Shoulder impingement syndrome is a disorder in which compression of the rotator cuff structures with the coracoacromial arch [1]. This sought of impingement occurs when there is a decrease in acromiohumeral space resulting in impingement syndrome. The SIS is also known as compressive tendinitis [2]. AHD is the distance between the inferolateral edge of acromion and superior margin of humeral head [3]. Literature review suggests positive correlation between decreased AHD and occurrence of SIS because decrement in the subacromial space is keystone causation for this disorder [4]. Disruption of physiological arthrokinematics is responsible for SIS pathology. Shoulder elevation causes physiological decrease in AHD however there is fine gap for classifying AHD as pathological. Repetitive overhead use causes cumulative rotator cuff trauma due to constant narrowing of AHD, which is common event for overhead athletes (volleyball, tennis, cricket, badminton, swimmers etc.,) [5]. Compressive tendinitis has worse prognosis if early detection is absent in athletes therefore, AHD can help guide clinician develop rational management plan for the patient. Measurement of AHD could be done by MRI, CT, ultrasound and X-ray. Amongst these RTUS offers non-invasive, radiation free, inexpensive method and highly valid measure for comparison (r>0.8) [6-8].
AHD of 11 mm and 5.7 mm has been found by RTUS at shoulder neutral and 90° abduction in previous studies [6]. Compression of the rotator cuff musculature in SIS athletes also causes gradual tendon attrition along with pain induced inhibition of the contractile component. Normally shoulder external rotator (infraspinatus) due to its large physiologic cross-sectional area, contributes a large percentage to torque and strength production during overhead movements.
Materials and Methods
This was a case-control test retest observational study. The study was performed in CPRS, Jamia Millia Islamia, New Delhi, India, from March 2016 to December 2017. Human Ethical Clearance Committee of the university gave permission for the research study. Afterwards informed consent was taken from all the participants. Power analysis was done for calculating sample size. The minimal ICC-value of 0.50 and maximal ICC-value of 0.90 (excellent) was selected, with an α error of 0.05 and power (1-β error) of 0.80, resulting in a minimal total sample size of 26 participants [10]. After performing standardised research canvassing in the university, overhead athletes and healthy individuals (control group) were screened for the study. The SIS athletes were confirmed clinically by following criteria where at least two out of five tests should be positive: a) positive Neer’s sign; b) positive Hawkins sign; c) positive Jobes sign; d) pain with apprehension test; e) positive relocation test [11]. Those with previous shoulder dislocation, Acromioclavicular (AC) joint pathology, prior surgery on the symptomatic side and positive drop arm test were excluded. The recruitment of control group was done by sending emails to university students. Subjects were included if they were in age group of 17-35 years, had no history of recent shoulder injury, fracture, surgical intervention, no history of neurological deficit and appendicular spondyloarthropathy. The exclusion criteria for control group included participation by subject in a sports involving overhead upper quadrant usage (more than once a week) [11]. The participants were divided into three groups namely SIS athlete, healthy athlete and control group as per presenting features. Ten were overhead athletes with SIS, eight were healthy overhead athletes and further eight constituted control group.
Procedure: The participants in three groups were tested for intra-rater test retest reliability at varied shoulder position in SIS group, cut-off point of AHD was determined for athletic groups and finally relationship of AHD and isometric shoulder external rotation along with AHD differences was examined on dominant side across three groups.
Reliability Analysis (RTUS): RTUS was done for each participant. AHD was measured with the help of radiologist (GE ultrasound modality, 7-12 MHz transducer head). Transducer head was placed in coronal plane to measure AHD. Imaging was obtained at three positions i.e., 0°, 45° and 60° abduction with the participants comfortably seated on chair [12]. For 0°, the arm was besides the body and the ulnar side of hand was comfortably resting on the thighs and thumbs pointing towards ceiling. The imaging for 45° and 60° shoulder abducted position was done by asking participants to hold the abducted position actively, elbow flexed to 90° and thumbs pointing upwards [13]. Strap belt fixed around elbow region helped in maintaining the desired angle and worked like check mechanism. To further ensure correct amount of abduction, goniometer was used for the measurement. The ultrasound head was positioned in coronal plane at the location at which the acromiohumeral distance was least [Table/Fig-1].
