/2157-7145.1000272 [Google Scholar] [CrossRef]
[17]. Chowdhry A, A simple working type Integrated Rugoscopy Chart proposed for analysis and recording rugae patternJournal of Forensic Dental Sciences 2016 8(3):171-72.10.4103/0975-1475.19510628123273 [Google Scholar] [CrossRef] [PubMed]
[18]. Shukla D, Chowdhry A, Bablani D, Jain P, Thapar R, Establishing the reliability of palatal rugae pattern in individual identification (following orthodontic treatment)J Forensic Odontostomatol 2011 29(1):20-29. [Google Scholar]
[19]. Dewey M, Practical Orthodontia 1919 4th edSt LouisCV, Mosby Co [Google Scholar]
[20]. Goddard CL, Orthodontia 1900 PhiladelphiaLea brothers ad Co. [Google Scholar]
[21]. Lischer BC, Principles and methods of orthodontics 1922 PhiladephiaLea and Febiger [Google Scholar]
[22]. Moore GR, Heredity as a guide in dentofacial orthopaedicsA Assoc Ortho. 42nd Annual Meeting 1944 [Google Scholar]
[23]. Hellman M, Studies on the etiology of Angle’s Class II malocclusal manifestationInt J Orth Oral Surg 1922 8:129-48.10.1016/S0099-6963(22)80015-6 [Google Scholar] [CrossRef]
[24]. Drelich RC, A cephalometric study of untreated Class II div 1 malocclusionThe Angle Orthodontist 1948 18:70-75. [Google Scholar]
[25]. Bjork A, The face in profileSvenske Tandlal.are Tkidskrift 1947 40(No. 5B) [Google Scholar]
[26]. Bayat M, Shariati M, Rajaeirad F, Yekaninejad MS, Momen-Heravi F, Davoudmanesh Z, Facial anthropometric norms of the young Iranian populationJ Maxillofac Oral Surg 2018 17(2):150-57.10.1007/s12663-016-0897-329618878 [Google Scholar] [CrossRef] [PubMed]
[27]. Stephan CN, Sievwright E, Facial Soft Tissue Thickness (FSTT) estimation models-And the strength of correlations between craniometric dimensions and FSTTsForensic Sci Int 2018 286:128-40.10.1016/j.forsciint.2018.03.01129574348 [Google Scholar] [CrossRef] [PubMed]
[28]. Reddy G, Reddy VP, Sharma M, Aggarwal M, Role of orthodontics in forensic odontology-a social responsibilityJ Clin Diagn Res 2016 10(4):ZE01-ZE03.10.7860/JCDR/2016/15798.763327190968 [Google Scholar] [CrossRef] [PubMed]
[29]. Sahni D, Sanjeev Singh G, Jit I, Singh P, Facial soft tissue thickness in northwest Indian adultsForensic Science International 2008 176(2-3):137-46.10.1016/j.forsciint.2007.07.01217997243 [Google Scholar] [CrossRef] [PubMed]