Vesicourachal Diverticulum: A Rare Entity
Partha Pratim Deb1, Amarendra Nath Sarkar2, Dawood Khan3, Supriya Basu4
1 RMO cum Clinical Tutor, Department of General Surgery, North Bengal Medical College, Siliguri, West Bengal, India.
2 Associate Professor, Department of General Surgery, North Bengal Medical College, Siliguri, West Bengal, India.
3 Postdoctoral MCh Resident, Department of Urology, R G Kar Medical College, Kolkata, West Bengal, India.
4 Professor, Department of Urology, R G Kar Medical College, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Partha Pratim Deb, A2, Block C, Shrikrishna Garden, Baikuntha Palli, Siliguri-734001, West Bengal, India.
E-mail: parthapratimdeb2@gmail.com
The urachus is a tubular embryonic structure connecting the allantois at the umbilicus to the bladder during development of foetus. It gets obliterated at 12th week of gestation and remains as a fibrous cord like structure extending from the umbilicus to the dome of the bladder. Complete or partial failure of this process results in urachal anomalies. We are reporting a rare case of young lady presenting with features of dysuria and passage of jelly like material in urine which was subsequently diagnosed as vesicourachal diverticulum by cross sectional imaging, cystoscopy and managed with minimally invasive surgical excision.
Dysuria, Urachus, Urachal anomalies, Vesicourachal diverticulum
Introduction
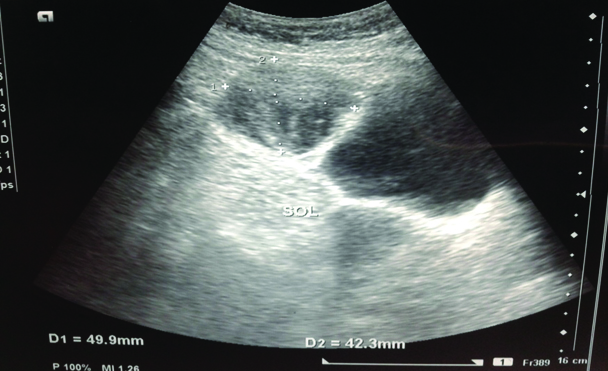
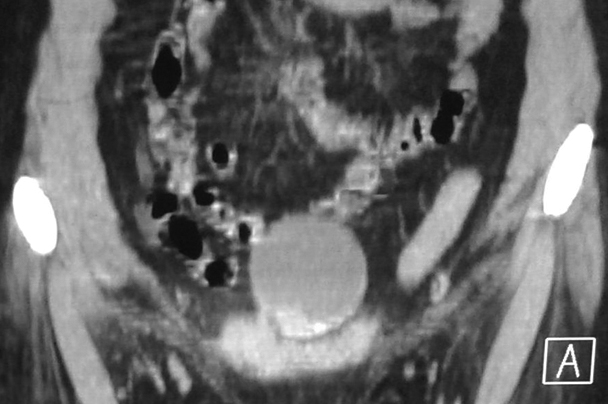
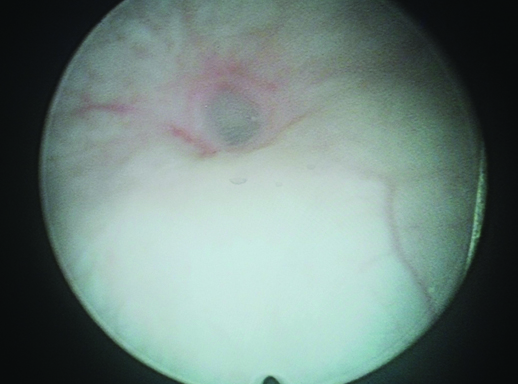
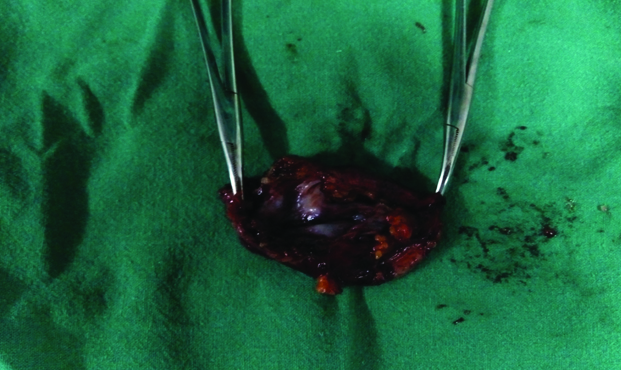
A 40-year-old female presented with dysuria and passage of jelly like material with urine for the last three months. She was haemodynamically stable and no lump was palpable abdominally. Her complete blood count was normal and her serum creatinine was normal denoting normal renal functioning status. Laboratory investigations revealed presence of 6-8 pus cells per high power field in the urine and urine culture was positive for Klebsiella species. Abdominal ultrasound revealed 4.9 x 4.2cm cystic Space Occupying Lesion (SOL) anterior to urinary bladder with debris inside with doubtful line of cleavage between SOL and outer wall of bladder [Table/Fig-1]. Contrast enhanced CT scan of abdomen showed a thick walled cyst of size 4.6x4.9x5.1 cm in front of urinary bladder with lower margin of the cyst inseparable from the bladder [Table/Fig-2]. Cystoscopy revealed a 4-5mm opening at the dome of bladder and the mucosa nearby was healthy [Table/Fig-3]. The diverticulum was explored laparoscopically, no attachment was found with the umbilicus and it was adherent to the omentum and gut. After dissecting the diverticulum from surrounding tissues, the communication between bladder and diverticulum were freed from adjacent structures. An endoloop was inserted through one of the ports and it was placed around the ostium of the communication like a noose. The endoloop was tightened and tied to close the communication. The diverticulum was severed from the urinary bladder and retrieved. Gross examination of the