CKD contributes to a major proportion of overall disease burden. Globally it is the 12th in terms of mortality and 17th in terms of disability [1]. Worldwide there were about 16 deaths per 100000 by the year 2013 and there was an overall increase in the last decade by about 36.9 % while comparing to that in 1993 [2]. It is estimated that there are 800 people living in India with CKD for every million population. These are not exact figures and they do not reflect the actual burden in India. Stage 1 and 2 usually go undetected as they present late. CKD causes an estimated 2.9% of overall mortality and about 3% of premature deaths in India [3]. In patients with CKD the most common cause of mortality is due to cardiovascular events. It is 10 to 30-fold more than that seen in the normal population; this in part may be explained by the accelerated atherosclerosis and the association of other factors like hypertension, diabetes and dyslipidaemia in such patients. Cardiovascular mortality increases with worsening of renal function independent of other factors [4].
The aortic knob width has been found to positively correlate with the severity of coronary artery disease [5] and was found to be increased in patients on haemodialysis compared to normal population [6]. This study describes the use of chest x-ray as a simple tool in evaluating CKD population who are at risk of cardiovascular events. The study assumes importance in resource poor setting such as our country where the access to tertiary care is limited. Therefore, this study was conducted with an aim to measure the aortic knob width by chest x-ray in CKD patients and compare it with Framingham’s’ risk scoring and other parameters.
Materials and Methods
A Cross-sectional study was conducted at Kasturba medical college Hospital and Government Wenlock hospital, Mangalore after taking the permission and approval of Kasturba medical college ethics committee (IEC KMC MLR 09-15/159). We determined the sample size of 60 based on earlier study [6]. The subjects of this study were CKD patients who were stage 3 to stage 5 as per KDIGO classification [7] on dialysis or being managed conservatively. Patients with known history of ischemic heart disease, old and present pulmonary tuberculosis, history of surgery of trachea and aorta were excluded. Additionally, patients whose chest x-ray was not properly centred (malrotation or tracheal deviation) were also excluded.
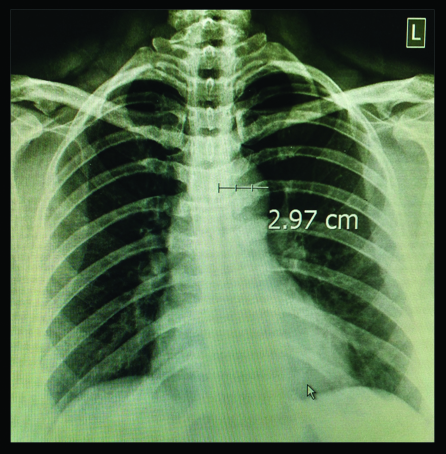
This study was performed in accordance with the Declaration of Helsinki and written informed consent was obtained from all patients before enrolment. Demographic characters were recorded for all patients. Patient’s investigations like serum urea, serum creatinine, serum magnesium, serum calcium, serum phosphate, serum albumin, serum total cholesterol and HDL cholesterol, haemoglobin and C-reactive protein were done. Electrocardiogram was done to look for previous myocardial infarction. Framingham 10 year cardiovascular risk prediction scoring was done [8]. Chest x-ray PA view was taken for these patients. The cassette of standard size 14x17 inch was placed at distance of 180 cm/6 feet from x-ray tube. On the x-ray viewing console, the widest point of the ascending aortic knob was measured (in cm) along the horizontal line from the point of the lateral edge of the trachea to the left lateral wall of the aortic knob [Table/Fig-1].
The Framinghams risk score was calculated by using the patients age, sex, blood pressure, total cholestrol and HDL cholestrol. The patients were categorised based on the score as mild (0-10%), moderate (11-20%) and high (>20%) risk. The AKW was compared with the Framingham’s risk score and other lab parameters.
Statistical Analysis
Statistical package SPSS version 17.0 was used. p<0.05 was considered as significant. Analysis was done in terms of mean, median, standard deviation and ROC curves were used to arrive at a cut-off for AKW which correlated with increased cardiovascular risk.
Results
The demographics of study population are described in [Table/Fig-2]. The aetiologies for CKD varied and included the following analgesic nephropathy (n:4), chronic glomerulonephritis (n:3), diabetes (n:29), hypertension (n:14), myeloma kidney (n:1), obstructive uropathy (n:6), Renal artery stenosis (n:2), granulomatosis with polyangiitis (n:1). The AKW measured in centi-metre varied from 2.08 to 4.47 cm with a mean of 3.2±0.43 among the study population.
Demographics of study population.
| Number (N) | Percentage (%) |
|---|
| Age |
| 20–30 | 17 | 28.3% |
| 31–40 | 24 | 40.0% |
| 41–50 | 19 | 31.7% |
| Male Sex | 45 | 75% |
| Smoker | 11 | 18.3% |
| Diabetics | 29 | 48.3% |
| Hypertensives | 49 | 81.7% |
| Dyslipidaemics | 2 | 3.3% |
| On Dialysis | 31 | 51.7% |
*Count - number of patients
†Column N% - percentage of total patients
Among the study population 45 were males and 15 females. Males were found to have higher AKW as compared to females [Table/Fig-3].
| Sex | N | Mean | Std.Deviation | t-test p-value |
|---|
| Female | 15 | 2.9760 | 0.36876 | .018 |
| Male | 45 | 3.2758 | 0.42735 |
There were 28 (46.7 %) patients who came under high risk, 18 (30%) under moderate risk and 14 (23.3 %) with mild risk as per Framinghams’ 10-year cardiovascular risk scoring. The AKW positively correlated with Framingham’s’ risk score. The p-value (<0.0001) was highly significant as done using Kruskall Wallis test [Table/Fig-4].
