Coronary artery disease is the most common, serious, life threatening illness in developed countries and has a rising prevalence rate in developing countries [1]. In India, it accounts for about 32% of the total deaths due to non-communicable diseases. Due to changing lifestyles, the overall burden of CAD is growing in India and is expected to be the leading cause of death and disability by 2015 [2]. CAD can be classified into single vessel, double vessel and triple vessel disease based on number of vessels involved and its severity can be graded based on Gensini scoring system. More than 95% of CAD is due to narrowing of coronary blood vessels due to atherosclerosis. This leads to decrease myocardial blood supply that in turn can be presented as stable angina, unstable angina, myocardial infarction and heart failure.
Conventional biochemical markers like Creatine Kinase MB isoenzyme (CK-MB), Troponin T (Trop T) etc., also have been used in diagnosis of CAD. But, these above mentioned parameters can help in detection only after infarction/ischaemia has occurred. Therefore, there is a need to identify a novel biochemical parameter which can detect such events before their occurrence. Natriuretic peptides family contains of three major peptides; Atrial Natriuretic Peptide (ANP), Brain Natriuretic Peptide (BNP), C-Type Natriuretic Peptide (CNP) that participate in cardiovascular and cardio-renal homeostasis [3]. Cardiac myocytes constitute the major source of BNP related peptides. The main stimulus for its synthesis and secretion is myocyte stretch. NT-proBNP is a well-established marker of heart failure and has been shown to be a good predictor of mortality in patients with acute coronary syndromes [3]. Thus, the present study compared the serum NT-proBNP levels in stable coronary artery patients and controls and with severity of CAD.
Materials and Methods
Study Population
The present case-control study was carried out after obtaining approval from the Institutional Ethics Committee of Kasturba Hospital, Manipal Academy of Higher Education, Manipal, from October 2012 to September 2014. A total of 86 study subjects (controls 36, cases 50) who presented to Department of Cardiology, Kasturba Hospital, who consented to participate were enrolled.
Sample Size Calculation
Anticipating a difference of 10 in the mean level of NT-proBNP with SD of 15 for a power of 80%, 95% confidence level and 40 subjects in each group. However, 50 participants were considered, in the study for case group.
Sample size calculation:
n=2{(Zα+Zβ) S}2/2 (d)2 = 45
Zα=value at specified confidence level
Zβ=value at specified power
S=pooled standard deviation of observations of 2 samples
d = clinically significant difference
Ethical clearance: IEC 225/2012, Monday 9th October 2012, Institutional Ethics Committee, Kasturba Hospital, Manipal.
Participants were enrolled based on following inclusion and exclusion criteria:
Inclusion Criteria
Cases: Subjects of both genders in the age group 30-75 years with stable CAD without left ventricular dysfunction diagnosed and graded by angiogram. Also, those who have stable CAD with co-existing diabetes/hypertension and on drugs like ACE inhibitors/ beta blockers/statins were included in the study.
Controls: Healthy individuals and those with co-existing diabetes/hypertension and on drugs like ACE inhibitors/beta blockers/statins in the age group of 30-75 years but not suffering from stable CAD were included in the study.
Exclusion Criteria
Cases: Patients of age <30 and >75 years, without any cardiac vessel narrowing, suffering from renal, liver disease, pulmonary artery hypertension, chronic obstructive pulmonary disease, congenital heart disease, valvular heart disease, unstable angina, acute myocardial infarction, old myocardial infarction, congestive heart failure, left ventricular dysfunction. Patients with history of smoking and alcoholism, on treatment with diuretics were excluded.
Controls: Subjects of age <30 and >75 years, suffering from renal, liver disease, pulmonary artery hypertension, chronic obstructive pulmonary disease, congenital heart disease, valvular heart disease, unstable angina, acute myocardial infarction, old myocardial infarction, congestive heart failure, stable coronary artery disease and left ventricular dysfunction. Subjects with history of smoking and alcohol, on treatment with diuretics were excluded.
Sample collection: Venous blood (4 mL) was drawn in red capped vacutainer. Serum was separated and stored at -70° C in eppendorf tubes.
Method of estimation of serum NT-proBNP: Enzyme linked immunosorbent assay, Uscn-Life-Science-Inc, SEA485Hu, 96 tests were used in the study.
