According to statistics released by the United Nations, an estimated 232 million people were classified as immigrants (approximately 3% of the world’s population). United Nations International Migration reports that the number of international migrants has increased significantly during the past 15 years, reaching 244 million in 2015 [1]. For decades, multiple factors such as war, insecurity, violence, drought and unemployment have led many Afghans to seek refuge abroad in Iran [2]. Iran is the third host country in the world for Afghan refugees with an open door policy towards immigration leading to allocation of a substantial part of national budget to subsidise basic necessities, transport, education, and health services for this population [3,4].
According to the reports of the United Nations High Commissioner for Refugees (UNHCR), despite signing a tripartite agreement with Afghanistan government to voluntary returning Afghans to their countries in 2002 followed by returning more than half of Afghans to their country, the residency of remaining population has imposed a heavy financial burden on Iran government especially in healthcare system [4]. The presence of these foreign nationals has imposed multiple challenges, such as new health risks. At present, approximately 24% of registered refugees are considered vulnerable, and this situation is expected to affect increasing numbers of refugees [5]. Iran is one of the most concentrated areas of Afghan migrants and refugees. In Iran, there are 1 million documented Afghan refugees that have access to health services and 2 million undocumented Afghan migrants. This openness to refugees and recognition of their social rights is very unusual in the international scene. [6]. Hyperinflation in the country has affected the delivery of services by different government sectors. There has also been a dramatic rise in the cost of living, including food items, other basic needs, health services and education-related costs. This has affected the refugee population in particular.
Materials and Methods
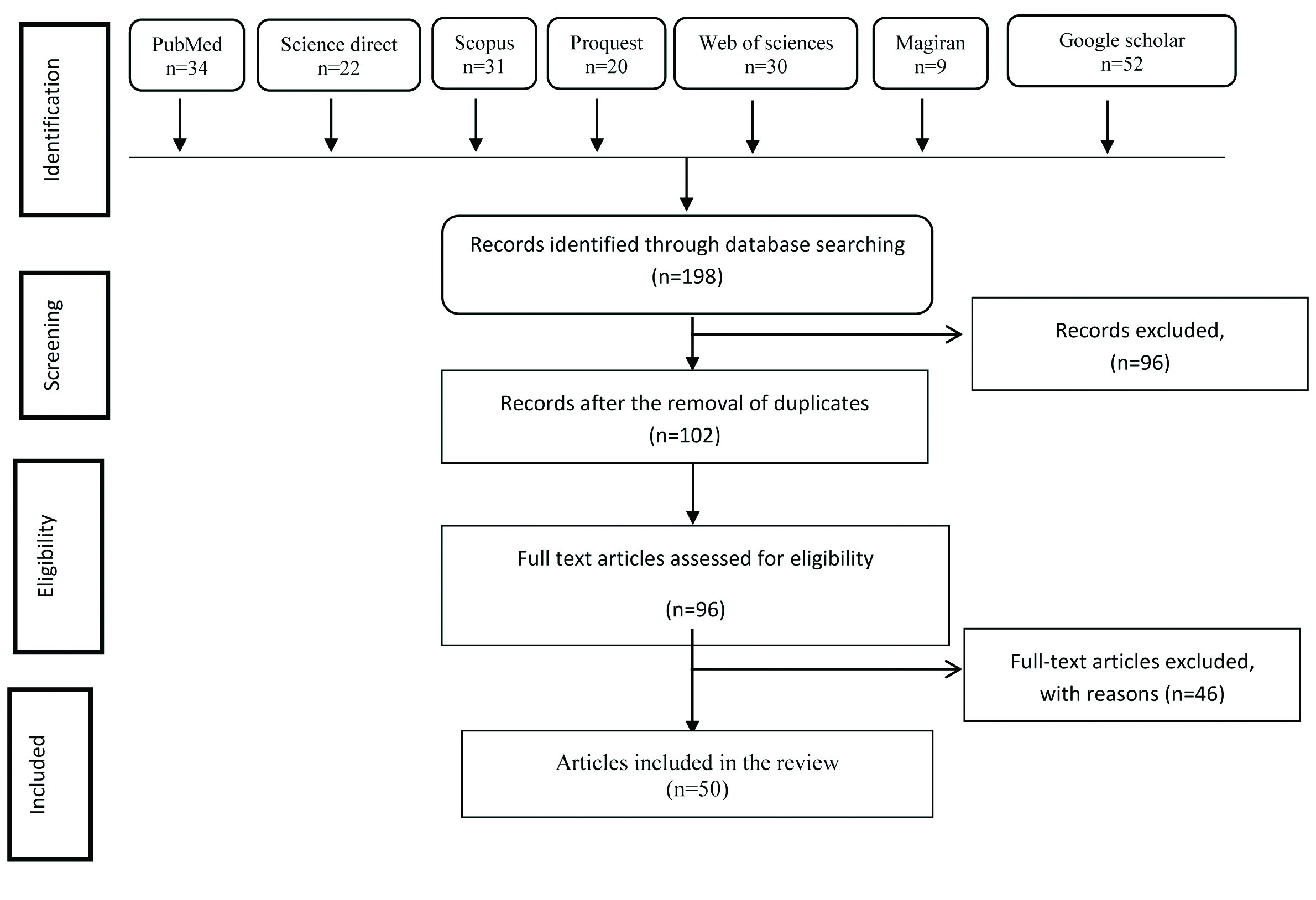
A literature review using electronic database such as MEDLINE, EMBASE, Science direct, Scopus, Cochrane Library, Google Scholar and Persian databases including Iran Medex, SID, Irandoc, Magiran was performed for studies between January 1994 and July 2017. Gray literature, reference lists of relevant studies as well as key journals were searched for additional studies. Mesh key terms were formed by combining “Afghan refugees” OR “Afghan immigrants” OR “Afghan populations” with at least one of the following terms: “health status”, “communicable diseases”, “non-communicable diseases”, “health service”, “food security” using the Boolean operator “AND”. A search strategy was built by applying the advanced search capability of the search engine. All cross-sectional, longitudinal, experimental, cohort or case-control analytical designs and reports were included. Based on this search strategy, only those articles that had one of the keywords, in either the title or abstract, were retrieved. The studies without numerical outcome data were excluded.