Participant position for ultrasound image at 45 degree shoulder abduction.

AHD is the distance between the lateral most acromial points to the humeral edge [14] [Table/Fig-2]. The test retest ultrasound measurements for AHD were done after two days from the initial measurement to examine intra rater reliability.
The tangential measurement of acromiohumeral distance by ultrasound imaging.

Isometric external rotation strength: For the isometric testing of the shoulder external rotation strength, Hand Held Dynamometer (HHD) Laffayette instruments) was used. The isometric shoulder external rotation strength was measured on dominant side across all three groups. The relationship of isometric strength was assessed to explore the impact of varying AHD on shoulder strength. The participants were asked to go into side lying position in such a manner that dominant arm was on top. The participants flexed their elbow to 90° and asked to perform external rotation with maintenance of prepositioning. HHD was placed on the dorsal surface of forearm near wrist joint and counter force applied [Table/Fig-3] [15]. The isometric contraction was performed for five seconds. Dominant shoulders were tested and pep talk was given to elicit maximal activity of the muscle [16-18]. The reading was measured in Newton-meter.
External rotation Isometric strength measurement by hand held dynamometer.

AHD cut-off point: The cut-off point calculation helps a clinician rationalise the result of the test and classify the participants into those with and without pathology. The AUC of the ROC curve was a prime determinant for sensitivity estimation (true positive cases) and specificity estimation (true negative). The cut-off point was determined by locating the point on the intersection of the imaginary line joining the top left and bottom left corner. The higher the sensitivity (closer to 1) better was its ability to detect true positive cases.
Statistical Analysis
Reliability was a measure which tests the consistency of deriving same or nearly similar result when measurements were taken on separate temporal frames. Intra rater reliability is calculated by measuring ICC value. The values >0.7 are considered to denote acceptable reliability. Standard Error of Measurement (SEM) was derived using equation: SEM=SD×√(1-ICC) where SD denotes Standard Deviation [19]. Minimum detectable change is the minimum amount of change in score or reading which was not due to error.
Minimum Detectable Change (MDC) is computed by using formula MDC=1.96×SEM×√2 [19].
The Bland altman plot was created to determine the level of agreement between the baseline test measurements and follow-up retest measurement. Limits of agreement were calculated by formula: mean difference ±1.96×SD [20]. One-way repeated measure ANOVA was used to compare the three groups’ differences. Post-hoc Bonferroni test is used as confirmatory test for the differences which are statistically significant. The relationship between shoulder isometric external rotation and AHD distance was measured by Pearson correlation coefficient. The correlation coefficient r measures the strength and direction of a linear relationship between two variables and the value of r is always between +1 and –1 values of r>0.5 indicate strong relationship [21]. SPSS version 21.0 (IBM Corporation, NY, USA) was used for statistical analysis. All p-values were two-tailed and significance taken at p<0.05.
Results
The mean age of the athlete group was 22.15±2 years and the normal individual control group had a mean age of 21.9±1.5 years [Table/Fig-4].
Characteristics of the participants.
| Variables | Normalindividuals(n=8) | Healthyathletes(n=8) | SIS(n=10) | p-value |
|---|
| Age (years) | 21.9±1.5 | 23.2±1.7 | 21.1±1.4 | >0.05 |
| Weight (kg) | 60.0±10.1 | 64.7±8.5 | 68.9±6.5 | >0.05 |
| Height (cm) | 165±8.5 | 175±7.5 | 173±7.2 | >0.05 |
| BMI (kg/m2) | 21.4±2.3 | 21.32±1.52 | 22.91±1.16 | >0.05 |
| Years of play (years) | -NA- | 4.2±1.2 | 4.6±1.6 | <0.05 |
| AHD (mm) ND | 10.90±0.65 | 12.08±0.62 | 11.23±0.51 | >0.05 |
| AHD (mm) D | 10.65±0.71 | 12.03±0.76 | 8.08±0.95 | <0.001 |
| Isometric ER ND | 86.20±2.48 | 100.50±3.20 | 81.25±4.09 | >0.05 |
| Isometric ER (D) | 83.63±2.66 | 104.63±3.77 | 68.89±6.44 | <0.001 |
Values were mean±SD; N: Number of participants; SIS: Shoulder impingement syndrome group; BMI: Body mass index; AHD: Acromiohumeral distance; ER: External rotation; ND: Non dominant side; D: Dominant
Descriptive characteristics regarding 26 participants was not found statistically significant (p>0.05) which refers that all participants had similar baseline characteristics [Table/Fig-4].
