An Adult with Bowel Sounds in the Chest
Karanam Gowrinath1, Manam Gayatri2
1 Senior Consultant, Department of Pulmonary Medicine, Apollo Speciality Hospital, Nellore, Andhra Pradesh, India.
2 Consultant, Department of Radiology and Imaging Sciences, Apollo Speciality Hospital, Nellore, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Karanam Gowrinath, House no.103, Bhavani Park Centra, 9th Street, Ramji Nagar, Nellore-524002, Andhra Pradesh, India.
E-mail: drkgowrinath@gmail.com
Eventration, Flouroscopy, Plication, Ultrasound
A 53-year-old male, non-smoker was admitted for cough, breathlessness, throat pain and difficulty in swallowing of one week duration. Breathlessness was more during eating and on lying down. There was no history of birth trauma. In 2010, patient met with an accident while travelling in a bus and sustained head injury but recovered quickly with medical treatment. In 2014, he was admitted for respiratory tract infection and left Diaphragmatic Eventration (DE) was detected through computed tomography of chest.
Patient remained asymptomatic after discharge till one week back. Physical examination findings were not remarkable. Chest examination showed fullness of lower left hemithorax and auscultation revealed bowel sounds in the left infraaxillary and infrascapular areas. Other systems were clinically normal. Blood examination was significant for leucocytosis. A postero-anterior and left lateral chest radiograph showed elevated left hemidiaphragm with underneath bowel loops.
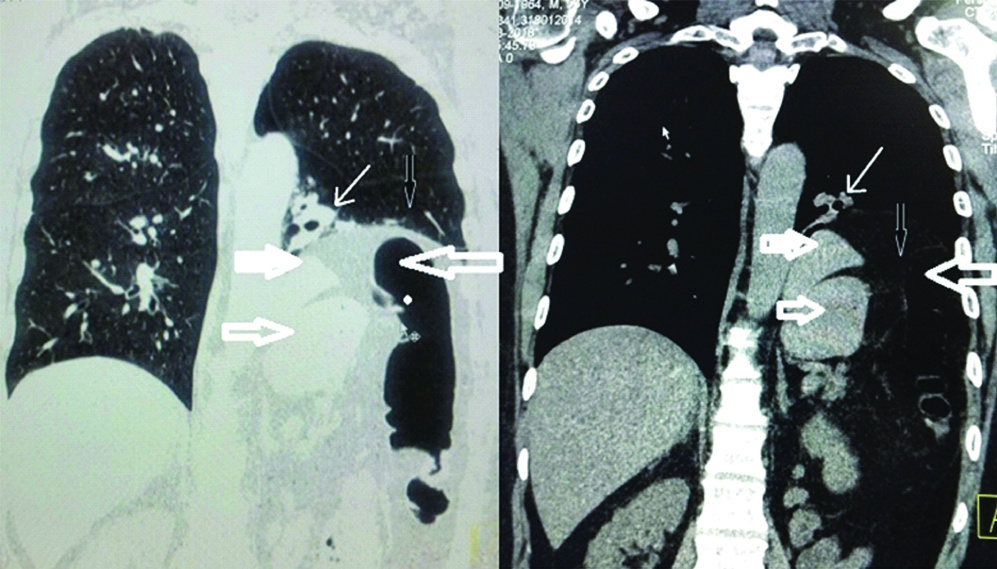
The Contrast-Enhanced Computed Tomography (CECT) scan of chest [Table/Fig-1] done four years back showed thin and elevated left hemidiaphragm, stomach, spleen, splenic flexure and colon. The latest Computed Tomography (CT) of chest [Table/Fig-2] done after admission also showed similar findings of thinned out left hemidiaphragm, stomach, spleen, splenic flexure and colon underneath it with sub-segmental atelectasis of lower lobe as an additional finding. Ultrasound examination showed uniformly elevated left hemidiaphragm with faintly appreciated respiratory phase movements and a single right renal cyst (23×18 mm) as an incidental finding. A diagnosis of left complete DE with acute bronchitis was made.
Coronal section of CECT scan of chest showing stomach (single arrow), spleen (thick white arrow), splenic flexure and colon (bigger arrows) below the elevated and thin left hemidiaphragm (black arrow).