specimen showed a thick walled cyst filled with gelatinous fluid [Table/Fig-4]. Postoperative period was uneventful and the patient was discharged on the 5th postoperative day after removal of abdominal drain. It was histologically reported as a cyst lined by mucin secreting tall columnar epithelium with focal areas of low grade dysplasia and fibrocollagenous deposits on the wall suggestive of urachal remnant. Because of the histological evidence of dysplasia patient is kept under follow up with three monthly urinary cytology for malignant cells and cystoscopic examination.
USG image of cystic SOL of 4.9 x 4.2cm seen on the anterior aspect of the bladder with debris inside;
Coronal section of the CECT KUB showing a cyst of 4.6 x 4.9 x 5.1cm in front of bladder with some septation, focal calcification at lower end and thick content inside.
KUB: Kidney ureter bladder; SOL: Space-occupying lesion
Cytoscopic view of the diverticulum opening in the bladder.
Specimen of the vesicourachal diverticulum.
Discussion
The urachus is a tubular structure which remains patent during gestation but during foetal development it connects the allantois at the umbilicus to the dome of the bladder. The lumen normally gets obliterated at around 12th week of gestation and remains as a fibrous cord (median umbilical ligament) in the midline extending down to the dome of the bladder [1]. Failure of complete obliteration of the lumen results in urachal anomalies. They are twice as common in men than in women and are rarely observed clinically. They often occur in children and remain silent until complicated by infection.
There are four types of congenital urachal anomalies: patent urachus (50%, where there is communication with both umbilicus and bladder), urachal cyst (30%, where there is no communication with umbilicus or bladder), umbilical urachal sinus (15%, where there is patency at the umbilicus only) and vesicourachal diverticulum (3-5%, where there is communication with the bladder only) [2]. Vesicourachal diverticulum is a rare anomaly and constitutes approximately 3-5% of the urachal anomalies. Just over 10 cases have been reported in the literature [3-9]. They rarely cause problems because of presence of large opening in the bladder. Majority of patients with urachal abnormalities are asymptomatic. However, they may become symptomatic if these abnormalities are complicated by infection. They tend to be found in patients with chronic bladder outlet obstruction and may be complicated by UTI, intraurachal stone formation and an increased incidence of adenocarcinoma after puberty [10]. In present case, the presence of dysuria and abnormal passage of jelly like material with urine suggested the possibility of vesicourachal diverticulum.
Infection has been reported as the most common complication in urachal anomalies [11]. Most common organism cultured from infected urachal cyst was staphylococcus aureus and others were streptococcus, E. coli, citrobacter. In our patient, the sample of urine was sent for culture and sensitivity and the organism isolated was E. coli.