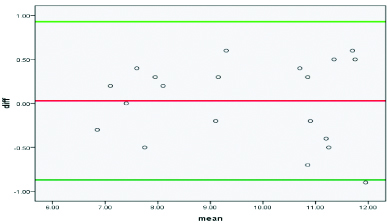
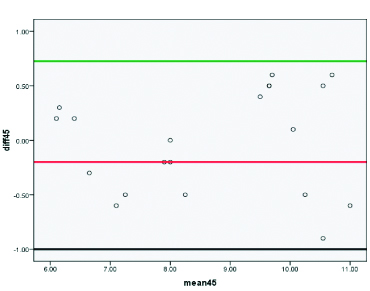
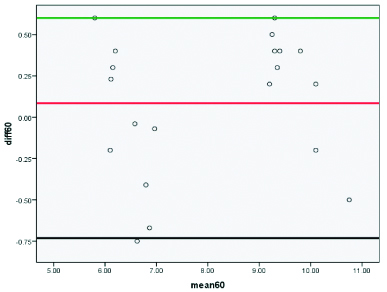
Intra rater reliability analysis: In the SIS, athlete group participants performed 0°, 45° and 60° of active shoulder abduction which yielded excellent reliability (ICC >0.90; 95% CI- 0.90-0.98) [Table/Fig-5a,b and c]. The corresponding MDC 95 for specified active abduction angle was calculated to be 0.98 mm, 0.94 mm and 0.83 mm respectively [Table/Fig-6].
Bland altman plots for acromiohumeral distance test retest reliability in shoulder impingement syndrome group at 0° (degrees) of shoulder abduction.
Note: X-axis denotes mean at test and retest measurements of AHD and Y-axis denotes the difference between test and retest measurements
Bland altman plots for acromiohumeral distance test retest reliability in shoulder impingement syndrome group at 45° (degrees) of shoulder abduction.
Note: X-axis denotes mean at test and retest measurements of AHD and Y-axis denotes the difference between test and retest measurements
Bland altman plots for AHD test retest reliability in shoulder impingement syndrome group at 60° (degrees) of shoulder abduction.
Note: X-axis denotes mean at test and retest measurements of AHD and Y-axis denotes the difference between test and retest measurements.
MDC95 for specified active abduction angle.
