Sternalis -An Accessory Muscle of Thoracic Wall
Virendra Budhiraja1, Swati Bansal2, Rakhi Rastogi3, Shveta Swami4, Rimpi Gupta5
1 Professor, Department of Anatomy, Kalpana Chawla Govermnent Medical College, Karnal, Haryana, India.
2 Demonstrator, Department of Anatomy, Kalpana Chawla Govermnent Medical College, Karnal, Haryana, India.
3 Professor, Department of Anatomy, Ganga Saran Medical College, Hapur, Uttar Pradesh, India.
4 Associate Professor, Department of Anatomy, Kalpana Chawla Govermnent Medical College, Karnal, Haryana, India.
5 Assistant Professor, Department of Anatomy, Kalpana Chawla Govermnent Medical College, Karnal, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Swati Bansal, Demonstrator, Department of Anatomy, Medical College Block, Karnal-132001, Haryana, India.
E-mail: bansal.swati64@gmail.com
Sternalis muscle is an anatomical aberration among the muscle group of anterior chest wall. This accessory muscle was discovered bilaterally in a 40-year-old female cadaver. The muscle which emanated from the external oblique aponeurosis was fleshy throughout its extent except at the ends where it was aponeurotic. At the sternal angle, the muscle displayed inverted “V” shaped configuration and merged with the opposite pectoralis major muscle. It is clinically very important in female patients as compared to male patients because of mammary gland surgeries, lymph node irradiation, postoperatively can be confused with recurrence etc. The present case endeavors to discuss the anatomical, embryological and clinical relevance of a rare accessory muscle of the anterior chest wall.
Aberrant, Aponeurotic, Pectoral
Case Report
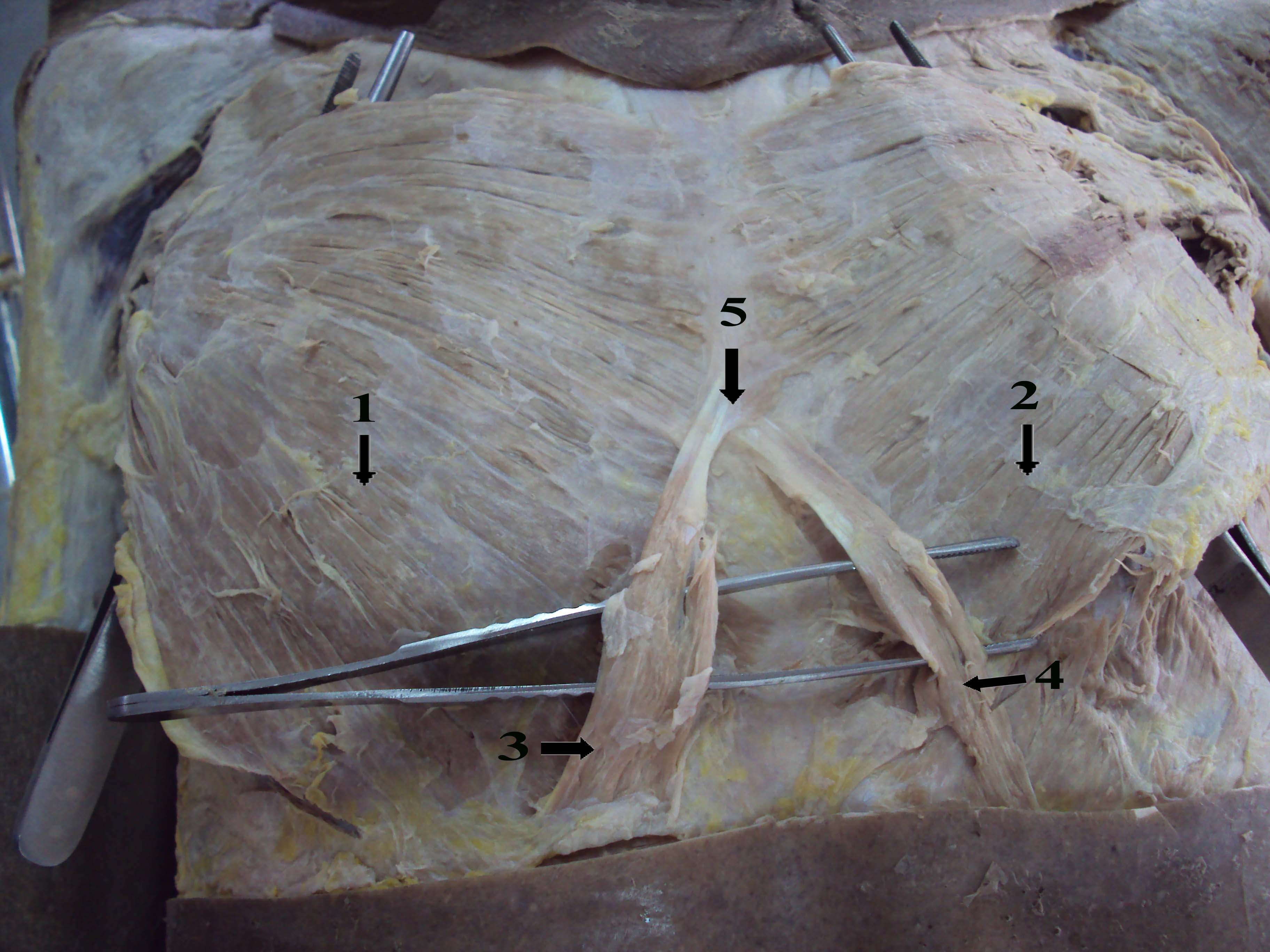
During routine cadaveric dissection, as a part of anatomy teaching for MBBS students, in a 45-year-old female cadaver we found an accessory muscle called sternalis, superficial to pectoralis major on both sides of pectoral region after removing mammary gland. It presents a slightly oblique orientation with respect to the sternal margin. Photographs and details of this muscle were taken after cleaning the dissected area [Table/Fig-1]. This accessory slip of muscle originated inferiorly from aponeurosis of external oblique both on right and left side and going upwards in slight oblique manner and inserted on to the sternum at the level of 4th costal cartilage