Introduction
Urinary Tract Infections (UTIs) are the most common infections in children worldwide, however, data from Iran is not very well studied.
Aim
The aim of the present study was to evaluate the prevalence of UTIs in Iranian children.
Materials and Methods
From the beginning of databases to November 2017, International {PubMed, Web of Science (WOS) and Google scholar} and National {Scientific Information Database (SID), Magiran} databases were searched for related observational studies that were conducted in Iran including only on Iranian children and published in English and Persian languages. The quality of the articles was evaluated using the Hoy D tool.
Results
Out of 515 initial studies, 14 and 6 studies were included in systematic review and meta-analysis, respectively. The overall prevalence of UTI in 3926 children was 4.92% (95% CI:2.32, 7.52; I2=93.58%). The prevalence of UTI in male and female children was 2.59% and 4.78%, and the difference was non-significant.
Conclusion
Considering the prevalence of UTIs in Iranian children, it is recommended that studies should be conducted in the field of research at the national level to determine the precise incidence and risk factors for UTIs in children.
Introduction
Globally, UTIs are the most common infectious disease in children [1]. In USA (2007) more than 10.5 million cases were diagnosed with symptoms of UTIs [2]. UTI is a term used for a wide range of clinical disorders of asymptomatic bacteriuria, infection of the kidneys, and sepsis [3]. UTIs are the most commonly reported infections in children [4-6]. Based on a meta-analysis study, the global incidence of UTIs in children is 7% [7]. In children, UTIs can have varying degrees of severity [8]. Symptoms like fever can also lead to chronic kidney failure as likelihood of scar formation in the kidney increases [9,10]. Therefore, early diagnosis of UTI is important, especially in children with special conditions of childhood, which does not allow the proper collection of urine samples, especially in developing countries where there is no access to appropriate primary care centres [11]. There is no precise and accurate prevalence of UTI in Iranian children except the Tola H et al., study which was conducted only on a specific population based on age (infants and specific disease) of infants with jaundice that the prevalence of UTI was 11% [12]. Policy makers can identify one of the most important health problems that can be reduced by correct screening. Conversely, if not identified, there would be an increased risk of developing chronic kidney disease which imposes a huge cost on healthcare system. This systematic review was conducted to determine the prevalence of UTIs in Iranian children.
Materials and Methods
This systematic review adopted methods developed in accordance with the guidelines detailed on the PRISMA checklist [13].
Inclusion and exclusion criteria: Only observational studies were included however, letter to editors, reviews, articles without quality (based on hoy tool) and studies conducted on adult’s participants were excluded. Only articles in English and Persian languages were included. The studies confirming with the UTI definition as “UTI is defined as bacteriuria of more than 105 CFU/mL in urine culture along with/without urinary symptoms” [14,15].
Sampling methods and sample size: All observational studies with any sampling and census designs were included in the present systematic review.
Search strategy: Two independent researchers conducted searches in International (PubMed, Google Scholar and WOS) and National databases (SID and Magiran) from the launching of the databases to November 2017, without time limitation in English and Persian languages. The references list of included articles are checked for finding more related articles. Specific search strategies were created by a Health Sciences Librarian with expertise in systematic review searching by using MESH terms and free terms according to the PRESS standard [16]. We used the MEDLINE search strategy for searching other databases. The keywords used in the search strategy were: Urinary tract infection, UTI, Paediatrics, Children and Iran which were combined with Boolean operators including AND, OR, and NOT.
Selection of studies and data extraction: By considering the eligibility criteria, two researchers independently screened the titles and abstracts. After removing duplicate studies, full texts of the studies were screened depending on the eligibility criteria and the required information were extracted. To resolve questions about eligibility, additional information was obtained from the authors of the study wherever necessary. General information (first author, province and year of publication), study characteristics (sampling method, study design, setting, sample size and risk of bias) and outcome measures (prevalence of UTI) were also collected.
Quality assessment and abstraction: The Hoy D et al., tool was used to evaluate the methodological quality and risk of bias of each included observational study [17]. This 10-item tool was used to evaluate the quality of studies in two dimensions including external validity (items 1-4 assessed the target population, sampling frame, sampling method and non-response bias minimal) and internal validity (items 5-9 assessed the data collection method, case definition, study instrument, mode of data collection while item 10 assessed bias related to data analysis). The higher score showed a lower risk of bias and the lower score showed a higher risk of bias. The risk of bias was independently evaluated by two researchers. The consensus method was used to resolve disagreements.
