A Rare Urinary Tract Infection by SalmonellaParatyphi A
Rohit Gupta1, KL Shobha2, Gowrish S Rao3
1 Postgraduate, Department of Microbiology, Kasturba Medical College, MAHE, Manipal, Karnataka, India.
2 Professor, Department of Microbiology, Melaka Manipal Medical College, MAHE, Manipal, Karnataka, India.
3 Selection Grade Lecturer, Department of Microbiology, Melaka Manipal Medical College, MAHE, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. KL Shobha, Department of Microbiology, Melaka Manipal Medical College, Manipal-576104, Karnataka, India.
E-mail: shobha.kl@manipal.edu
Urinary Tract Infection (UTI) caused by Salmonella is very rare and occurs mainly in immunocompromised patients, infants and those over 60 years of age. A 12-year-old patient admitted with history of fever, burning micturition and suprapubic abdominal pain, diagnosed with a rare variant of Salmonella from UTI which had showcased abnormal biochemical reaction unlike typical Salmonellaparatyphi A reactions. Here, we are communicating the rare H2S variant Salmonellaparatyphi A, causing UTI which caused clinical and microbiological confusion in the diagnosis. A high suspicion is required for adequate diagnosis and treatment when non-lactose fermenting colonies are seen in the culture plate.
H2S variant Salmonella spp, Non-lactose fermenting colonies, Paediatric age group
Case Report
A 12-year-old boy was admitted in the paediatric ward of the peripheral hospital with complaints of fever, pain abdomen and burning micturition for past 14 days. Fever was of high grade and was associated with chills followed by pain abdomen in suprapubic region which was insidious in nature and not associated with diarrhea and vomiting. No predisposing factor was present except a travel history to a gulf country two weeks before and returned to India a week before the presentation. None of the family members had similar features or any history of enteric fever.
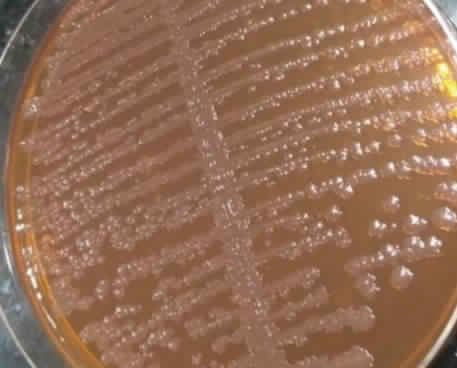
Haematological parameters were in normal range. Liver and renal parameters were also normal. Blood and urine samples were sent to Microbiology laboratory for culture and susceptibility testing. Urine sample was inoculated into blood agar and MacConkey’s agar following semi quantitative method. Blood agar had a count of >105 CFU/mL growth of gram negative bacteria and MacConkey’s agar showed non-lactose fermenting colonies [Table/Fig-1] Biochemical test showed abundant H2S production. Salmonellaparatyphi A was confirmed as Salmonella group by Matrix-Assisted Laser Desorption Ionization-Time of Flight (MALDI-ToF), Mass Spectrometry (MS) and with serotyping. Antimicrobial susceptibility testing was performed by VITEK 2 system (bioMerieux, Inc., Durham, NC). Organism was sensitive to ceftriaxone, ciprofloxacin and trimethoprim/sulphamethoxazole. Blood culture was sterile. Widal test did not show any significant titer done in the first week of admission. Salmonella isolate was reconfirmed by another urine sample to rule out contamination. Consent was not given for the stool sample. Patient was empirically started with Amoxicillin-Clavulanic acid but after antibiotic susceptibility testing report, it was changed to Ceftriaxone. Repeat urine sample culture after one week also showed Salmonellaparatyphi A with a count of >105 CFU/mL. No organism was seen in the urine culture plate collected after three weeks of therapy. Patient improved symptomatically and was discharged.
MacConkey’s agar showing non-lactose fermenting colonies.
Discussion
Salmonella bacteriuria occurs in <1% cases of enteric fever even in the endemic areas like India [1]. The patient had no previous history of enteric fever as urinary shedding of Salmonella may occur several months after infection in a carrier. Prolonged Salmonella shedding is seen in patients with abnormalities of urinary tract or in case of nephrolithiasis [2]. In this patient we could not find any abnormalities. Initially, enteric fever was suspected and blood culture and WIDAL were sought but it was of no contribution to the diagnosis. Isolation of Salmonella in urine with findings of >105 colony forming units/mL in the patient suggested more in favour of a localised infection or previous unnoticed asymptomatic blood infection, rather than a carrier state. According to Abdullah FE et al., 36.6 % were paratyphi A among the isolated Salmonella strains from urine [3]. Salmonellaparatyphi A, normally does not produce H2S and such H2S variants can be easily misdiagnosed as other non-fermenter like Citrobacter spp. and other Salmonella spp., leading to inappropriate antibiotic therapy [4]. As the identification was inconclusive, we had sent the isolate to reference Salmonella laboratory for typing but the strain was not typable. To the best of my knowledge this is one of the rarest cases of H2S producing Salmonellaparatyphi A possibly causing UTI. Probably he might have got the infection during his stay in gulf country where the Salmonellaparatyphi A infection is endemic [2].
Conclusion
We conclude that Salmonellaparatyphi A suspicion should also be there, whenever non-lactose fermenting gram negative organisms are grown in the culture medium and biochemical results are inconclusive. Identification of organism helps in better antibiotic stewardship.
[1]. Krishna S, Thunga R, Bairy I, Shobha K, Carrier status or Uro-pathogenic Salmonella paratyphi-A: urinary isolation of variant Salmonella paratyphi- A in a case of catastrophic systemic lupus erythematosusJournal of Case Reports 2015 5(1):75-78.10.17659/01.2015.0019 [Google Scholar] [CrossRef]
[2]. Al-Otaibi FE, Isolation of Salmonellaparatyphi A from a patient with nephrolithiasisSaudi Med J 2003 24(4):406-08. [Google Scholar]
[3]. Abdullah FE, Tanvir SB, Syed AZ, Haq MF, Shariq A, Ahmed S, Prevalence of Salmonella typhi and Paratyphi in urine cultures and their antibiotic sensitivity patterns in KarachiEuropean J Biotechnol Biosci 2015 3(3):35-38. [Google Scholar]
[4]. Jain S, Arora S, Saha R, Kaur I, Nalidixic acid resistant Salmonellaparatyphi A causing urinary tract infection in a patient with nephrolithiasis: case reportInt J Med Public Health 2011 1(4):45-46.10.5530/ijmedph.4.2011.9 [Google Scholar] [CrossRef]