and merges with the fibres of opposite pectoralis major. Caudally the attachment was fleshy with the aponeurosis of external oblique and cranially it was aponeurotic in its attachment with pectoralis major fibres. It is also important to note that there was criss crossing of fibres of sternalis on the sternum and opposite side sternalis was merging with the fibres of same side of pectoralis major muscle. Because of this criss-crossing, both the sides of sternalis are forming the pattern of inverted ‘V’. The fibres of this accessory muscle was 2.5 cm from the midsternal line and the length was 7.5 cm from its caudal to cranial attachment and the breadth was 2.5 cm. It was of regular flame shape with its longitudinal and a parasternal course. It was difficult to show the innervation source of Sternalis muscle in this cadaver, as during separation of the lateral margins of muscle, the twigs from the pectoral nerve, which could be easily be confused with the connective tissue, were almost removed or damaged.
Bilateral sternalis muscle showing criss crossing of fibres and merging with contralateral pectoralis major muscle. (Arrow markers-1. Right Pectoralis Major Muscle 2. Left Pectoralis Major Muscle 3. Right Sternalis Muscle 4. Left sternalis Muscle 5. Criss Crossing of fibres of Sternalis Muscle)
Discussion
Presence of sternalis is quite a rare but normal anatomical variant of anterior chest wall musculature of human body. Cases have been reported by different authors with different names of this muscles i.e., Sternalis, Rectus thoracis, Presternalis, Muscularis sternalis, Parasternalis, Episternalis etc. This muscle has been described in both sexes with equal incidence. However, it has a variable frequency in different ethnic groups [1]. Many authors have assumed this muscle to be derived from neighboring muscles such as pectoralis major [2], rectus abdominis, sternocleidomastoid, external oblique [3] and panniculus carnosus [4]. Before labeling any superficial muscle in pectoral region as sternalis it should subserve the following parameters, it should be located between superficial fascia and deep fascia of pectoral region, its origin from sternum and insertion either into lower ribs, costal cartilages, rectus abdominis sheath or aponeurosis of external oblique muscle and innervated by either intercostals or pectoral nerves [5].