Data synthesis: Extracted data of final included studies combined by forest plot and prevalence of UTI assessed by random effect model using STAT 14.0 statistical software.
Results
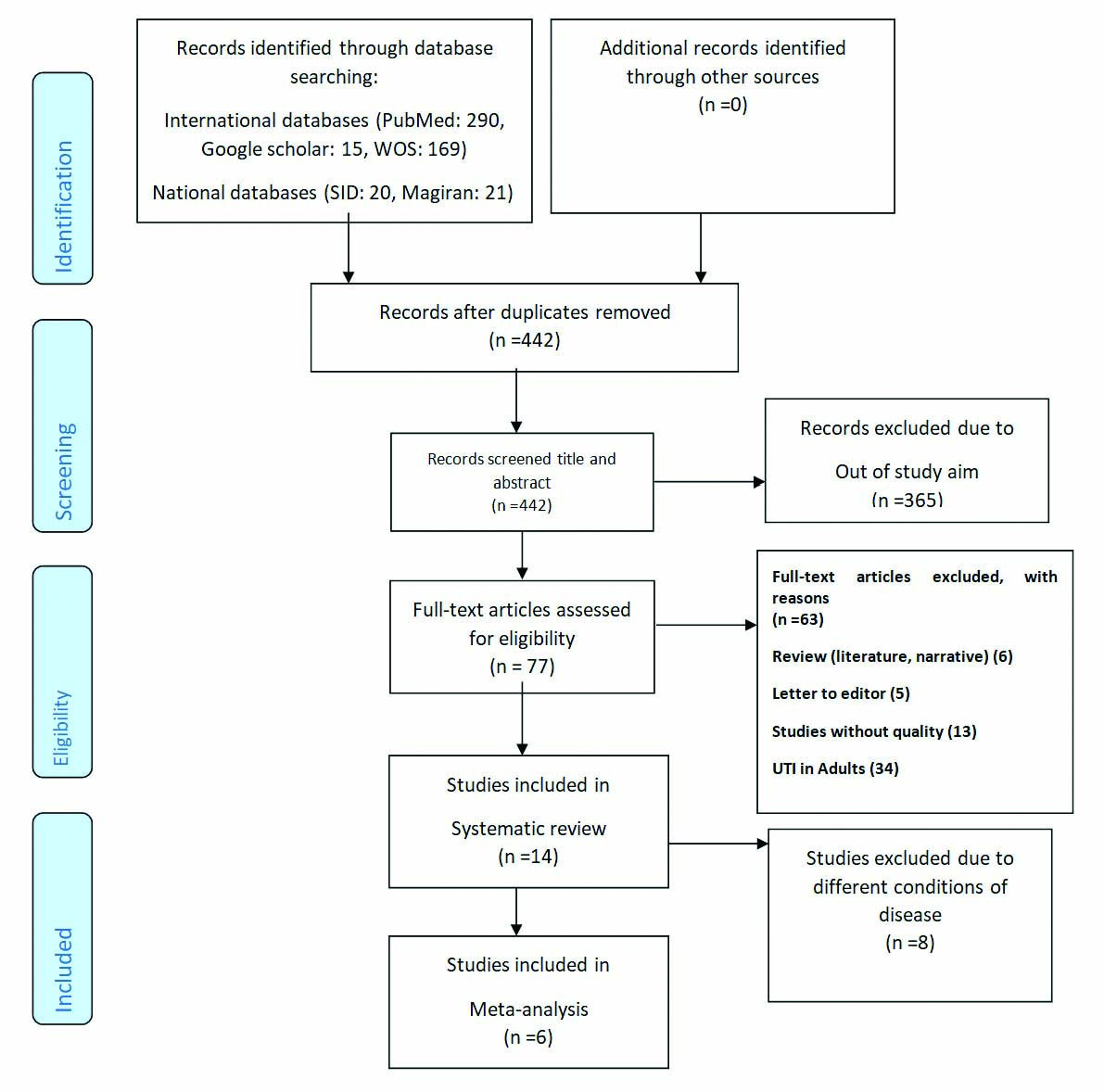
Study selection: A total of 515 articles were retrieved from the initial search in PubMed, Google scholar, SID, Magiran, and Web of science from inception to 1 November 2017. From a total of 442 non-duplicated studies in the title and abstracts screening process, 365 studies were excluded because their titles were unrelated. Of 77 studies, 14 studies met the eligibility criteria. Of the 63 excluded studies, six studies were review, five studies were letter to editor, 34 studies examined UTI prevalence in adults, five studies did not have full text and 13 studies did not meet the least quality requirement for inclusion in the study [Table/Fig-1].
