Massive Lymphocytic Infiltration in the Uterus Mimicking Lymphoma-A Potential Diagnostic Challenge
Shailaja Shukla1, Shivali Sehgal2
1 Director Professor, Department of Pathology, Lady Hardinge Medical College, New Delhi, Delhi, India.
2 Assistant Professor, Department of Pathology and Blood Bank, Lady Hardinge Medical College, New Delhi, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shivali Sehgal, Assistant Professor, Department of Pathology, Lady Hardinge Medical College, New Delhi-110001, Delhi, India.
E-mail: shivalisehgal@gmail.com
Leiomyoma with lymphoid infiltration is an uncommon lesion which mimics lymphoma. Although, the polymorphous nature of the lymphoid infiltrate differentiates it from lymphoma, it may pose a diagnostic challenge at times. A 31-year-old female (Para 3, live issues 3) presented with menorrhagia. On sonography, a submucosal fibroid polyp measuring 2.5×2×1 cm arising from the anterior wall of the uterus was identified. Hysteroscopic polypectomy was carried out. Microscopy showed an exuberant lymphoid infiltrate in what appeared to be a leiomyoma. Numerous lymphoid follicles were observed, which on low magnification gave an impression of follicular lymphoma. Immunohistochemistry revealed their polymorphous character. It was diagnosed as leiomyoma with extensive lymphoid infiltration. It is important to know the range of histological alterations in leiomyomas, especially those with massive lymphoid infiltration since they simulate lymphoma clinically.
Immunohistochemistry, Lymphoid infiltration, Uterine leiomyoma
Case Report
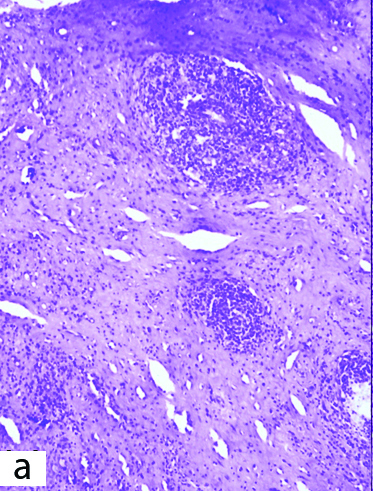
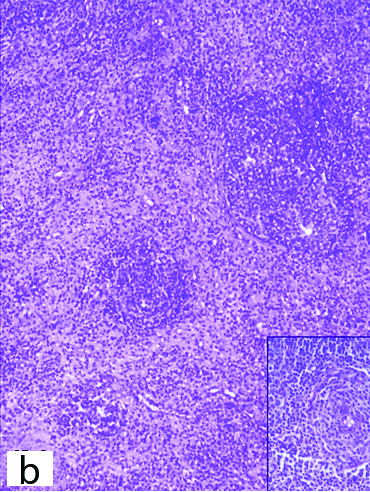
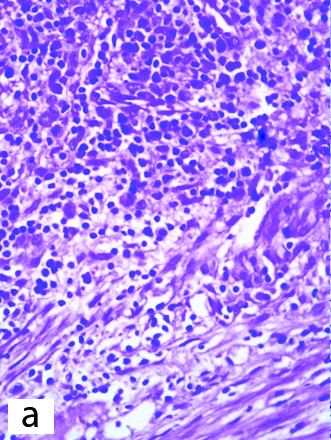
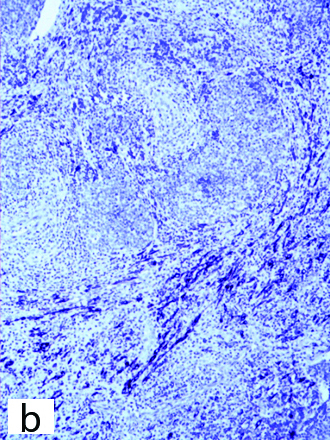
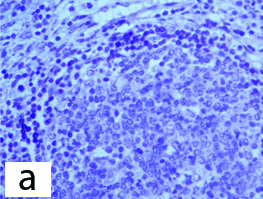
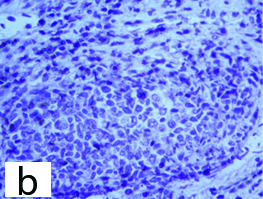
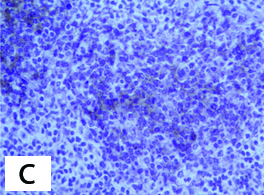
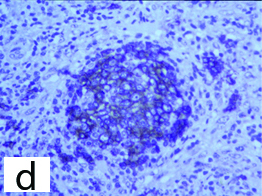
A 31-year-old female (Para 3, live issues 3) presented with menorrhagia. She had no history of treatment with Gonadotropin Releasing Hormone (GnRH) agonist or use of Intrauterine Contraceptive Device (IUCD). On sonography a submucosal fibroid polyp measuring 2.5×2×1 cm arising from the anterior wall of the uterus was identified. Hysteroscopic polypectomy was carried out and the tissue (multiple bits) was sent for histopathology. Microscopy showed an exuberant lymphoid infiltrate in what appeared to be a leiomyoma. Numerous lymphoid follicles were observed [Table/Fig-1a,b], which on low magnification gave an impression of follicular lymphoma. However, some of the follicles displayed prominent germinal centres pointing towards a benign pathology [Table/Fig-1b (inset)]. The infiltrate was polymorphous with presence of small mature lymphocytes, large lymphoid cells, histocytes and