Assessment of severity of coronary artery disease-Gensini scoring system: The Gensini scoring system is a valuable aid to estimate the severity of CAD according to angiographic findings. The calculation is based on the evaluation of number of stenotic segments along with their respective degrees of luminal narrowing and localisation within the coronary tree [4]. The Gensini score grades the narrowing of the lumen of the coronary artery as: 1 for ≤25% narrowing; 2 for 26-50% narrowing; 4 for 51-75% narrowing; 8 for 76-90% narrowing; 16 for 91- 99% narrowing; and 32 for total occlusion. This primary score is then multiplied by a factor that takes into account the importance of the position of the lesion in the coronary arterial tree, 5 for the left main coronary, 2.5 for proximal left anterior descending artery or proximal left circumflex artery and 1.5 for mid region, 1 for the distal left anterior descending artery and 1 for mid-distal region of the left circumflex artery or right coronary artery [5].
Statistical Analysis
The collected data were compiled and analysed using SPSS version 15.0 (SPSS South Asia Bangalore). Descriptive statistics was used to summarise the data. Spearman’s correlation coefficient was used. Associations were studied using chi-square test for categorical variables and Mann-Whitney test for the skewed continuous variables. Receiver Operating Characteristics curve (ROC) was used to identify optimal cut-off for NT-proBNP. Sensitivity, specificity, positive predictive value, negative predictive value of the test with area under the curve are reported. A forward Likelihood Multiple logistic regression was used to identify predictors of CAD. Adjusted Odds Ratio (OR) with 95% Confidence Interval (CI) was reported. A p-value<0.05 was considered to indicate the statistical significance.
Results
Among 86 study subjects, 59 were males and 27 were females. Males were more prone to suffer from stable CAD than females [Table/Fig-1].
Gender distribution among cases and controls.
| Gender | Controlsn (%) | Casesn (%) | Total |
|---|
| Males | 19 (52.77%) | 40 (80%) | 59 |
| Females | 17 (47.22%) | 10 (20%) | 27 |
| Total | 36 (100%) | 50 (100%) | 86 |
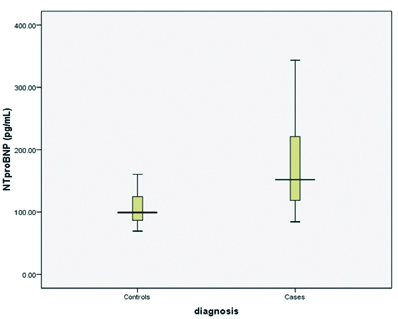
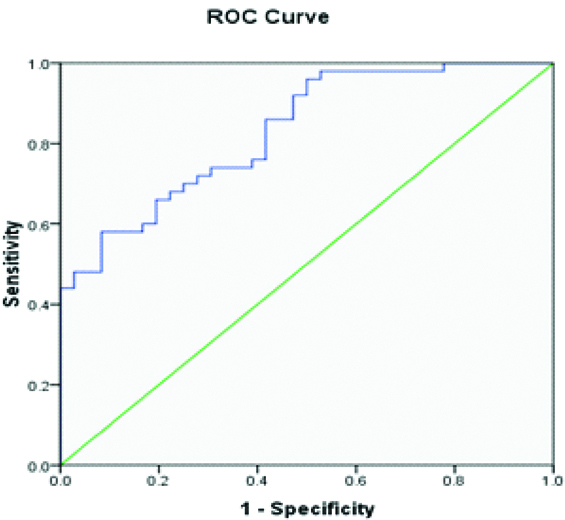
Above [Table/Fig-2] implies the total number of patients with single and double vessel disease were more than that of triple vessel disease group. Median level of serum NT-proBNP in controls was 99.31 pg/mL and median level of the same in cases was 151.9 pg/mL which was statistically significant (p=<0.001) [Table/Fig-3,4]. Significant increase in serum NT-proBNP among male and female cases compared to their controls are shown in [Table/Fig-5]. The mean Gensini score in cases were found to be 21.66 [Table/Fig-6]. Receiver Operating Characteristics (ROC) curve was used to identify the optimal cut-off and NT-proBNP levels ≥120.8 was found to be a predictor of stable CAD with 72% specificity and 72.2% sensitivity. Area under the curve was 83.1%. Positive predictor value was 77.4% and negative predictor value was 63.4% [Table/Fig-8]. Stepwise logistic regression was used to identify the predictor of stable CAD. NT-proBNP, age, and BMI was found to be predictors of stable CAD and use of statin as protective factor for stable CAD in the present study [Table/Fig-9].