Flow diagram of study selection.
Study characteristics: These 14 studies were conducted on 6786 (male:3,339; female:3,447) Iranian children with age range between 2 to 12 years [18-31]. Out of the 14 included studies, 13 studies provided cross-sectional data, one study was a prospective study [19]. Out of the 14 studies, four studies were from Fars [21,23,24,29], two studies were from Ardabil [22,30] and Tehran [19,28] and one study was from East Azerbaijan [18], South Khorasan [25], sistan and Baluchestan [31], Golestan [20], Hamadan [27] and a national study [26], respectively. The most common sampling method used was convenience (n=4). More than 85% of studies had a low risk of bias. The most common setting where studies were conducted was in the hospital (n=11). Of 14 studies only six studies were included in final meta-analysis, other eight studies excluded from final analysis due to different type of diseases that affected the UTI in children participants. Prevalence of UTI in children were between 5.8% to 38% in children with constipation (n=120) and nephrotic syndrome (n=124), respectively [Table/Fig-2].
Characteristics of final included studies about prevalence of UTI in Iranian children.
| First author | Year | Province | Sampling method | Design | Setting | Study population | Sample size | Overall Prevalence (%) | Risk of bias |
|---|
| Abdinia B et al., [18] | 2013 | East Azerbaijan | Random Cluster | Cross-Sectional | School | Asymptomatic | 312 | 3.8 | Moderate |
| Abedi A et al., [19] | 2017 | Tehran | Convenience | Prospective | Hospital | Cystic fibrosis | 153 | 11.11 | Low |
| Cheraghi M et al., [20] | 2017 | Golestan | Convenience | Cross-Sectional | Health center | Asymptomatic | 2145 | 6.81 | Low |
| Dehghani SM et al., [21] | 2013 | Fars | Purposive | Cross-Sectional | Hospital | Constipation | 120 | 5.83 | Low |
| Etehad G [22] | 2000 | Ardabil | Convenience | Cross-Sectional | Hospital | Multiple diseases | 100 | 30 | Low |
| Fallahzadeh MH and Ghane F [23] | 2006 | Fars | Consecutive | Cross-Sectional | Hospital | Kidney transplantation | 120 | 6.67 | Low |
| Fallahzadeh MK et al., [24] | 2011 | Fars | Census | Cross-Sectional | Hospital | Diarrhoea | 138 | 17.39 | moderate |
| Fesharakinia A et al., [25] | 2006 | South Khorasan | Multistage cluster | Cross-Sectional | Hospital | Asymptomatic | 278 | 1.08 | Low |
| Kalantar E et al., [26] | 2008 | National | Convenience | Cross-Sectional | Hospital | Multiple diseases | 1669 | 26.20 | moderate |
| Mahmoudi H et al., [27] | 2015 | Hamadan | Two stage cluster | Cross-Sectional | Hospital | Asymptomatic | 350 | 12.86 | Low |
| Panahi Y et al., [28] | 2008 | Tehran | Purposive | Cross-Sectional | Hospital | Febrile | 433 | 9.01 | Low |
| Porahmad M [29] | 2005 | Fars | Cluster | Cross-Sectional | School | Asymptomatic | 387 | 2.33 | Low |
