Posterior Tibial Artery Injury with Intact Posterior Tibial Pulse: A Case Report
Kamalakumar Karuppasamy1, Natarajan Shanmugam2, Gunalan Kannaiyya Naidu3, Surya Rao Rao Venkata Mahipathy4, Narayanamurthy Sundaramurthy5
1 Junior Resident, Department of Orthopaedics, Saveetha Medical College, Chennai, Tamil Nadu, India.
2 Professor, Department of Orthopaedics, Saveetha Medical College, Chennai, Tamil Nadu, India.
3 Assistant Professor, Department of Orthopaedics, Saveetha Medical College, Chennai, Tamil Nadu, India.
4 Professor, Department of Plastic Surgery, Saveetha Medical College, Chennai, Tamil Nadu, India.
5 Assistant Professor, Department of Plastic Surgery, Saveetha Medical College, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kamalakumar Karuppasamy, 159-B, R.S.K.P Road, Puliangudi, Tamil Nadu, India.
E-mail: dr.kamalakumar@gmail.com
The presence of distal pulses can be misleading and the presence of good vascularity to the affected part may be unrelated to the possibility of a vascular injury in orthopaedic trauma to the affected part. We report a case of Grade II open fracture of Proximal Tibia with Posterior Tibial Artery (PTA) tear. The case being presented came with an intact PTA pulsations clinically and with good vascularity to the lower limb, with no difference in the pulse rate between radial and posterior tibial pulse rate and no underlying bruits. The underlying PTA tear was found only incidentally on operating when the patient was taken up for open reduction with internal fixation with proximal tibial locking plate surgical procedure and the fracture site was opened. Arterial injuries following trauma may be missed without liberal use of arterial Arteriograms and Doppler study, unless looked for with a high degree of suspicion. If the arterial tear is identified early, patient and his limb can be saved without much morbidity to the patient, though diagnosing the injury is the hard part. Presence of intact and good peripheral pulses is not a sole criteria to rule out underlying vascular injury following orthopaedic trauma.
Intact arterial pulse post injury, Limb ischaemia, Vascular injury
Case Report
A 70-year-old male presented to the emergency room within 30 minutes after a road traffic accident caused by a 4 wheeler hitting the patient, and had multiple injuries to scalp, right leg, left elbow and shoulder. Patient was examined by the Emergency response team, the General Surgery team and the Orthopedic Surgery team. Patient did not have any vomiting, ENT bleeds or loss of consciousness following accident. Initial survey was done and airways, breathing and circulation were all intact. Patient was conscious and oriented at the time of admission and had a Glasgow Coma Scale (GCS) of 15 with no distal neurological deficits and had stable vitals. He had a laceration of size 5x1cm in the left elbow and a laceration of size 4x1cm in the right side of the forehead above the upper eyelids. A laceration of size 2x1 cm was present in the right leg, five cm below the tibial tuberosity, through which fractured end of tibia was visible, hence the fracture is Gustillo Anderson grade 2 compound fracture.