In the era of minimally invasive surgery, multiple reports of laparoscopic and more recently robotic assisted laparoscopic resection of urachal remnant in children have emerged. Visualization is excellent with a laparoscopic approach for the bladder but can be more challenging at the umbilicus if the ports are not carefully placed. In our case, as the bladder mucosa looked healthy at the opening of the diverticulum, so laparoscopic resection was performed. Also, there is controversy as to whether or not complete resection requires excision of the dome of the bladder [12-14]. If there is any doubt as to the extent of the lesion being excised, then one should be on the side of a more complete resection.
Conclusion
Vesicourachal diverticulum is a rare among the urachal anomalies. They may be symptomatic in the later part of life. They can be complicated by infection especially if their opening is narrow. Laparoscopic technique is a good and less invasive modality for the resection of these diverticula.
[1]. Park JM, Normal development of the urogenital systemCampbell Walsh Urology 2016 11th edPhiladelphiaElsevier [Google Scholar]
[2]. Blichert-Toft M, Nielsen OV, A congenital patent urachus and acquired variantsActa Chir Scand 1971 137:807-14. [Google Scholar]
[3]. Austin JC, Urachal anomalies in childrenPaediatric urology book 2015 1st edWiley Blackwell [Google Scholar]
[4]. Schnyder P, Candardjis G, Vesicourachal diverticulum: CT diagnosis of two adultsAm J Roentgenol 1981 137:1063-65.10.2214/ajr.137.5.10636794339 [Google Scholar] [CrossRef] [PubMed]
[5]. Jack BL, Jeffrey WM, Michael FE, Stephen LS, Spontaneous rupture of a vesicourachal diverticulum manifesting as acute abdominal painAcad Emerg Med 1996 3:1140-43.10.1111/j.1553-2712.1996.tb03375.x8959170 [Google Scholar] [CrossRef] [PubMed]
[6]. Ozbulbul NI, Dagli M, Akdo gan G, Olcer T, CT urography of a vesicourachal diverticulum containing calculiDiagn Interv Radiol 2010 16:56-58. [Google Scholar]
[7]. Patel PJ, Kolawole TM, Izzidien AI-Samarrai AY, Vesicourachal diverticulum in association with other urological anomaliesEur Urol 1987 13(6):417-18.10.1159/0004728383123243 [Google Scholar] [CrossRef] [PubMed]
[8]. Atalar MH, Salk I, Cetin A, Bozbiyik N, A rare case of vesicourachal diverticulum with calculus in a 24 year old manPol J Radiol 2016 81:301-02.10.12659/PJR.89612927429672 [Google Scholar] [CrossRef] [PubMed]
[9]. Yong EL, Ratnam SS, Prabhakaran K, Lee YS, Peritonitis following diagnostic laparoscopy due to injury to a vesicourachal diverticulumBJOG: An International Journal of Obstetrics & Gynaecology 1989 96(3):365-68.10.1111/j.1471-0528.1989.tb02399.x2523725 [Google Scholar] [CrossRef] [PubMed]
[10]. Yu JS, Kim KW, Lee HJ, Lee YJ, Yoom CS, Kim MJ, Urachal remnant diseases: spectrum of CT and US findingsRadiographics 2001 21:451-61.10.1148/radiographics.21.2.g01mr0245111259707 [Google Scholar] [CrossRef] [PubMed]
[11]. Al-Hindawi MK, Aman S, Benign noninfected urachal cyst in an adult: review of literature and a case reportBr. J Radiol 1992 65:313-16.10.1259/0007-1285-65-772-3131581788 [Google Scholar] [CrossRef] [PubMed]
[12]. Stone NN, Garden RJ, Weber H, Laparoscopic excision of a urachal cystUrol 1995 45:161-64.10.1016/S0090-4295(95)97824-0 [Google Scholar] [CrossRef]
[13]. Cutting CWM, Hindley RG, Poulsen J, Laparoscopic management of complicated urachal remnantBJU Int 2005 96:1417-21.10.1111/j.1464-410X.2005.05856.x16287469 [Google Scholar] [CrossRef] [PubMed]
[14]. Yamzon J, Kokorowski P, De Fillipp RE, Chang AY, Hardy BE, Koh CJ, Paediatric robotic-assisted laparoscopic excision of urachal cyst and bladder cuffJ Endourol 2008 22:2385-88.10.1089/end.2008.033818937602 [Google Scholar] [CrossRef] [PubMed]