Coronal section of latest CT scan of chest showing subsegmental atelectasis of left posterior basal segment (thin white arrow), stomach (single arrow), spleen (thick white arrow and splenic flexure with colon (bigger arrow) below the elevated left hemidiaphragm (black arrow).
Patient responded well to medical treatment for his respiratory infection which included intravenous cefepime (1 gm twice a day) for five days. After recovery, he was discharged and referred to cardiothoracic surgeon for surgical management. Patient remained asymptomatic and waiting for surgery at the end of five months follow up.
Discussion
The generally accepted definition of DE is “abnormally high or elevated position of one leaf of the intact diaphragm as a result of paralysis, aplasia or atrophy of varying degrees of muscle fibres. The unbroken continuity distinguishes it from diaphragmatic hernia” [1]. DE may manifest at any age and males are more often affected. True DE is a congenital anomaly resulting from incomplete development of muscular portion of part or total hemidiaphragm which becomes a thin layer of connective tissue and few scattered muscle fibres covered with pleura and peritoneum on either side [2]. In a study of DE among children, 17.5% had associated congenital malformations; hypoplasia of lung being the commonest followed by congenital heart disease [3].
Symptomatic DE is rare in adults and left hemidiaphragm is most often affected. Complete DE is detected more often in the left than in the right hemidiaphragm. Acquired eventration may be idiopathic or as a result of dysfunction of phrenic nerve as a consequence of spread of inflammation or neoplasm from adjacent area, trauma during birth or later including surgery [4]. In the present case, patient was born through normal delivery and never had respiratory problem till four years back. Whether, left DE was related to sudden jerky movements, experienced by the patient during bus accident eight years ago or not, could not be verified as patient denied direct chest trauma and did not preserve medical records including chest radiographs. Elevation caused by paralysis or weakness typically involves an entire hemidiaphragm whereas elevation secondary to eventration involves only a portion of a hemidiaphragm and pulmonary function testing may show restrictive defect [5]. In the present case, patient had complete eventration of left hemidiaphram and spirometry showed mild restrictive ventilatory defect. The normal diaphragm acts as a partition between the thorax and abdomen. But thin and weakened musculature of eventrated hemidiaphragm can no longer act as mechanical barrier and is displaced upwards resulting in protrusion of abdominal viscera into thoracic cavity. The main symptoms of DE are exertional dyspnoea and orthopnoea [6]. In the present case, patient presented with exertional breathlessness, orthopnoea along with throat pain and dysphagia.
Clinical diagnosis of eventration is not possible and some cases may have fullness of lower chest on the affected side, diminished or absent breath sounds and presence of bowel sounds in the chest [7] and our patient had all these clinical findings which may also be seen in diaphragmatic hernia but CT scan of chest can exclude diaphragmatic hernia. In an earlier published report, an adult case of left DE who had chronic respiratory symptoms presented with bowel sounds in the left hemithorax and the diagnosis was made only at surgery [8]. In another report, an adult case of left DE presented with 2 year history of breathlessness with peristaltic sounds in left hemithorax and showed paradoxical movement during fluoroscopic sniff test [9].
Flouroscopic sniff test is useful to document immobility or paradoxical movement of paralysed hemidiaphragm. The ultrasound technique has emerged as potential alternative for evaluation of diaphragmatic movement as it is more sensitive than fluoroscopy, can directly quantify diaphragmatic movement without any ionizing radiation and portable [10]. The eventrated hemidiaphragm may show little or no movement or even paradoxical movement. In our patient, thoracic ultrasound showed little diaphragmatic movement during inspiration. Sometimes total eventration of hemidiaphragm cannot be differentiated from diaphragmatic paralysis but a typical case of DE will not have any adjacent area of atelectasis [11]. Our case showed subsegmental plate like atelectasis in the posterior basal segment adjacent to elevated left hemidiaphragm when compared to previous CT scan of chest done four years back.
A symptomatic DE is treated surgically with diaphragmatic plication usually through posterolateral thoracotomy [12]. Minimally invasive techniques like VATS or laparoscopic diaphragmatic plication have proved to be effective alternative to open thoracotomy approach [13]. In the present case, there was recurrence of respiratory tract infection after a symptom free period of four years and stomach, colon were in the thoracic cavity. We, advised the patient to undergo surgery to avoid potentioal life threatening complications like gastric volvulus, intestinal obstruction, etc., [14,15].