Two authors independently evaluated the 198 search results in terms of eligibility and resolved cases of disagreement through consensus. After initial assessments, 102 irrelevant and duplicate studies were excluded. The abstracts and titles of the remaining 96 articles were then reviewed. In the next stage, the full texts of the remaining articles were evaluated and 46 studies which did not match the aim and/or inclusion criteria of this systematic review were excluded. Finally, 50 eligible articles were reviewed [Table/Fig-1].
Flow diagram depicting the search items at different stages.
Results
Demographic Profile of Afghan Immigrants
At the peak of the Afghan refugee’s crisis in 1991, around 3 million Afghans have been hosted by Iran. The soviet occupation of Afghanistan resulted in a massive influx of 2.9 million Afghans into Iran between 1980 and 1989. Based on UNHCR statistics published in 2002, within the year 1993, 1994 the population of concern of UNHCR among the Afghan refugees respectively stood over 1,850,000 and 1,623,331 person [17]. However, there is no information on exact number of unregistered Afghan migrants at the same period. The number of documented Afghan refugees in Iran decreased in 1993 until the year 2000 that had a peak again with 1,482,000 refugees reported at this year and in 2001. Later in 2001 the number of Afghan refugees showed constant reduction whereas the latest official report by UNHCR 2013 indicate the presence of 8,40,000 Afghan refugees in Iran [18]. The gender and age distribution of Afghan refugees has not been equivalent during these years. Socioeconomic condition of both countries along with war and insecurity in Afghanistan influenced the demography of Afghan migrants in Iran. By the end of 2005 the number of Afghan female refugees reported as 426,877. The number of children under five years and between 5-17 years of age, both in girls and boys at the same period were 41,549 and 4,04,280 respectively. Besides the individuals who cross the borders and arrive in Iran as refugees, there is another group of Afghan migrants who are born or raised in Iran. They are called as second generation of Afghan refugees and at least have one Afghan parent or have spent more than half of their life in Iran. Some of them have never been to Afghanistan. The total number of documented Afghans aged between 15 and 29 years living in Iran is 341,157 or 33.4% of the total population of Afghans in Iran [4]. The Afghan immigrant population is relatively young in Iran with a median age of 31 years. In compliance with the world trend, in 2015 less than half of the international immigrants in Iran were women (47%) [15].
Health Status of Afghan Immigrants
Reviewing the published reports in valid databases summarises five aspects for Afghan health problems in Iran.