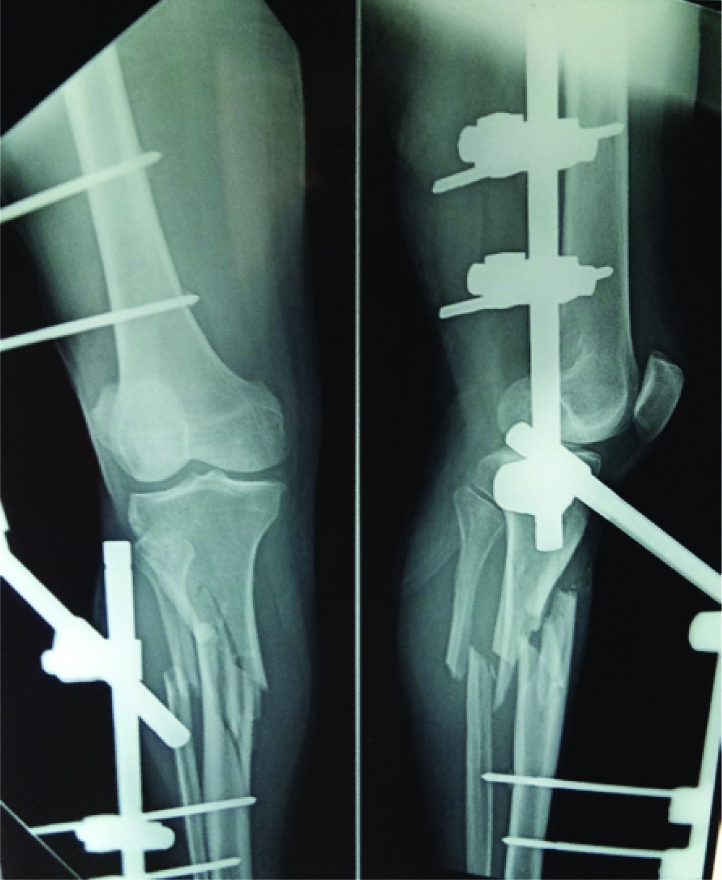
Radiographs of Right leg, Pelvis, Spine, Chest and left elbow were taken. An emergency-FAST scan was done which showed no evidence of abdominal injury. Computerised Tomogram (CT) of brain was done which showed no evidence of intracranial bleeding. He had fracture of proximal tibia and fibular shaft in X-rays with no fractures in any other site. Hence, he was evaluated for anesthesia and was taken up for surgery immediately and under spinal anesthesia, provisional external fixation procedure was done after a thorough wound wash and debridement [Table/Fig-1].
Patient treated with a provisional external fixation.
Patient was stable in the first 16 hours of postoperative period but started developing neurological deterioration. However, he became disoriented and started hitting his caregivers (both his nurses and his attenders). His blood pressure started falling to 90/60mm of mercury and was shifted to Intensive Care Unit where he received 1 unit packed cells to compensate the pre-operative blood loss and was given supportive treatment. Patient’s vitals stabilized over the next day but he continued to have episodes of delirium every now and then. Neuro-Surgery consultation was obtained and repeat CT was taken, which showed no significant abnormality other than chronic atrophic changes related to age.
Regular dressing of wound was done. The wound, along with the Ex-Fix pin site had more than normal soakage from bleeding but was otherwise healthy. The wound healed well and suture removal was done on post-operative day 10. Patient was stable with no significant abnormality other than intermittent bouts of delirium for which he was treated.
Patient was posted for surgery 15 days after the initial injury for providing a definitive fixation in the form of open reduction internal fixation with proximal tibial locking plate for the tibial fracture. He was found to have injury to the PTA on the operating table, after the External Fixation was removed and fracture site was opened [Table/Fig-2,3]. The PTA was found lacerated partially and the vein accompanying was torn and found to be thrombosed. The vein was ligated. The PTA injury seemed to have been caused by fractured end of the Tibia rather than the External fixation equipment as is usually the case with PTA injuries. Plastic surgeons were consulted for the case on table and PTA repair was done using 8-0 prolene [Table/Fig-4].
Arterial tear seen at the fracture site.

Close-up image of Posterior tibial arterial tear.

Arterial tear after repair with 8-0 prolene.

