Second Degree Mobitz Type 1 Block in Dengue Haemorrhagic Fever: A Rare Manifestation
Harpreet Singh1, Gagan Deep Sukhija2, Saroj Bala3, Ruchi4, Harveen Sodhi5
1 Senior Professor, Department of General Medicine, Pandit Bhagwat Dayal Sharma, PGIMS, Rohtak, Haryana, India.
2 Senior Resident, Department of General Medicine, NC Medical College and Hospital, Karnal, Haryana, India.
3 Senior Resident, Department of General Medicine, Pandit Bhagwat Dayal Sharma, PGIMS, Rohtak, Haryana, India.
4 Senior Resident, Department of General Medicine, Kalpana Chawla Medical College, Karnal, Rohtak, Haryana, India.
5 Senior Resident, Department of Pediatrics, Kalpana Chawla Medical College, Karnal, Karnal, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Gagan Deep Sukhija, 529-A, Model Town, Near Parnami Mandir, Karnal, Haryana-132001, India.
E-mail: gagan43@gmail.com
Dengue is an arboviral disease caused by a Flavivirus. It is spread by the bite of Aedes aegypti mosquito. Spectrum of this disease ranges from mild self-limiting fever to potentially fatal severe multiorgan dysfunction with shock. Cardiac manifestations of dengue are uncommon but rhythm disturbances in the form of ventricular ectopics and different types of blocks have been reported with dengue haemorrhagic fever in the literature. Here, we present a case report of a young lady who developed 2nd degree Mobitz type I block during the de-fervescence stage of infection.
Arrhythmia, Atypical complications, Dengue
Case Report
A 25-year-old female presented to emergency with high grade fever (>103oF) since 4 days along with petechial rashes and pain in abdomen. There was no history of loose stools, syncopal attacks or palpitations. Past history was not significant.
On examination, patient was conscious, oriented and afebrile. Her fever grade had naturally decreased in 4 days duration and she was afebrile when she presented to us at the hospital. Her blood pressure was 130/80 mmHg and pulse rate was 60/min. Her face was plethoric and erythematous rashes were present predominantly over the trunk. There was tender hepatomegaly and multiple petechial rashes were present predominantly over bilateral lower legs. Cardiovascular and respiratory system examination were unremarkable.
On laboratory examination, her haemoglobin was increased to 16.2 gm%. Total leukocyte count was low (2.5×109/L) and there was thrombocytopenia (60×109/L). Liver function tests were deranged with SGOT/SGPT levels of 332/207 IU/L. Serum electrolytes and her cardiac enzymes (cpk-mb) were normal.
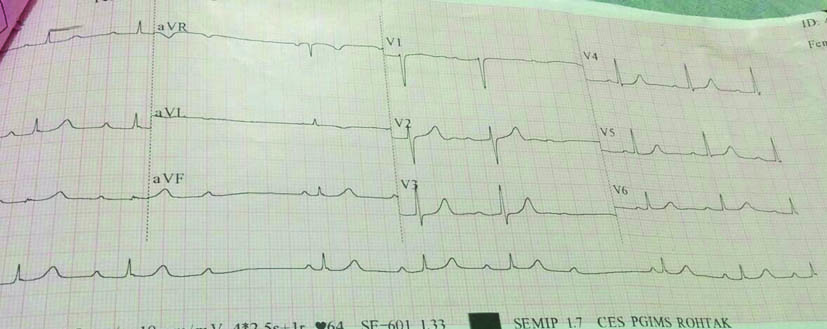
Malaria antigen card test was negative. Dengue NS1Ag was positive. Chest X-ray was normal while ultrasound abdomen revealed mild gall bladder oedema. Electrocardiogram showed 2nd degree Mobitz type I block i.e., Wenckebach phenomenon [Table/Fig-1]. She was put on regular cardiac monitoring with intravenous fluid replacement. Echocardiography was planned but as her AV block was resolved after two days so it was not done.
Showing second degree Mobitz type 1 block.
Her platelet count improved to 120×109/L and SGOT/PT dropped to 113/65 IU/L over next two days and IgM for dengue was positive on 5th day of infection and she was discharged in stable condition.