1) Non-communicable disorders: According to the reports published in 2012 [12], the most frequent non-communicable reasons for Afghan referrals to healthcare centres are ophthalmic disorders in 23.7%, different types of malignancies in 13.3%, nephropathies in 11.0%, ischaemic heart diseases in 10.4%, and perinatal disorders in 9.2%. The main aspect of referring in Afghans younger than 14 years was prenatal disorders, followed by ophthalmic disorders, and congenital abnormalities; while the main aspect for middle aged Afghans was ophthalmic diseases followed by nephropathies, malignancies, and coronary artery disease but for old Afghan population, it was ophthalmic disorders, followed by coronary artery disease and carcinomas.
2) Infectious disorders and other communicable diseases: Available data suggest that the Afghan population is greatly affected by infectious diseases, with reports of excess mortality from diarrhoeal disease, respiratory infections, and measles [19]. Compared to Iran, the overall prevalence of some communicable and infectious disorders including tuberculosis, Leishmaniasis and malaria is higher among Afghans than in Iranians [1]. This disproportion has led to higher prevalence of these infectious disorders in Afghan refugees and immigrants in Iran especially in Southeastern provinces. According to published reports on the prevalence of tuberculosis among Afghan refugees in 2009, the pooled proportion of Afghans with tuberculosis in Iran is 29% in the range of 4% to 55% [17,20-27]. Moreover, the prevalence of tuberculosis among Afghans is 40% in the range of 4% to 59% [28-30]. In this regard, the pooled proportion of Afghans with leishmaniasis is estimated as 7% [22,31,32], cholera as 8% [33-35], Crimean-Congo haemorrhagic fever as 25% [36,37], and hepatitis B as 14% [38]. Moreover, another study assessed the presence of HIV infection among Afghan immigrants using a rapid test in the field. HIV prevalence was 0.2%. It is suggested periodic HIV sero-surveillance for this population [39].
3) Food insecurity and malnutrition: Food insecurity is a common finding in Afghan refugees in Iran [40]. Food insecurity is a useful index of health and well-being because it is associated with poverty, ill-health, poor dietary intake and depressive disorders [41]. According to recent reports on food situation in Afghans [40,42], about 60% to 88% of Afghan households were food insecure in Iran that is determined by their low socioeconomic level as well as improper occupational state, low educational level, and illegal residential status. Moreover, significant prevalence of obesity in Afghan women (58%) and underweight/wasting status in Afghan children (11% to 16%) has been reported [43].
4) Low immunization coverage: An immunity gap has been recently reported in Afghan children when compared to Iranian children. In a published report in 2014 [16], the prevalence of partial immunization in Afghan children was about six fold to that of Iranian children (11.9% versus 2%). In addition, majority of Afghan children remain non-immunized. The reported discrepancy can explain considerable high prevalence of infectious diseases among Afghan refugees.
5) Psychological disorders: Recognising and appropriately treating mental health problems among immigrants in primary care poses a challenge because of differences in language and culture and because of specific stressors associated with migration and resettlement [44]. Studies showing a high prevalence of mental health problems such as Post Traumatic Stress Disorder (PTSD), depression and anxiety have convinced the government of Afghanistan to consider mental health among the top five priorities of the country’s health system. Although, there is still a long way to go to achieve significant recovery in population mental health given the limited access to mental health services and lack of trained staff particularly for psychiatric patients. A notable number of Afghan immigrants and refugees suffer from psychological disorders. Based on recent reports, about one-third of Afghans in Iran suffer from psychiatric problems [14]. Considerably, focusing Afghan refugees in camps showed 88.5% of Afghan refugees had mental disorders. Considering different components of mental health, revealed the prevalence of depression in 22.1%, anxiety in 39.3%, psychosomatic problem in 48.9%, and social dysfunction in 80.1% of them. In addition to consequences of war as a major determinant for mental disorders especially post traumatic stress disorder in this population, lower ages at migration time, unemployment status, higher number of households, and history of chronic diseases were other indicators of mental diseases [13].
Health Services
A healthcare system in refugee population should provide easy access to different levels of care, including referral services; and combine both curative and preventive services [45]. UNHCR support efforts of Ministry of Health in providing PHC services to all refugees, including vaccinations, antenatal care, maternal and child health, and family planning. UNHCR joint interventions with partners include medical referral, harm reduction, Sexual Gender-Based Violence (SGBV) prevention, and community-based rehabilitation. UNHCR assistance contributes to the construction and rehabilitation of health centers, payment of health personnel, training of community health workers, procurement of medicine and equipment [46].