Conclusion
Complete left DE is rare in adults and respiratory symptoms may recur even after years of symptom free period. Bowel sounds may be heard due to DE with protruded bowel loops during auscultation of chest. Thoracic ultrasound or CT scan can confirm DE and exclude conditions with similar clinical presentation like Bochdalek’s hernia.
[1]. Bisgard JD, Congenital eventration of the diaphragmJ Thorac Surg 1947 16:481-91. [Google Scholar]
[2]. Deslauriers J, Eventration of the diaphragmChest Surg Clin North Am 1988 8:315-30. [Google Scholar]
[3]. Wu S, Zang N, Zhu J, Pan Z, Wu C, Congenital diaphragmatic eventration in children: 12 years experience with 177 cases in a single institutionJ Pediatr Surg 2015 50:1088-92.10.1016/j.jpedsurg.2014.09.05525783408 [Google Scholar] [CrossRef] [PubMed]
[4]. Gupta V, Gupta P, Chandra A, Diaphragmatic eventration complicated by gastric volvulus with perforationSouth Afr J Surg 2012 50:90-91.10.7196/sajs.1043 [Google Scholar] [CrossRef]
[5]. Nason LK, Walker CM, McNeeley MF, Burivong W, Fligner CL, Godwin FJ, Imaging of the diaphragm: Anatomy and functionRadiographics 2012 32:E51-71.10.1148/rg.32211512722411950 [Google Scholar] [CrossRef] [PubMed]
[6]. Groth SS, Andrade RS, Diaphragmatic eventrationThorac Surg Clin 2009 19:511-19.10.1016/j.thorsurg.2009.08.00320112634 [Google Scholar] [CrossRef] [PubMed]
[7]. Thomas TV, Congenital eventration of the diaphragmAnn Thorac Surg 1970 10:180-92.10.1016/S0003-4975(10)65584-1 [Google Scholar] [CrossRef]
[8]. Shen C, Che G, Congenital eventration of hemidiaphragm in an adultAnn Thorac Surg 2012 94:e137-39.10.1016/j.athoracsur.2012.06.03223176954 [Google Scholar] [CrossRef] [PubMed]
[9]. Das A, Das SK, Sarkar A, Datta S, Rare association of eventration of left hemidiaphragm with ipsilateral thyroid agenesisIndian J Chest Dis Allied Sci 2012 54:131-33. [Google Scholar]
[10]. Houston JG, Fleet M, Cowan MD, MacMillan NC, Comparison of ultrasound and fluoroscopy in the assessment of suspected hemidiaphragmatic movement abnormalitiesClin Radiol 1995 50:95-98.10.1016/S0009-9260(05)82987-3 [Google Scholar] [CrossRef]
[11]. Roberts HC, Imaging of the diaphragmThorac Surg Clin 2009 19:431-50.10.1016/j.thorsurg.2009.08.00820112626 [Google Scholar] [CrossRef] [PubMed]
[12]. Ali Shah, Khan SA, Bilal A, Ahmad M, Muhammad G, Khan K, Eventration of diaphragm in adults: Eleven years experienceJ Ayub Med Coll Abbotabad 2014 26:459-62. [Google Scholar]
[13]. Podgaetz E, Diaz I, Andrade RS, To sink the lifted: Selection, technique and result of laparoscopic placation of paralysis or eventrationThorac Cardiovasc Surg 2016 64:631-40.10.1055/s-0035-157037226720705 [Google Scholar] [CrossRef] [PubMed]
[14]. Kanojia RP, Shanker R, Menon P, Rao KLN, Eventration with diaphragmatic perforation leading to secondary diaphragmatic hernia and intestinal obstructionHernia 2009 14:531-33.10.1007/s10029-009-0573-319826894 [Google Scholar] [CrossRef] [PubMed]
[15]. Yerrapragada S, Perumalla K, Daga S, Amirineni K, Diaphragmatic eventration with gastric volvulus: A surgical emergencyArch Int Surg 2015 5:109-12.10.4103/2278-9596.158826 [Google Scholar] [CrossRef]