| Rostami M et al., [30] | 2005 | Ardabil | Simple random | Cross-Sectional | School | Asymptomatic | 454 | 4.19 | Low |
| Salarzaei M et al., [31] | 2017 | Sistan and Baluchestan | Simple random | Cross-Sectional | Hospital | Nephrotic syndrome | 124 | 37.90 | Low |
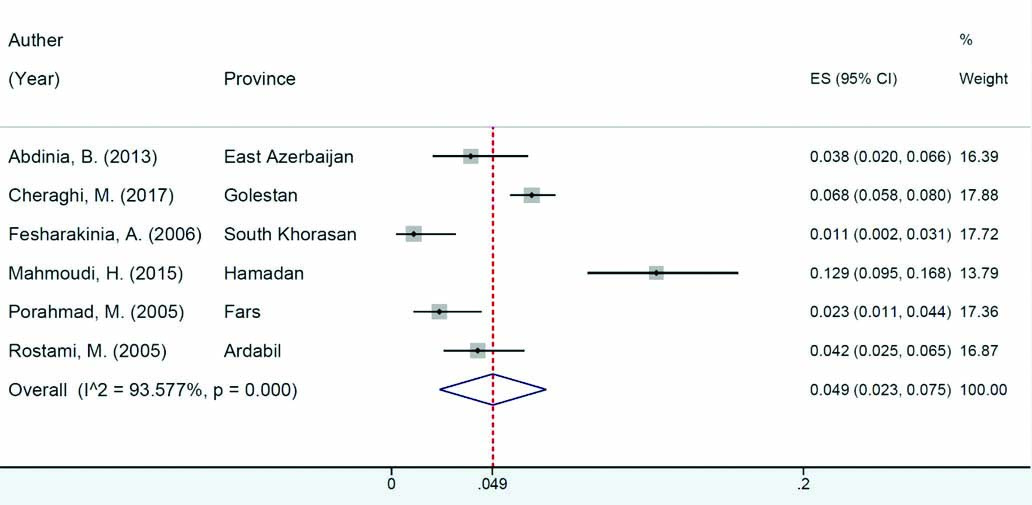
Prevalence of UTIs in children: Six studies that were conducted on 3926 children (male:1939/female:1987) were included in meta-analysis [18,20,25,27,29,30]. In asymptomatic children based on the results of the random effect method, the overall prevalence of UTI in 3926 children was 4.92% (95% CI: 2.32, 7.52; I2=93.58%) [Table/Fig-3]. Prevalence of UTI in male and female children were 2.59% (95% CI: 1.88, 3.29) and 4.78% (95% CI: 3.86, 5.71), respectively and this difference was also found in the study participant’s sub-group [Table/Fig-4].
Prevalence of children’s UTI in health population studies and of pooled prevalence of UTI estimate in Iran.
Prevalence of UTI in asymptomatic children by gender.
| Firstauthor | Male | Female |
|---|
| ES | 95% CI for ES | % Weight | ES | 95% CI for ES | % Weight |
|---|
| Abdinia B et al., [18] | 0.71 | 0.13, 3.93 | 25.32 | 6.40 | 3.61, 11.09 | 6.35 |
| Cheraghi M et al., [20] | 4.66 | 3.57, 6.06 | 32.16 | 9.13 | 7.52, 11.04 | 27.45 |
| Fesharakinia A et al., [25] | 1.35 | 0.37, 4.79 | 14.24 | 0.77 | 0.14, 4.23 | 37.64 |
| Mahmoudi H et al., [27] | 7.69 | 4.23, 13.58 | 2.35 | 15.91 | 11.67, 21.32 | 3.63 |
| Porahmad M [29] | 1.58 | 0.54, 4.54 | 15.68 | 3.05 | 1.40, 6.48 | 14.74 |
| Rostami M et al., [30] | 2.78 | 1.28, 5.93 | 10.26 | 5.46 | 3.22, 9.12 | 10.19 |
| Overall random pooled ES | 2.59 | 1.88, 3.29 | 100 | 4.78 | 3.86, 5.71 | 100 |
ES: Effect size
Discussion
This systematic review was conducted to determine the prevalence of UTIs in Iranian children until November 2017. The overall prevalence of UTI among asymptomatic Iranian children was 4.92%, which is lower than the prevalence of UTI in children of India (15%) [32]. The probable cause of this variation is attributed to sample size, research methodology and the study setting in both researches. Also, according to individual studies in the United States (9%) [33], England (5.6%) [34], and Turkey (7.1%) [35], it was found that the UTI rate is lower compared to the figures published in Iran. This difference can be attributed to the methodological differences in studies as well as the existence of better screening programs for children in the above mentioned countries [36-38]. Also, the results of this study showed that the prevalence of UTI is higher in women than in men, in line with studies in the United States [39] and Turkey [35], which can be due to the shorter urine tract in women. One of the most important sub-factors in urinary tract infections is poor health behaviours, especially in developing countries. By increasing education in family and community level towards management of risk factors of UTI is crucial.