few plasma cells. There was no cellular atypia. The intervening stroma between the follicles was sclerotic at many places. The leiomyoma was almost completely replaced by the lymphoid infiltrate with only few residual smooth muscle fibres remaining at the periphery and the central portion showing hyalinisation [Table/Fig-2]. The overlying endometrium was in the proliferative phase. Immunohistochemistry (IHC) showed Smooth Muscle Actin (SMA) and desmin positivity [Table/Fig-2b] of spindle cells at the periphery of the mass as well as in the intervening stroma. BCL2 was positive in the marginal zone [Table/Fig-3a]. CD3 and CD5 were positive in the lymphoid cells in the interfollicular areas [Table/Fig-3b]. Majority of the infiltrating lymphocytes were B cells with few scattered T cells. CD19, CD10 [Table/Fig-3c] and CD20 [Table/Fig-3d] were positive in the follicles. There was a positive reaction for both kappa and lambda light chains. It was diagnosed as leiomyoma with lymphoid infiltration. Low grade lymphoma was ruled out on the basis of positivity with both kappa and lambda light chains on IHC. This requires confirmation with immunoglobin gene rearrangement studies, which was not performed due to non availability of the test in our centre. The postoperative course of the patient was uneventful and subsequently the patient was lost to follow-up.
Hyalinised leiomyoma with lymphoid infiltration (H&E; 100X).
Exuberant lymphoid infiltrate showing vague follicular pattern (H&E; 100X) with inset showing prominent germinal centres within lymphoid follicles (H&E; 100X).
Polymorphous lymphoid infiltrate splaying smooth muscle fibres (H&E; 400X).
The smooth muscle fibers are desmin positive (IHC; 100X).
BCL2 was positive in the marginal zone (IHC; 400X).
CD3 was positive in the lymphoid cells in the interfollicular areas (IHC; 400X).
CD10 was positive in the follicles (IHC; 400X).
CD20 was positive in the follicles (IHC; 400X).
Discussion
Leiomyoma with lymphoid infiltration is composed of a moderate to marked infiltrate of small lymphocytes, large lymphoid cells, histiocytes, variable number of plasma cells and rarely eosinophils. No increase in mitotic activity was seen. Reactive follicles may be observed. The infiltrate is mainly restricted to the leiomyoma and may rarely extend into the adjacent myometrium. On IHC, B cells (CD20 and CD79a positive) are seen within the follicles and T cells are present outside the follicles (CD3 and CD45RO positive) [1].
Leiomyoma with lymphoid infiltration is associated with the use of GnRH agonists, which help in the volume reduction of leiomyomata [1-4]. It may also occur secondary to use of IUCD. We present a case of a leiomyoma with lymphoid infiltration in a 31-year-old female who presented with abnormal uterine bleeding.