| Arm position (SIS) | Mean (SD), (mm) | SEM, (mm) | MDC95, (mm) | ICC (2,1) | 95% CI |
|---|
| 0° | 9.65 (1.78) | 0.356 | 0.98 | 0.96 | 0.92-0.98 |
| 45° | 8.66 (1.70) | 0.340 | 0.94 | 0.96 | 0.90-0.98 |
| 60° | 8.07 (1.76) | 0.304 | 0.83 | 0.97 | 0.92-0.98 |
SD: Standard deviation; SEM: Standard error of measurement; MDC95: Minimum detectable change with 95% confidence; CI: Confidence interval; ICC: Intra class coefficient (intra rater reliability)
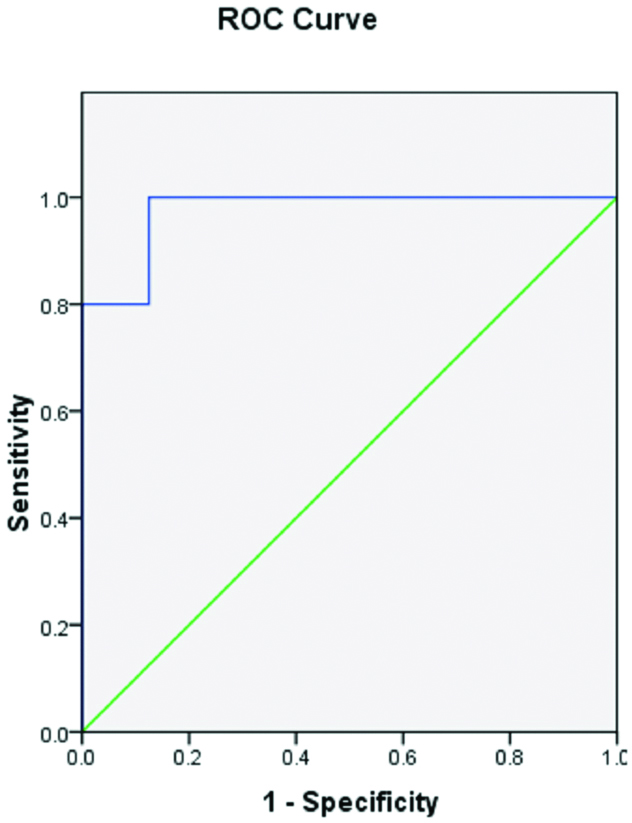
ROC curve was plotted to determine the appropriate cut-off point of the AHD distance in identifying the SIS pathology in athletic participants. The dominant side AUC was found to be 0.975 (p<0.001). The proportionate cut-off on dominant side of the athletic group was reported to be 10.20 mm (sensitivity 0.90, specificity-0.12; p<0.001) [Table/Fig-7,8]. Group differences in AHD at varied abduction angles One-way ANOVA was used for statistical analysis. The test of normality (shapiro-wilk test) revealed normal distribution in all groups (p>0.05). The present study findings at 0° abduction showed significant differences between all three groups (p<0.05) on dominant side. Besides this the analysis revealed larger AHD in healthy athletes (12.03±0.76 mm) and normal control individuals (10.65±0.71 mm) than SIS athletes (8.08±0.95 mm) [Table/Fig-9,10]. At 45° and 60° abduction on dominant side AHD in SIS athletes was significantly different from other two groups (p<0.05) [Table/Fig-11].
Correlational analysis between the isometric shoulder external rotation and AHD at 0° (degree).
| Cut-off value (mm) | Sensitivity | 1-specificity | Area under curve (AUC) | p-value | Pearson correlation coff. |
|---|
| 10.2 | 0.900 | 0.125 | 0.975 | <0.001 | 0.924 |
Receiver operating characteristic curve for cut-off value of AHD amongst athletes.
Comparison of AHD and ER among groups.
| Variables | SIS athletes | Healthy athletes | Control group | p-value |
|---|
| AHD | 8.08±0.95 | 12.03±0.76 | 10.65±0.71 | <0.001 |
| ER | 68.89±6.44 | 104.63±3.77 | 83.63±2.66 | <0.001 |
(one-way ANOVA); Values were mean±SD, SIS: Shoulder impingement syndrome group, AHD: Acromiohumeral distance; ER: External rotation; p-value significant at p<0.05
Post-hoc analysis of AHD and external rotation among the groups.
| Group | Mean±SD | p-value | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| SIS vs. Healthy athletes (D) | 8.08±0.95 vs. 12.03±0.76* | <0.001 | 4.97 | 2.93 |
| 68.89±6.44 vs. 104.63±3.77** | <0.001 | 41.58 | 29.89 |
| Normal athletes vs. Normal individuals (D) | 12.03±0.76 vs. 10.65±0.71* | <0.001 | 0.31 | 2.46 |
| 104.63±3.77 vs. 83.63±2.66** | <0.001 | 14.48 | 27.16 |
| SIS vs. Normal individuals (D) | 10.65±0.71 vs. 8.08±0.95* | <0.001 | 1.54 | 3.59 |
| 83.63±2.66 vs. 68.89±6.44** | <0.001 | 8.89 | 20.58 |
Bonferroni test: Values were mean±SD; SIS: Shoulder impingement syndrome group; *AHD: Acromiohumeral distance; **ER: External rotation; D: Dominant side; p-value significant at p<0.05
Post-hoc analysis of AHD among the groups (45° and 60° shoulder abduction).