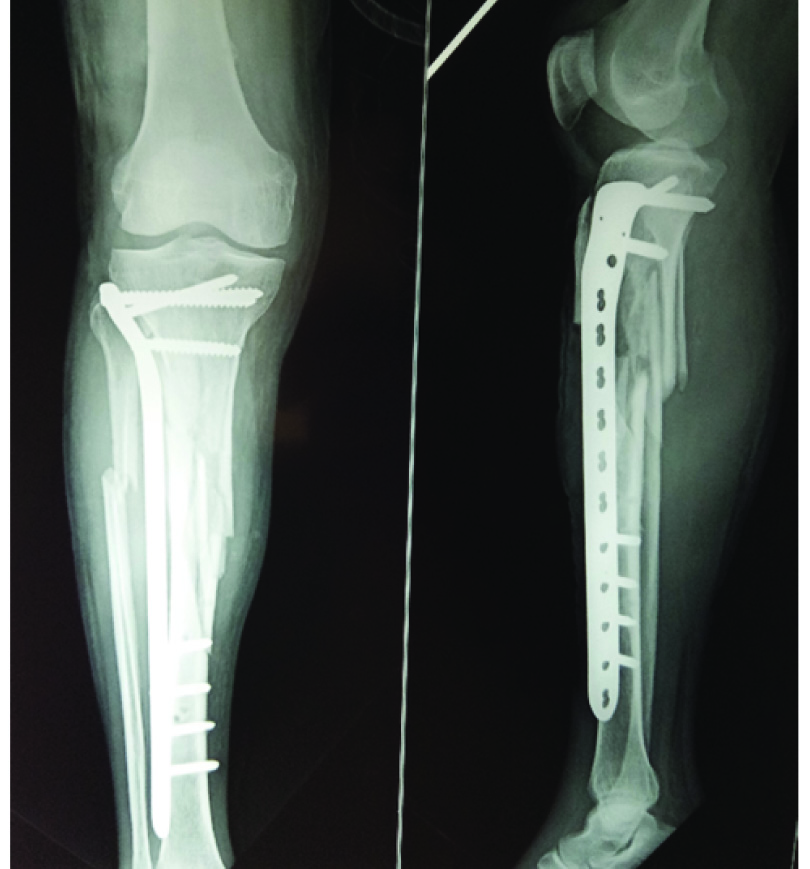
Patient’s fracture was then fixed with proximal tibial locking plate [Table/Fig-5]. Patient was given therapeutic dose of Heparin injections post-operative.
Patient X-ray post definitive internal fixation.
Post-operative period was uneventful following the second surgery and the patient’s neurological symptoms and delirium completely stopped without any other neurological intervention. The neurological manifestations in this patient might have been due to fat embolism or embolic episodes from the fracture site occurring through the injured vessel. Postoperative Doppler study of the lower limb was done which showed the repair of the PTA holding up. He was then mobilsed with non-weight bearing walking for the next 12 days and he was discharged after suture removal [Table/Fig-6]. He is on follow up now and his wounds have healed up well.
Wound site on postoperative day 12 after suture removal.

Discussion
The presence of distal pulses can be misleading and the presence of good vascularity to the affected part may be unrelated to the possibility of a vascular injury in orthopedic trauma to the affected part. The case being presented came with an intact PTA pulsations clinically and with good vascularity to the lower limb. The underlying PTA tear was found only incidentally on the operating table when the patient was taken up definitive fixation with open reduction and internal fixation. Arterial injuries following trauma may be missed without a high degree of suspicion and this case helps us to understand that presence of intact and good peripheral pulses is not a sole criteria to rule out underlying vascular injury following orthopaedic trauma. Similar cases of Anteriortibial arterial injury and PTA injury during plate [1-3]. application or pseudoaneurysm following plate removal have been reported. In cases of doubt as in excessive bleeding or expanding swellings, arteriograms may be helpful.
PTA damage following fracture of the proximal tibia is uncommon (about 12% in Tibial shaft fractures) and the arterial injuries are usually due to iatrogenic injury to the proximal tibial vessel following External Fixation of the proximal tibial fractures with Schanz pins or Illizarov’s ring fixator [4-6]. Early diagnosis and repair of such injuries is paramount in limb salvage and there is direct correlation between the time taken for diagnosis of arterial damage and limb amputation [7].
The classical feature of arterial injury such as, absence of the distal pulses, increase in the compartment pressure, decrease in the oxygenation of the periphery, decrease in the temperature of the periphery supplied by the artery and pallor of the peripheral tissue supplied by the artery is usually found in the complete transection of the artery. However, incomplete transections of the vessels or arterial injuries with only intimal tears may not present with the classical features of the vessel injury and may even present with an intact peripheral pulse. The incomplete tears of the arterial wall following injury may turn into AV fistula or Pseudo Aneurysm over the course of the disease and might preserve peripheral pulses. Perry et al., showed that 10% of fractures associated with vascular injury would have intact pulses [8].