Ferry JA et al., reported 7 cases of leiomyoma with lymphoid infiltration which simulated lymphoma [5]. Zouari IB et al., reported a case of leiomyoma with lymphoid infiltration in which the intervening spindle cells were positive for smooth muscle markers and diffusely infiltrating lymphoid cells were of T cell phenotype [6].
The possible etiological factors are use of IUCDs, underlying autoimmune diseases, treatment with GnRH releasing hormone agonists/luteinizing hormone releasing hormone therapy all of which lead to an inflammatory response within the leiomyomata [1]. Bardsley V et al., described massive lymphoid infiltration in leiomyomata in patients on GnRH agonists [2]. Crow J et al., postulated that the alterations in the cell surface antigens elicit an immunological response causing deposition of inflammatory cells [3]. A specific human leukocyte antigen alteration or a viral infection could also be the cause of this entity [7]. In the present case, there was no history of treatment with GnRH agonists or use of IUCD.
The follow-up course of such cases is uneventful. The differential diagnosis includes uterine lymphoma, inflammatory pseudotumour and pyomyoma. Uterine lymphomas have a monomorphic infiltrate of cells which is not confined to the leiomyoma. Inflammatory pseudotumour produces a mass lesion within the uterus which is composed of fibroblasts and myofibroblasts and the infiltrate often has neutrophils. Pyomyoma is a leiomyoma with marked neutrophilic infiltrate and suppurative necrosis [1].
Conclusion
It is important to know the range of histological alterations in leiomyoma. Leiomyoma with lymphoid infiltration is an uncommon lesion which mimics lymphoma. Although, the polymorphous nature of the lymphoid infiltrate differentiates it from lymphoma, it may pose a diagnostic challenge at times, especially when the extensive infiltration almost completely obscures the underlying leiomyoma.
[1]. Kurman RJ, Ellenson LH, Ronnett BM, Blaustein’s Pathology of the female genital tract 2011 6th edNew YorkSpringer:1149-50.10.1007/978-1-4419-0489-8 [Google Scholar] [CrossRef]
[2]. Bardsley V, Cooper P, Peat DS, Massive lymphocytic infiltration of uterine leiomyomas associated with GnRH agonist treatmentHistopathol 1998 33:80-83.10.1046/j.1365-2559.1998.00451.x9726054 [Google Scholar] [CrossRef] [PubMed]
[3]. Crow J, Gardner RL, McSweeny G, Shaw RW, Morphological changes in uterine leiomyomas treated by GnRH agonist goserelinInt J Gynecol Pathol 1995 14:235-42.10.1097/00004347-199507000-000078600075 [Google Scholar] [CrossRef] [PubMed]
[4]. Lumsden MA, West CP, Thomas E, Coutts J, Hillier H, Thomas N, Treatment with the gonadotropin releasing hormone agonist goserelin before hysterectomy for uterine fibroidsBr J Obstet Gynecol 1994 301:438-42.10.1111/j.1471-0528.1994.tb11919.x8018618 [Google Scholar] [CrossRef] [PubMed]
[5]. Ferry JA, Harris NL, Scully RE, Uterine leiomyomas with lymphoid infiltration simulating lymphoma: A report of seven casesInt J Gynecol Pathol 1989 8:263-70.10.1097/00004347-198909000-000102670790 [Google Scholar] [CrossRef] [PubMed]
[6]. Zouari IB, Gouiaa N, Charfi S, Ellouze S, Chaari C, Kessentini M, Uterine leiomyoma with massive lymphoid infiltration: a case reportAnn Pathol 2011 31:98-101.10.1016/j.annpat.2010.12.00221601114 [Google Scholar] [CrossRef] [PubMed]
[7]. Botsis D, Koliopoulos C, Kondi-Pafitis A, Creatsas G, Frequency, histological, and immunohistochemical infiltration of leiomyomas of the uterus: an entity causing diagnostic difficultiesInt J Gynecol Pathol 2005 24:326-29.10.1097/01.pgp.0000172087.69384.3416175076 [Google Scholar] [CrossRef] [PubMed]