Access to Health Services
Refugee operation in Iran is completely managed by government through Ministry of Interior, Ministry of Health and Medical Education and Ministry of Education. Iran prefer to preserve the authority of refugee’s performance for government due to national security matter and continue to work with UNHCR as the main partner. Other UN agencies including WFPA and UNODC. Furthermore, there are few national NGOs and international organizations that handle some parts of refugees operation in Iran. Government through Bureau of Aliens and Foreign Immigrants Affairs (BAFIA), Ministry of Interior, closely observes their performances, defines their field of action and their boundaries. UNHCR continues funding a range of NGOs as well as Organizations delivering health services through: MAHAK (supports refugee children suffering from cancer); Society for Recovery Support (SRS); Chain of Hope (CoH); Association for Protection of Refugee Women and Children (HAMI); Organization for Defending Victims of Violence (ODVV); State Welfare Organization of Iran (SWO) [47]. Whereas, public health relevant programs like vaccination, family-planning services are free, Afghan women do not receive free prenatal care, as do Iranian women. Other barriers to healthcare services for immigrants can result from lack of insurance or from delays of treatment. Another barrier to healthcare services and health education results from cultural problems and language barriers [48].
Primary Healthcare (PHC)
Afghans who are registered as refugees with the UNHCR receive specific health benefits. In 2010, this group was reported to have access to primary health services similar to those available to Iranian citizens. UNHCR continues its agreement with the Ministry of Health and Medical Education to provide PHC services to refugees, consisting of vaccinations, antenatal care, maternal and child health, and family planning, mostly in 15 settlements and 30 urban locations with a high density of refugee population. UNHCR assistance contributes to the construction and rehabilitation of health centers, payment of health personnel (inclusive of Afghan community health workers), training of community health workers, procurement of medicine and equipment. It is documented all vulnerable women of reproductive age and refugee students residing in settlements received sanitary materials and hygiene services [49], although unmet needs including:
Nearly 12,000 vulnerable refugees could not access to secondary healthcare services.
Victims of sexual and gender-based violence, female headed households and the elderly.
Some 2,500 refugees living with disabilities were excluded from community-based rehabilitation projects.
The protection needs of some 7,000 refugees could not be addressed, affecting child labourers, unaccompanied children,
A total of 20,000 vulnerable refugee women of reproductive age living in urban areas could not be provided with sanitary kits [50].
Health Insurance Scheme (HISE)
An arrangement with an insurance company enabled close to 40% of the registered refugee population to enjoy insurance coverage for secondary and tertiary health services. More than 40,000 extremely vulnerable refugees received financial support for their medical bills from UNHCR and the insurance company [46]. After the successful implementation of HISE-II in 2012-2013 which covered 209,714 vulnerable refugees, including 1,112 refugees with five recognised special diseases (thalassaemia, haemophilia, renal failure, cancer and multiple sclerosis), the new phase HISE-III was launched in September 2013 covering 220,200 vulnerable refugees including 2,000 refugees with special diseases. Under HISE-III scheme, the annual premiums are covered by UNHCR. The premium level and the ceilings for reimbursement of medical costs remain the same as HISE-II [50].
Discussion
In summary, migratory and asylum movement of the Afghans to Iran imposes both financial and health problems on Iran government. In consequence of low socioeconomic status, poor health condition, improper dietary behaviours, and lack of proper immunization coverage, high incidence of physical and mental disorders is expected in Afghan immigrants in Iran which led to high economic burden and healthcare issues. Afghan refugees are a potentially high risk group, and our finding suggests a need for more monitoring of their health. Because the evidence is limited, research is needed to develop and evaluate healthcare strategies for promoting health that respond to the increasing diversity of Afghan immigrants in Iran.
Conclusion
The present study identified issues related to Afghan health status in Iran. From the material we have analysed, we can conclude that it is imperative to combat the high numbers of diseases among immigrants in Iran while simultaneously modifying the public image of immigrants as a health and social service threat to Iran. These results are ambiguous and deserve further enquiry. Questions still remain regarding the regulation of access to healthcare services, existence of barriers, and measures which should be implemented to secure access to healthcare services.
Limitation
Limitation of this study was that present study was conducted using a limited number of databases, thus leaving out possible other literature sources that can help to provide a more accurate picture of Afghan immigrants health in Iran.