Limitation
The limitations of the present study were less number of studies related to the topic and heterogenous group of participants in studies. The lack of clarity of the causes of UTIs in most studies. In retrospect, the authors feel that if few more keywords like pyelonephritis, cystitis, urethritis, pyonephrosis, bacteriuria would have been included during literature search then it would have led to better results.
Conclusion
The results of the present study provide healthcare policymakers with precise prevalence rate of UTIs in children which enables them to make necessary plans according to their actual level.
Considering the prevalence of UTIs in Iranian children, it is recommended to perform studies in the field at national level to determine the precise incidence and risk factors for UTIs in children.
ES: Effect size
[1]. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ, Urinary tract infections: epidemiology, mechanisms of infection and treatment optionsNat Rev Microbiol 2015 13(5):269-84.10.1038/nrmicro343225853778 [Google Scholar] [CrossRef] [PubMed]
[2]. Foxman B, The epidemiology of urinary tract infectionNat Rev Microbiol 2010 7(12):653-60.10.1038/nrurol.2010.19021139641 [Google Scholar] [CrossRef] [PubMed]
[3]. Chua M, Ming J, Chang SJ, Dos Santos J, Mistry N, Silangcruz JM, A critical review of recent clinical practice guidelines for pediatric urinary tract infectionCanadian Urological Association Journal 2017 12(4)10.5489/cuaj.479629319481 [Google Scholar] [CrossRef] [PubMed]
[4]. Foxman B, Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burdenInfect Dis Clin North Am 2014 28(1):01-13.10.1016/j.idc.2013.09.00324484571 [Google Scholar] [CrossRef] [PubMed]
[5]. Das R, Ahmed T, Saha H, Shahrin L, Afroze F, Shahid A, Clinical risk factors, bacterial aetiology, and outcome of urinary tract infection in children hospitalized with diarrhoea in BangladeshEpidemiology & Infection 2017 145(5):1018-24.10.1017/S095026881600297128029092 [Google Scholar] [CrossRef] [PubMed]
[6]. Wallace SS, Brown DN, Cruz AT, Prevalence of concomitant acute bacterial meningitis in neonates with febrile urinary tract infection: a retrospective cross-sectional studyThe Journal of Pediatrics 2017 184:199-203.10.1016/j.jpeds.2017.01.02228185626 [Google Scholar] [CrossRef] [PubMed]
[7]. Tandogdu Z, Wagenlehner FM, Global epidemiology of urinary tract infectionsCurr Opin Infect Dis 2016 29(1):73-79.10.1097/QCO.000000000000022826694621 [Google Scholar] [CrossRef] [PubMed]
[8]. Shaikh N, Hoberman A, Keren R, Gotman N, Docimo SG, Mathews R, Recurrent urinary tract infections in children with bladder and bowel dysfunctionPediatrics 2016 137(1):e2015298210.1542/peds.2015-298226647376 [Google Scholar] [CrossRef] [PubMed]
[9]. Park YS, Renal scar formation after urinary tract infection in childrenKorean Journal of Pediatrics 2012 55(10):367-70.10.3345/kjp.2012.55.10.36723133482 [Google Scholar] [CrossRef] [PubMed]
[10]. Beiraghdar F, Panahi Y, Einollahi B, Moharamzad Y, Nemati E, Amirsalari S, Predisposing factors for renal scarring in children with urinary tract infectionSaudi Journal of Kidney Diseases and Transplantation 2012 23(3):532 [Google Scholar]
[11]. Rosenthal VD, Ramachandran B, Dueñas L, Çlvarez-Moreno C, Navoa-Ng JA, Armas-Ruiz A, Findings of the International Nosocomial Infection Control Consortium (INICC), Part I: effectiveness of a multidimensional infection control approach on catheter-associated urinary tract infection rates in pediatric intensive care units of 6 developing countriesInfect Control Hosp Epidemiol 2012 33(7):696-703.10.1086/66634122669231 [Google Scholar] [CrossRef] [PubMed]