In such cases, clinical diagnosis of the arterial vessel wall injuries can be made by feeling for the bruits in the peripheral pulses, any change in character of the pulse compared to the normal limb and by use of specific investigations like Arteriogram. The indications for an arteriogram as given by Saletta JD et al., are [9]:
Absent or diminished Peripheral pulses
Audible bruits
Unusually large extremity or pulsatile hematoma
Severe recurrent haemorrhage through the open wound
Knee dislocation
However, in rare cases, PTA injuries may present without the above clinical features. High degree of suspicion is needed to pick up the injury to the artery in such cases and liberal use of arteriogram as and when needed clinically might help in early detection of the injury to prevent further damage to the tissue from the vessel injury and its related effects.
The repair of the arterial laceration and definitive fixation of the fracture with plating also led to significant improvement in the general neurological status of the patient. The frequent bouts of delirium he suffered, stopped and he became neurologically stable after the definitive operation. This suggests that the neurological symptoms of the patients could have been due to fat embolism or micro-embolisms from the fracture site entering the injured vessel wall. This might explain the improvement in neurological status of the patient post-repair of the vessel [10,11].
Conclusion
Although presence or absence of the distal posterior tibial pulses is a good indicator of the vascular injuries from proximal tibial fractures, it may not be a reliable indicator of absence of PTA injury as it may present with normal pulsations clinically. Use of Arteriogram or Doppler to rule out arterial injury might help to prevent overlooking of the PTA vessel injury.
[1]. Katsuura Y, Gardner II WE, Transection of the anterior tibial artery during minimally invasive plate osteosynthesis of the proximal tibiaTrauma Case Reports 2017 8:32-35.10.1016/j.tcr.2017.01.01729644311 [Google Scholar] [CrossRef] [PubMed]
[2]. Ghaffari S, Farsavian H, Daneshpoor SM, Shayesteh M, Pseudoaneurysm of the posterior tibial artery following removal of tibial plate-A rare caseJournal of Orthopaedic Case Reports 2016 6(3):46 [Google Scholar]
[3]. Gary JL, Sciadini MF, Injury to the anterior tibial system during percutaneous plating of a proximal tibial fractureOrthopedics 2012 35(7):e1125-28.10.3928/01477447-20120621-3722784915 [Google Scholar] [CrossRef] [PubMed]
[4]. Suri T, Dabas V, Sural S, Dhal A, Pseudoaneurysm of the anterior tibial artery: A rare complication of proximal tibialsteinman pin insertionIndian Journal of Orthopaedics 2011 45(2):17810.4103/0019-5413.7714021430875 [Google Scholar] [CrossRef] [PubMed]
[5]. Breen T, Brumback R, Posterior tibial artery pseudoaneurysm following tibial fracture: A case reportOrthopedics 1985 8(8):993-97. [Google Scholar]
[6]. Haas LM, Staple TW, Arterial injuries associated with fractures of the proximal tibia following blunt traumaSouthern Medical Journal 1969 62(12):143910.1097/00007611-196912000-000015372056 [Google Scholar] [CrossRef] [PubMed]
[7]. Burkhardt GE, Cox M, Clouse WD, Porras C, Gifford SM, Williams K, Outcomes of selective tibial artery repair following combat-related extremity injuryJournal of Vascular Surgery 2010 52(1):91-96.10.1016/j.jvs.2010.02.01720471774 [Google Scholar] [CrossRef] [PubMed]
[8]. Perry MO, Thal ER, Shires GT, Management of arterial injuriesAnn Surg 1971 173(3):403-08.10.1097/00000658-197103000-000114927238 [Google Scholar] [CrossRef] [PubMed]
[9]. Saletta JD, Freeark RJ, Vascular injuries associated with fracturesOrthop Clin North Am 1970 1:93-102. [Google Scholar]
[10]. Bardana D, Rudan J, Cervenko F, Smith R, Fat embolism syndrome in a patient demonstrating only neurologic symptomsCanadian Journal of Surgery 1998 41(5):398 [Google Scholar]
[11]. Gupta B, D’souza N, Sawhney C, Farooque K, Kumar A, Agrawal P, Misra MC, Analyzing fat embolism syndrome in trauma patients at AIIMS Apex Trauma Center, New Delhi, IndiaJournal of Emergencies, Trauma and Shock 2011 4(3):33710.4103/0974-2700.8385921887021 [Google Scholar] [CrossRef] [PubMed]