| Group | Mean±SD | p-value | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| SIS vs. Healthy athletes (D) | 7.10±0.74 vs. 9.62±0.63* | <0.001 | 3.35 | 1.69 |
| 6.38±0.27 vs. 10.38±0.68** | <0.001 | 4.61 | 3.38 |
| Normal athletes vs. Control group (D) | 9.62±0.63 vs. 10.26±0.63* | >0.05 | 1.51 | 0.24 |
| 10.38±0.68 vs. 10.17±0.50** | >0.05 | 0.43 | 0.85 |
| SIS vs. Control group (D) | 7.10±0.74 vs. 10.26±0.63* | <0.001 | 2.32 | 3.99 |
| 6.38±0.27 vs. 10.17±0.50** | <0.001 | 3.17 | 4.39 |
Bonferroni test: Values were mean±SD; SIS: Shoulder impingement syndrome group; *AHD: Acromiohumeral distance at 45° abduction; **AHD: Acromiohumeral distance at 60° abduction D: Dominant side; p-value significant at p<0.05
Correlational analysis between AHD and isometric external rotation: The correlational analysis between the isometric shoulder external rotation and AHD at 0° (degree) yielded positive Pearson correlation coefficient 0.924 on dominant side (p<0.05) [Table/Fig-7].
Discussion
The reliability of ultrasound measurement for AHD has limited evidence when assessing the SIS athletes. Therefore this study aimed at determining the reliability, relationship between AHD and external rotation strength, diagnostic accuracy of RTUS and group differences in AHD at varied abduction angles. The intra rater reliability was examined and found to be excellent {ICC>0.90 (2,1), p<0.05} for all the test positions i.e., 0°, 45° and 60° in SIS athletes. These findings are in line with many of the studies which have also reported ICC(2,1) in the range of 0.92 to 0.98 [3,5,12,19]. In continuation with the work the MDC was calculated. MDC reflects the true change without error and it was calculated for all three positions in SIS athletes. The MDC was found to be 0.98 mm, 0.93 mm and 0.84 mm for the above mentioned three shoulder positions which is in accordance to the recent study [19]. However, some other studies have reported the MDC95 to be in range of 2.1-2.3 mm [5]. This difference can be attributed to variation in shoulder test position and the method used to hold the angled shoulder position.
In present study, the AHD findings showed significant difference (p<0.05) between three groups at 0° of abduction on the dominant shoulder side. This implicates that on the dominant side the AHD is significantly decreased in comparison to healthy athletes and the normal control. The present study findings were in line with studies performed recently which have also reported differences in AHD on dominant side [3,22].
The study reported that in SIS, the AHD at rest (0 degrees) was correlated with its reduction at all shoulder positions (rp 0.62-0.88), however, correlation was weak when AHD was measured at 110° (flexion, R2=0.09; abduction, R2=0.08) [23].
The mentioned findings can be explained by the decrement in inferomedial rotator cuff force vector. This force vector is required to offset the superior pull of the deltoid muscle. SIS and normal control participants have a weak or inactive inferior medial force vector which results in decreased AHD in contrast to inferomedial vector pull in healthy athletes.
During active abduction of shoulder to 45°, there was significant difference between SIS athlete/normal athletes and SIS/normal individuals (p<0.05). The results imply that as abduction increases, the rotator cuff muscles are not able to simultaneously inferior glide the humeral head with concomitant superior humeral rolling.