[12]. Tola H, Ranjbaran M, Omani-Samani R, Sadeghi M, Prevalence of UTI among Iranian infants with prolonged jaundice, and its main causes: A systematic review and meta-analysis studyJournal of Pediatric Urology 2018 14(2):108-15.10.1016/j.jpurol.2018.01.00429456119 [Google Scholar] [CrossRef] [PubMed]
[13]. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P, Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statementPLoS Medicine 2009 6(7):e100009710.1371/journal.pmed.100009719621072 [Google Scholar] [CrossRef] [PubMed]
[14]. Lee JB, Neild GH, Urinary tract infectionMedicine 2007 35(8):423-28.10.1016/j.mpmed.2007.05.009 [Google Scholar] [CrossRef]
[15]. Roberts KB, Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 monthsPediatrics 2011 128(3):595-610.10.1542/peds.2011-133021873693 [Google Scholar] [CrossRef] [PubMed]
[16]. McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C, PRESS peer review of electronic search strategies: 2015 guideline statementJournal of Clinical Epidemiology 2016 75:40-46.10.1016/j.jclinepi.2016.01.02127005575 [Google Scholar] [CrossRef] [PubMed]
[17]. Hoy D, Brooks P, Woolf A, Blyth F, March L, Bain C, Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreementJ Clin Epidemiol 2012 65(9):934-39.10.1016/j.jclinepi.2011.11.01422742910 [Google Scholar] [CrossRef] [PubMed]
[18]. Abdinia B, Mohkam M, Karimi A, Alikhah F, Prevalence rate of urinary tract infection and disorder of urinary profiles in the 7-12 years old healthy children in Tabriz, IranArch Pediatr 2013 1(3)10.5812/pedinfect.10347 [Google Scholar] [CrossRef]
[19]. Abedi A, Moghtaderi M, Ashrafi M, Prevalence of urinary tract infection among children with febrile convulsionInt J Nephrol Kidney Failure 2017 3(1)10.16966/2380-5498.143 [Google Scholar] [CrossRef]
[20]. Cheraghi M, Zare MR, Vakili MA, Hafezi AA, Nikyar A, Prevalence of urinary tract infections among first grade primary school Children in Gorgan, Northeast of IranJournal of Clinical and Basic Research 2017 1(1):22-26.10.18869/acadpub.jcbr.1.1.22 [Google Scholar] [CrossRef]
[21]. Dehghani SM, Basiratnia M, Matin M, Hamidpour L, Haghighat M, Imanieh MH, Urinary tract infection and enuresis in children with chronic functional constipationIranian journal of kidney diseases 2013 7(5):363-66. [Google Scholar]
[22]. Etehad G, The study of common bacterial contaminated urinary tract infections in children admitted to Ali Asghar Hospital in Ardabil in 1994Journal of Ardabil University of Medical Sciences 2000 1(2):01-03. [Google Scholar]
[23]. Fallahzadeh MH, Ghane F, Urinary tract infection in infants and children with diarrhoeaEastern Mediterranean Health Journal 2006 12(5):690-94. [Google Scholar]
[24]. Fallahzadeh MK, Fallahzadeh MH, Derakhshan A, Basiratnia M, Hoseini Al-Hashemi G, Fallahzadeh MA, Urinary tract infection after kidney transplantation in children and adolescentsIranian journal of kidney diseases 2011 5(6):416-19. [Google Scholar]
[25]. Fesharakinia A, Taheri F, Saadatjoo SA, The prevalence of urinary tract infection in 7-years children of Birjand city: Screening of urinary tract infection in the children before attendance to primary school?Pathobiology Research 2006 9(85):53-56. [Google Scholar]
[26]. Kalantar E, Esmaeel Motlagh M, Lornejad H, Reshadmanesh N, Prevalence of urinary tract pathogens and antimicrobial susceptibility patterns in children at hospitals in IranArchives of Clinical Infectious Diseases 2008 3(3) [Google Scholar]