Discussion
Dengue is caused by a mosquito-borne virus of the Flaviviridae family. It is transmitted by Aedes Aegypti mosquito which is also known as Tiger Mosquito. It is an endemic disease in India and can present with wide range of presentations. The usual presenting complaints are fever, rash, retro-orbital pain, headache, myalgia and arthralgia. Presentation like dengue haemorrhagic fever and dengue shock syndrome are seen in few of the total patients diagnosed with dengue fever [1,2]. Dengue fever on occasions also presents with atypical presentations which include like encephalitis, mono/poly neuropathies, gullian barre syndrome, meningitis, myelitis, hepatitis, pancreatitis, parotitis, haemolytic uremic syndrome, renal failure, myocarditis, conduction abnormalities, ARDS, rhabdomyolysis etc. Although myocarditis has been shown to be complicating dengue infection in some case reports, little is known about cardiac involvement as a whole in dengue virus infection [3]. Our patient had evidence of hepatic involvement in form of raised liver enzymes and tender hepatomegaly along with rhythm disturbances diagnosed on the ECG, both of which were self limiting and improved with supportive treatment.
The cardiac involvement is generally diagnosed clinically and by electrocardiography as endomyocardial biopsy is rarely possible. Its manifestations can range from self-limiting rhythm disturbances to congestive heart failure to potential cardiogenic shock. The rhythm disturbances that have been reported include ventricular arrhythmias, ventricular ectopics, atrial fibrillation and varying degrees of heart blocks [3]. Type I Mobitz type of block as was in the present case is rarely reported in literature. Two cases of Type I mobitz were reported by Khongphatthallayothin A et al., [4]. The precise underlying mechanism for these type of rhythm disturbances are not known but various mechanisms are postulated. One of these is that in response to viral infection the immune system responds by making a lot of cytokines which is known as “cytokine storm”. These cytokines cause inflammation of myocardium which can trigger any sort of arrhythmias of the heart. Other mechanisms include autonomic dysfunctions, adenosine metabolism abnormalities and calcium and other electrolyte abnormalities in the myocardium [5,6]. Bleeding in the subendocardium close to the AV node can also lead to rhythm disturbances as noted by Bhamarapravati N et al. They noted bleeding in the septal region in the form of subendocardial haemorrhages in 47% of autopsies in cases of dengue haemorrhagic fever [7].
Conclusion
The present case of dengue (NS1Ag+ and IgM serology+) was detected to have 2nd degree AV block Type I Mobitz on routine ECG. Since the patients of dengue are likely to have autonomic failure so rhythm disturbances may aggravate the haemodynamic stability, so routine ECG is suggested to all suspected cases of dengue for better patient management.
[1]. Simmons CP, Farrar JJ, Nguyen VC, Wills B, DengueN Engl J Med 2012 366(15):1423-32.10.1056/NEJMra111026522494122 [Google Scholar] [CrossRef] [PubMed]
[2]. Deen JL, Harris E, Wills B, Balmaseda A, Hammond SN, Rocha C, The WHO dengue classification and case definitions: time for a reassessmentLancet 2006 368(9530):170-73.10.1016/S0140-6736(06)69006-5 [Google Scholar] [CrossRef]
[3]. Gulati S, Maheshwari A, Atypical manifestations of dengueTrop Med Int Health 2007 12(9):1087-95.10.1111/j.1365-3156.2007.01891.x17875019 [Google Scholar] [CrossRef] [PubMed]
[4]. Khongphatthallayothin A, Chotivitayatarakorn P, Somchit S, Mitprasart A, Sakolsattayadorn S, Thisyakorn C, Morbitz type I second degree AV block during recovery from dengue haemorrhagic feverSoutheast Asian J Trop Med Public Health 2000 31(4):642-45. [Google Scholar]
[5]. Salgado DM, Eltit JM, Mansfield K, Panqueba C, Castro D, Vega MR, Heart and skeletal muscle are targets of dengue virus infectionPediatr Infect Dis J 2010 29(3):238-42.10.1097/INF.0b013e3181bc3c5b20032806 [Google Scholar] [CrossRef] [PubMed]
[6]. Tisoncik JR, Korth MJ, Simmons CP, Farrar J, Martin TR, Katze MG, Into the eye of the cytokine storm. microbiology and molecular biology reviewsMMBR 2012 76(1):16-32.10.1128/MMBR.05015-1122390970 [Google Scholar] [CrossRef] [PubMed]
[7]. Bhamarapravati N, Tuchinda P, Boonyapaknavik V, Pathology of Thailand haemorrhagic fever: a study of 100 autopsy casesAnn Trop Med Parasitol 1967 61(4):500-10.10.1080/00034983.1967.116865195634140 [Google Scholar] [CrossRef] [PubMed]