Angulated Custom Cast Post and Core Restoration for Traumatised Anterior Tooth-“Not as Straight as an Arrow”
Apra Butail1, Parminder Dua2, Ritu Mangla3, Ananya Chauhan4
1 Research Resident, Department of Pedodontics and Preventive Dentistry, Himachal Institute of Dental Sciences, Paonta Sahib, Sirmaur, Himachal Pradesh, India.
2 Professor and Head, Department of Pedodontics and Preventive Dentistry, Himachal Institute of Dental Sciences, Paonta Sahib, Sirmaur, Himachal Pradesh, India.
3 Reader, Department of Pedodontics and Preventive Dentistry, Himachal Institute of Dental Sciences, Paonta Sahib, Sirmaur, Himachal Pradesh, India.
4 Research Resident, Department of Pedodontics and Preventive Dentistry, Himachal Institute of Dental Sciences, Paonta Sahib, Sirmaur, Himachal Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Apra Butail, Research Resident, Himachal Institute of Dental Sciences, Rampur Ghat Road, Paonta Sahib, Sirmaur-173021, Himachal Pradesh, India.
E-mail: butail.apra@gmail.com
Traumatic dental injuries are most common injuries afflicting young children and generally involve the maxillary anterior teeth. Increased overjet with protrusion of upper incisors and insufficient lip closure are significant predisposing factors to traumatic dental injuries. Anterior tooth trauma leads to discomfort and serious psychological, aesthetic, functional, and phonetic problems that can affect social relationships. Treatment of a traumatically injured single central incisor poses significant challenges to the dentist and the patient. The reduced tooth structure makes retention of extra coronal restoration difficult. The purpose of cast post is to provide retention for the core restoration, which replaces the lost coronal tooth structure. This case report describes aesthetic rehabilitation of a fractured labially inclined left maxillary central incisor. Aesthetic and functional reconstruction was achieved by customising the axial inclination of the core followed by cementation with Porcelain Fused to Metal (PFM) crown. Thus, endodontic approach combined with prosthodontics provides a quick, reliable and economic treatment option.
Aesthetics, Anterior tooth trauma, Function, Metal post
Case Report
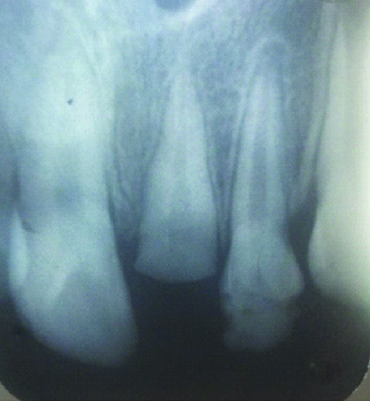
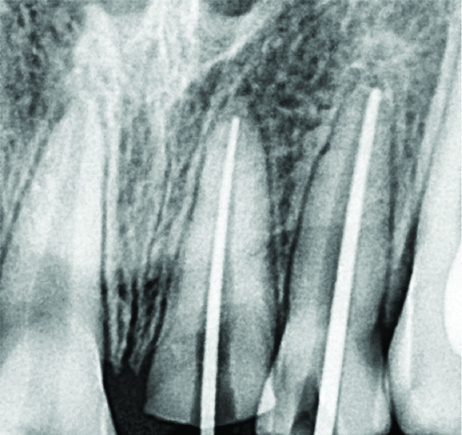
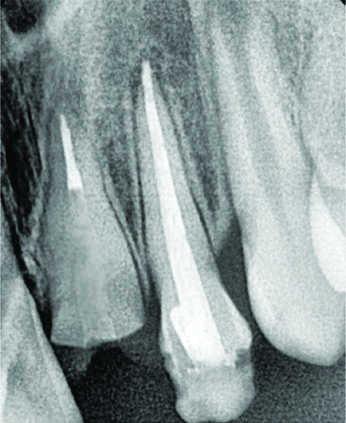
A 12-year-old boy reported to the Department of Paediatric and Preventive Dentistry, with a complex crown fracture of his left maxillary central incisor [Table/Fig-1]. His medical history was unremarkable. The trauma, was caused by a cycling accident, had occurred about one month earlier. The patient gave a history of pain and swelling in the upper front tooth region, which subsided after four to five days on its own. There was no bleeding. No medical or dental consultation was sought. However, one month after the trauma, the patient experienced pain and swelling in the maxillary anterior tooth region again for which he reported to our department. On intraoral examination, there were no lacerations or evidence of alveolar bone fracture or any gingival inflammation. The left maxillary central incisor showed a Class III fracture, with Grade 1 mobility. The tooth was non vital, with no response to the electric pulp test and other vitality tests. Radiographic examination showed complete root end development. There was carious pulp exposure in left maxillary lateral incisor [Table/Fig-1,2]. Keeping into consideration the tender age of the patient, we devised a treatment plan which was minimally invasive, cost effective and aesthetically sound. The patient and parents were given detailed information about the treatment plan, with its complications. Initially topical anaesthetic was applied at the site of injection followed by nerve block for adequate anaesthetisation (2% lignocaine 1.5 mL) and access opening was done in #21 and #22. The working length (15 mm for maxillary central incisor and 21 mm for the maxillary lateral incisor) was determined using a Radiovisiograph (RVG) for better resolution. The root canals were instrumented and both the teeth were filled with triple antibiotic paste (combination of ciprofloxacin, metronidazole, and minocycline). After two weeks, when the teeth were asymptomatic, cleaning and shaping of the canals was done using the step back technique. Copious irrigation with 2.5% NaOCl and 17% EDTA alternatively was done during the procedure. The canals were dried with paper points and were obturated with gutta-percha using lateral condensation technique followed by temporary restoration (3M Cavit G) [Table/Fig-3a,b and c]. To increase the clinical crown height gingivectomy was done around the maxillary central incisor by giving crevicular and interdental incisions so as to establish the desired gingival marginal position. On the next appointment, post space preparation was done with peeso reamer leaving the 5 mm of gutta-percha at apical end of root canal to maintain a good seal [Table/Fig-4]. An intraoral digitised periapical radiograph was obtained to evaluate the post space preparation. Inlay wax (GC Corp., Tokyo, Japan) was used for fabricating wax pattern. The core of the wax pattern was fabricated at an inclination of 20 degree palatal to the long axis of the root of the fractured tooth to achieve satisfactory aesthetics. The guidance for the same was obtained by the inclination of the adjacent central incisor. If the core was not subjected to inclination, the post would have remained in the direction of the long axis of tooth. The wax pattern was then sent to the casting laboratory for converting into metal post [Table/Fig-5]. The [Table/Fig-6] shows drastic change in the labiopalatal inclination created by custom post and core. The fit of the cast post and core was first assessed and then it was luted with glass ionomer cement (3M ESPE Ketac Molar). The remaining tooth structure was prepared with shoulder finish line on labial side and chamfer on the palatal side in #21 and #22 [Table/Fig-7]. Rubber base impression was made with heavy body (putty material) and light body (3M ESPE Soft putty). The cast was poured in die stone (Kalabhai Ultrarock). The shade selection for PFM crown was done in natural daylight with the adjacent teeth. Splint PFM crown was made for #21, #22 and cemented with luting glass ionomer cement [Table/Fig-8]. The patient reported no discomfort on one year follow-up [Table/Fig-9].
Preoperative photograph showing complex crown fracture of left maxillary central incisor and carious lateral incisor.