Gender distribution among the subgroups of stable coronary artery disease without left ventricular dysfunction.
| Subgroups | Males | Females |
|---|
| Single vessel disease (n=22) | 15 (37.5%) | 7 (70%) |
| Double vessel disease (n=20) | 18 (45%) | 2 (20%) |
| Triple vessel disease (n=8) | 7 (17.5%) | 1 (10%) |
| Total | 40 (100%) | 10 (100%) |
Serum NT-proBNP levels in cases and controls.
| Serum NT-proBNP (pg/mL) | p-value* |
|---|
| Median | Interquartile range |
|---|
| Controls | 99.31 | (86.38, 125.54) | <0.001 |
| Cases | 151.9 | (117.74, 222.23) |
Serum NT-proBNP among cases and controls.
Gender wise comparison of serum NT-proBNP among controls and cases.
| Gender | ControlsMedian (IQR) | CasesMedian (IQR) | p-value |
|---|
| Females(n=27) | 89.53(85.03, 123.6) | 164.1(108.73, 221.52) | 0.006* |
| Males(n=59) | 117.19(87.83, 129.89) | 151.90(120.71, 238.93) | <0.001* |
Mann-Whitney U test
| Gensini score | Cases |
|---|
| Mean±SD | 21.66±29.09 |
| Range | 6-118 |
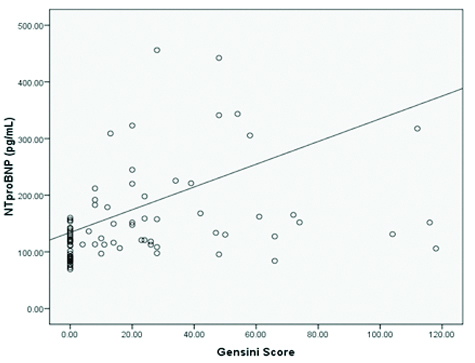
Correlation between Gensini score and serum NT-proBNP.
ROC curve of serum NT proBNP.
Stepwise Multiple logistic analysis.
| Predictors | Model Log Likelihood | Change in -2 Log Likelihood | Sig. of the change |
|---|
| NT proBNP | -39.97 | 15.99 | <0.0001 |
| Age | -34.10 | 4.26 | 0.039 |
| Statins | -35.78 | 7.61 | 0.006 |
| BMI | -44.52 | 25.10 | <0.0001 |
Discussion
N-terminal pro brain natriuretic peptide has been shown to be a powerful marker of systolic function. It has gained widespread acceptance as tool for the diagnosis of heart failure. It has been reported to identify patients with asymptomatic left ventricular dysfunction and also used to assess the severity of CAD [6-9].
The present study compared serum NT-proBNP in severity of stable CAD in subjects without left ventricular dysfunction. Among the cases, males (n=40) had higher preponderance over females (n=10) [Table/Fig-1] which was in consistency with many other studies [10,11].
The present study found that, the total number of patients with single and double vessel disease were more than that of triple vessel disease group [Table/Fig-2].
Serum NT-proBNP was significantly increased in cases as compared to controls [Table/Fig-3,4]. When serum NT-proBNP was compared based on gender, it had significant role in stable CAD development in both genders [Table/Fig-5].
Similar finding was observed in another study by Palazzuoli A et al., in subjects with non-ST segment elevation myocardial infarction [12]. They demonstrated that BNP also correlated with extent and severity of myocardial ischaemia. The present study observed that serum NT-proBNP had significant role in stable CAD development in both genders.
The mean Gensini score in cases were found to be 21.66 [Table/Fig-6]. We observed statistically significant weak positive correlation between serum NT-proBNP and Gensini score further substantiating its role in predicting severity of stable CAD [Table/Fig-7]. Even though the p-value was significant the correlation coefficient was 0.263, this may be due to small stable CAD size. Studies by Yesil M et al., Ndrepepa G et al., and Sahinarslan A et al., have also revealed that serum NT-proBNP correlated with CAD severity assessed by angiography [13-15].
The present study found out optimal cut off for serum NT-proBNP for predicting the CAD to be 120.8 pg/mL [Table/Fig-8]. Both modifiable and nonmodifiable factors affect the risk of developing CAD. In the present study along with increased serum NT-proBNP levels, other risk factors like age, body mass index played important predictors for developing the atherosclerosis resulting in CAD and use of statins were found to be protective factor in stable CAD [Table/Fig-9].
Limitation
We excluded four samples due to hemolysis (two samples) and serum NTproBNP value more than 99th percentile (two samples), thus sample size in controls reduced to 36. The number of males and females were not equally distributed in the study. These study subjects did not represent the whole population.
Conclusion
The serum NT-proBNP is elevated in patients with stable coronary artery disease without left ventricular dysfunction and it has close correlation with the severity of CAD. Thus NT-proBNP may be a valuable tool to predict the stable CAD and its severity. Thus in future it can be used as screening test.
Mann-Whitney U test