[27]. Mahmoudi H, Emadmomtaz H, Karimitabar Z, Emam AH, Alikhani MY, Prevalence of asymptomatic urinary tract infection in primary school children of Hamadan City and drug resistance of isolated microorganisms in 2014Pajouhan Scientific Journal 2015 13(3):08-14. [Google Scholar]
[28]. Panahi Y, Beiraghdar F, Moharamzad Y, Matinzadeh ZK, Einollahi B, The incidence of urinary tract infections in febrile children during a two-year period in Tehran, IranTropical doctor 2008 38(4):247-49.10.1258/td.2008.07035618820202 [Google Scholar] [CrossRef] [PubMed]
[29]. Porahmad M, The prevalence of urinary tract infection in primary school children in Jahrom in 2002Hormozgan Medical Journal 2005 9(2):137-42. [Google Scholar]
[30]. Rostami Magsodian Pour A, Arian Prevalence of Asymptomatic Urinary Tract Infection in Primary School Children of ArdabilJournal of Ardabil University of Medical Sciences 2005 5(3):241-45. [Google Scholar]
[31]. Salarzaei M, Saravani S, Heydari M, Aali H, Malekzadegan A, Soofi D, Prevalence of urinary tract infection in children with nephrotic syndromeInternational Journal of Pharmaceutical Sciences and Research 2017 8(7):3146-50. [Google Scholar]
[32]. Narain U, Gupta A, Urinary tract infection in children with nephrotic syndromeThe Pediatric Infectious Disease Journal 2018 37(2):144-46.10.1097/INF.000000000000174728827494 [Google Scholar] [CrossRef] [PubMed]
[33]. Zorc JJ, Levine DA, Platt SL, Dayan PS, Macias CG, Krief W, Clinical and demographic factors associated with urinary tract infection in young febrile infantsPediatrics 2005 116(3):644-48.10.1542/peds.2004-182516140703 [Google Scholar] [CrossRef] [PubMed]
[34]. Butler CC, O’Brien K, Pickles T, Hood K, Wootton M, Howe R, Childhood urinary tract infection in primary care: a prospective observational study of prevalence, diagnosis, treatment, and recoveryBr J Gen Pract 2015 65(633):e217-e23.10.3399/bjgp15X68436125824181 [Google Scholar] [CrossRef] [PubMed]
[35]. Zincir H, Erten ZK, Özkan F, Sevig Ü, Baser M, Elmalı F, Prevalence of urinary tract infections and its risk factors in elementary school studentsUrologia Internationalis 2012 88(2):194-97.10.1159/00033555422327441 [Google Scholar] [CrossRef] [PubMed]
[36]. Fatholahzadeh B, Hashemi FB, Emaneini M, Aligholi M, Nakhjavani FA, Kazemi B, Detection of vancomycin resistant enterococci (VRE) isolated from urinary tract infections (UTI) in Tehran, IranDARU Journal of Pharmaceutical Sciences 2006 14(3):141-45. [Google Scholar]
[37]. Farajnia S, Alikhani MY, Ghotaslou R, Naghili B, Nakhlband A, Causative agents and antimicrobial susceptibilities of urinary tract infections in the northwest of IranInternational Journal of Infectious Diseases 2009 13(2):140-44.10.1016/j.ijid.2008.04.01418703368 [Google Scholar] [CrossRef] [PubMed]
[38]. Mihankhah A, Khoshbakht R, Raeisi M, Raeisi V, Prevalence and antibiotic resistance pattern of bacteria isolated from urinary tract infections in Northern IranJournal of Research in Medical Sciences: The Official Journal of Isfahan University of Medical Sciences 2017 :2210.4103/jrms.JRMS_889_1629026424 [Google Scholar] [CrossRef] [PubMed]
[39]. Bachur R, Harper MB, Reliability of the urinalysis for predicting urinary tract infections in young febrile childrenArchives of Pediatrics & Adolescent Medicine 2001 155(1):60-65.10.1001/archpedi.155.1.6011177064 [Google Scholar] [CrossRef] [PubMed]