Preoperative radiovisograph showing complex crown fracture of left maxillary central incisor and carious lateral incisor.
Radiovisiograph depicting the working length i.e., 15 mm for maxillary central incisor and 21 mm for maxillary lateral incisor.

Radiovisiograph showing the master cones in #21 and #22.
Radiovisiograph showing the obturation done in #21 and #22 with gutta-percha.

Post space preparation done in #21 using peeso reamer leaving 5 mm of gutta-percha at the apical end of the root canal.
Angulated metal post with an inclination of 20°.

Marked change (20° palatal to long axis of root) in labiopalatal inclination created by custom post and core (Dotted line).

Photograph showing cemented metal post in #21 and PFM crown cutting done in #21 and #22.

Postoperative photograph with cemented Porcelain fused to metal crowns in #21 and #22.

Photograph after one year follow-up.

Discussion
For rehabilitation of traumatised anterior teeth, both aesthetic and mechanical aspects should be considered. Post and core is considered as the foundation restoration for mutilated dentition. The main purpose of this procedure is to provide retention for the core restoration, which replaces lost coronal structure. Post and core can be prefabricated post with composite build up or one piece custom made post [1]. The custom made post and core is indicated in various situations wherein gross tooth structure is lost, anterior deep bite, teeth with wider canals and where a change in angulation is required for enhancing aesthetics [2]. In the present case, crown lengthening also allowed the margins to be placed in sound tooth structure. According to a study done by Gegauff AG, a 2 mm ferrule obtained by crown lengthening resulted in a reduction of static load fracture [3]. Custom cast post and core is preferred over prefabricated post for any change in labiopalatal and mesiodistal angulation of proclined or angulated teeth. Custom cast post and core can be shaped until satisfactory aesthetic is achieved although, the core might not be in the same axis as the post or the root. However, in prefabricated post core system, the core is built around the post after post cementation in the prepared canal so that if tooth is rotated or more labially inclined, the post will remain in the direction of the long axis of that tooth. Any alteration in angulation, performed by the core shaping around the prefabricated post, usually leads to an unsupported core due to loss of coronal extended post during preparation. The functional loading of the crown over the unsupported core might result in fracture thereby, complicating the treatment [4]. Therefore, the only treatment option in such cases is the change in angulation with custom cast post and core followed by fabrication of PFM or zirconia based crown.
Conclusion
The aesthetic rehabilitation of traumatised labially inclined tooth poses tough challenge to the dentist. Custom cast post offers advantages in form of higher strength, precise fit with minimal luting surface and inherent anti rotation mechanism. In this case report, considering the age and aesthetic concerns of the patient we devised a treatment plan which was cost effective, had long lasting results and provided desirable aesthetics.
[1]. Smith CT, Schumann N, Prefabricated post and core systems: an overviewCompend Contin Educ Dent 1998 19(10):1013-20. [Google Scholar]
[2]. Shah NP, Gaikwad AM, Ram SM, Nadgere JB, Masking conventional metallic cast post for enhancing estheticsJ Contemp Dent 2016 6(1):85-89.10.5005/jp-journals-10031-1148 [Google Scholar] [CrossRef]
[3]. Gegauff AG, Effect of crown lengthening and ferrule placement on static load failure of cemented cast post-cores and crownsJ Prosthet Dent 2000 84:169-79.10.1067/mpr.2000.10758310946334 [Google Scholar] [CrossRef] [PubMed]
[4]. Singh K, Kumar N, Choudhary N, Gupta N, Unconventional prosthodontics for the aesthetic rehabilitation of discoloured rotated maxillary central incisorBMJ Case Rep 2013 :01-03.10.1136/bcr-2013-20004823893280 [Google Scholar] [CrossRef] [PubMed]