| FraminghamScore | N | Mean | StandardDeviation | Median(IQR) | Kruskallwallis test value | p | |
|---|
| Mild | 14 | 2.75 | 0.379 | 2.76(2.49 - 3.01 | 19.563 | 0.0001 | HS |
| Moderate | 18 | 2.276 | 0.255 | 3.21(3.12 - 3.56) |
| High | 28 | 3.377 | 0.391 | 3.39(3.15 – 3.64) |
*IQR-Interquartile range
There was a significant correlation between AKW and both systolic (r=0.038; p<0.0001) and diastolic (r=0.5465; p<0.0001) blood pressures. Karl pearsons correlation test showed no significant correlation between AKW and the various laboratory parameters as well as duration of disease [Table/Fig-5].
| Pearson Correlation co-efficient (r) | p |
|---|
| Duration of disease | 0.110 | 0.403 |
| Urea | 0.093 | 0.480 |
| Creatinine | 0.039 | 0.770 |
| Magnesium | -0.135 | 0.305 |
| Calcium | -0.026 | 0.843 |
| Phosphate | 0.094 | 0.474 |
| Albumin | -0.087 | 0.506 |
| Haemoglobin | 0.037 | 0.781 |
| C-reactive protein | -0.007 | 0.959 |
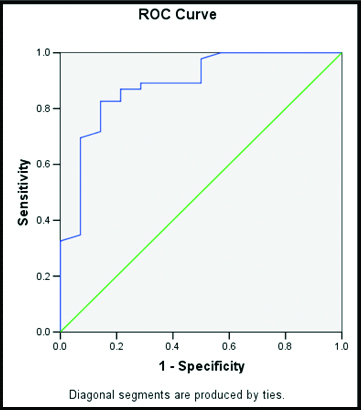
Using the ROC curve [Table/Fig-6], we found that AKW more than 3.1 centimetres corresponds with moderate to high risk as calculated using FRS scoring system with a sensitivity of 82% and specificity of 86%.
ROC curve.
*ROC curve drawn for AKW when comparing it with moderate to high risk as per FRS.
Discussion
There have been many attempts at identifying CKD patients who are at risk of CVD by using simple tools such as chest x-ray. The cardiothoracic ratio was evaluated to identify any correlation with increased cardiovascular mortality but studies failed to show any significant result in this regard [9].
The AKW was found to be useful tool in predicting cardiovascular mortality. Accelerated atherosclerosis which is a major factor/link in increased risk of cardiovascular events in CKD, leads to increased width of the Aortic knob. Hypertension being one of the major antecedent event related to major cardiovascular event was correlated with AKW and it was found to have significant positive correlation with both systolic and diastolic pressure which was similar to other studies [10,11].
Subsequent studies evaluated the use of AKW for its ability to predict various events with significant consequences on health such as ischemic heart disease and ischemic stroke. It was found that there was a significant correlation between AKW and the number of coronary vessels (by coronary angiogram) involved in ischemic heart disease patients, as well as co-relate with significant internal carotid artery stenosis (as assessed using Carotid-vertebral Doppler) which led to ischemic strokes [5,12].
The AKW is increased in CKD patients who are on haemodialysis [6]. In our study, we have assessed whether this increase in AKW translates to increased risk in terms of cardiovascular events. The risk of developing a cardiovascular event was calculated using well established Framingham’s Risk Scoring (FRS) system, which is based on incorporating the traditional risk factors for cardiovascular events [8].
The AKW in Indian population, even in elderly was found to be not more than 3.1 cm [13]. The mean value of AKW was found to be 3.2±0.43 cm in our study population which was lesser when compared to the mean value of AKW of 3.5±0.58 cm in CKD patients as found by Afsar B et al.,. This could be explained by the differences in ethnicity of both groups which paves way for the fact that AKW needs to be evaluated with keeping in mind the normal cut-off for the population at study rather than generalising the findings across different ethnic groups [6].
The AKW was found to be increased in patients who are at risk of developing a cardiovascular event within the next 10-years across all the three risk groups i.e., mild, moderate and severe. It was highly significant and the AKW positively correlated with FRS (p < 0.0001).
The AKW more than 3.1 cm is associated with moderate to high risk for cardiovascular events within the next 10 years with sensitivity 82% and specificity 86% while using FRS. Gürbak I et al., demonstrated that aortic knob of 37 mm constitutes the cut-off value for the presence of subclinical LV dysfunction with 85.9% sensitivity and 86.4% specificity [14].
We also found that there was a positive correlation of AKW with age and male sex similar to the findings of Afsar B et al., [6]. There was no correlation between AKW and other lab parameters commonly assessed in CKD patients such as serum urea, serum creatinine, serum magnesium, serum calcium, serum Phosphate, serum albumin, haemoglobin and C-reactive protein which in turn is contrary to the findings of Afsar B et al., where they had found increased AKW to correlate with creatinine, urea, albumin, phosphorus and CRP [6].
Limitation
In our study, we used FRS as an indirect indicator of cardiovascular risk hence a prospective study in future directly corelating AKW and cardiovascular events might add strength to our findings.
Conclusion
The results of this study allow the use of chest X-ray a cost-effective investigation modality commonly available, as a screening tool in patients with CKD. Patient with increased AKW can be identified as at-risk population and subjected to further evaluation and treatment.
*Count - number of patients
†Column N% - percentage of total patients
*IQR-Interquartile range