At 60° there was significant difference on the dominant side between the groups except that of normal athlete and normal individuals (p<0.001). The clinical rationale behind the above mentioned results was due to the lack of the inferomedial rotator cuff force vector. This force vector was required to offset the superior pull of the deltoid muscle. SIS and normal control participants have a weak or ineffective inferiormedial force vector which results in decreased AHD. Also, at 0° of abduction the normal athlete had a greater AHD than other two groups. This can also be possibly due to thicker and morphologically developed supraspinatus tendon and higher infero medial pull of the humeral head which increases AHD. When active shoulder abduction is initiated, scapula humeral rhythm with normal arthrokinematic comes into force. As per concave convex rule, the convex humeral head rolls superiorly and glides inferiorly. This helps to achieve higher degree of abduction without compressing the subacromial structures. The pathological condition disrupts the normal arthrokinematic due to rotator cuff shutdown which corroborates with our result in AHD. The present study found greater mean difference of 0.9 mm (45 degrees) and 0.59 mm (60 degrees). These findings were in contrast to findings of recent work which reported less reduction in AHD during first 45 degrees of abduction [20,24]. The reason behind the difference may be because of difference in subject population-normal athletic and non-athletic population.
ROC curve was also plotted and AUC was found to be 0.975 for dominant side in athletes groups. In addition we found AHD optimal cut-off value on dominant side<10.20 mm for the presence of SIS. Hence, participants with above mentioned cut-off value may suffer from SIS with a sensitivity of 0.900 and specificity of 0.125. The cut-off value in study done by previous study was found it be even higher i.e., 23.9 mm than present study. However, the sensitivity of the study is less than ours [3].
The reliability of ultrasound measurement for AHD also has limited evidence when assessing the SIS athletes. AHD is also strongly positively correlated with isometric external rotation strength of dominant shoulder in all three groups. This indicates that lower AHD results in lower isometric ER strength. This result also matches with the concept that lower AHD leads to increased compression of the rotator cuff musculature resulting in inhibition of contractile component, a portion of the rotator cuff musculature i.e., infraspinatus and teres minor have a pivotal action in inferiorly pulling the humeral head. The normal athletes (104.63±3.77 Nm) and normal individuals (83.63±2.66 Nm) had greater external rotation strength when compared with SIS athletes (68.89±6.44 Nm). This rationalises the previous findings that SIS causes a rotator cuff shutdown (inhibition) hence resulting in decreased ER isometric strength. Previous research findings also match our results of positive relationship of AHD with external rotation strength [9,12].
Limitation
First limitation of this study which needs to be considered is that SIS can also be due to intrinsic cause (tendon degeneration) which was not taken into account in this research. The second limitation was the smaller sample size in this study. Future researches can have stringent inclusion criteria for SIS athletic group.
Conclusion
This study concludes that RTUS is a reliable method for measurement of AHD. Healthy athletes have a greater AHD in comparison to SIS and control. Also, the greater AHD is associated with greater external rotation strength. Players with AHD of less than 10.65 mm are at a higher risk of developing SIS. Decrease in AHD induces higher loading of the rotator cuff tendons resulting in gradual tendon attrition. This study shows the importance of muscle strength evaluation as diagnostic and prognostic markers in players with SIS.
Values were mean±SD; N: Number of participants; SIS: Shoulder impingement syndrome group; BMI: Body mass index; AHD: Acromiohumeral distance; ER: External rotation; ND: Non dominant side; D: Dominant
SD: Standard deviation; SEM: Standard error of measurement; MDC95: Minimum detectable change with 95% confidence; CI: Confidence interval; ICC: Intra class coefficient (intra rater reliability)
(one-way ANOVA); Values were mean±SD, SIS: Shoulder impingement syndrome group, AHD: Acromiohumeral distance; ER: External rotation; p-value significant at p<0.05
Bonferroni test: Values were mean±SD; SIS: Shoulder impingement syndrome group; *AHD: Acromiohumeral distance; **ER: External rotation; D: Dominant side; p-value significant at p<0.05
Bonferroni test: Values were mean±SD; SIS: Shoulder impingement syndrome group; *AHD: Acromiohumeral distance at 45° abduction; **AHD: Acromiohumeral distance at 60° abduction D: Dominant side; p-value significant at p<0.05