Out of all the above parameters, origin from the sternum is one of the main criteria for a muscle to be categorized as sternalis [6]. However, its position in the subcutaneous plane, insertion and innervations support its name sternalis.
Presence of sternalis can be explained embryologically from its nerve supply, if supplied by the pectoral nerves, it could originate from the pectoralis major and if by intercostal nerves than from the rectus abdominus muscle [6]. In the current case we were unable to find its innervation source. Its presence can also be explained depending on the arrangement of its muscle fibers, it could be an aberrant extension from the adjacent muscles or their blastemas which include the sternocleidomastoid muscle, rectus abdominis or external oblique. In the present case the muscle fibres are similar to fibers of external oblique and meeting with sternocleidomastoid muscle as previously reported [7,8]. Because of its location in superficial fascia it may be a remnant of panniculuscarnosus [4] which is also in favor of the present case. Various patterns of sternalis have been described by different authors by different names, by its location either unilateral or bilateral, or by attachment with sternocleidomastoid muscle of same side or opposite side.
Kumar MR Bhat reported a case of sternalis in a 60-year-old male cadaver that was oblique and about 12.3 cm long on left side whose cranial end was inserted into fibers of left pectoralis major muscle close to second costochondral junction and some fibers blend with sternal origin of sternocleidomastoid muscle and whose caudal end remained as panniculus carnosus [9]. Cherian SB and Gandhalam AJ reported a case of rectus sternalis muscle bilaterally in a 70-year-old female cadaver; 15 cm long, originated from the aponeurosis of external oblique muscle from 5th to 7th costal cartilages about 5cm from the midsternal line and extended cranially to blend with the sternal origin of the sternocleidomastoid. On both sides pectoralis major were normal [10]. The present case report is supported by all these above studies in bilateral occurrence, location, dimensions which can vary attachment with external oblique and pectoralis major muscle. Mehta V et al., reported a case of sternalis unilaterally in a 40-year-old male cadaver originating from external oblique which was fleshy throughout except at the ends where it was aponeurotic and had a “Y" shaped configuration at the sternal angle and later merged with respective sternocleidomastoid muscle. The muscle received its nerve supply from the third intercostal nerve [11]. This study matches with present case in location and attachment with nearby muscles but not with its unilateral presence.
Although an uncommonly described muscular variation, it merits a special mention in anatomical archives owing to its propensity to stimulate a soft tissue mass on radiological evaluation of pectoral region. It deserves a special mention in females because in breast carcinoma, depth of lymph nodes to be irradiated can also vary the presence of this muscle especially in inferomedial quadrant [12-14]. In addition, breast tissue extending deep to the sternalis muscle may be neglected during mastectomy [15]. This muscle can be used as muscle flap for reconstructions of anterior chest wall, head and neck and breast reconstructions [1,14]. Further this accessory muscle tissue can cause a myofascial pain in the chest wall located around the sternum and may radiate into the arm which is mild to moderate and is dull in nature. Sternalis syndrome is often confused with the pain of a heart attack. The diagnosis of sternalis syndrome is made by eliciting trigger points in the muscles of the chest wall by palpation [16].
If accidentally detected it should be mentioned in clinical records of the patient because muscular anomalies of the thoracic wall are associated with congenital anomalies like anencephaly and anomalies of adrenal gland [4] so it warrants documentation. If this muscle presents unilaterally and get hypertrophied it can lead to deviation of nipple areolar complex that may not be cosmetically acceptable. However, its presence may evoke alterations in the electrocardiogram and may cause breast or chest asymmetry [17,18].
Conclusion
The knowledge of this muscle variant will be of paramount importance to surgeons. This muscle can be mistaken for recurrence of malignancy of breast during CT, MRI and mammography especially during post treatment period. This accessory muscle should be known to clinicians so that they can make the patient understand about his clinical symptoms like chest asymmetry, myofascial pain, changes in mammograms and ECG etc. So, this has to be reported if present. Despite its diverse origin or incidence, it has hardly any biomechanical advantage or functional bearing, unless it assumes an enormous size replacing the congenitally absent pectoralis major.
[1]. Arráez-aybar LA, Sobrado-Perez J, Merida-Velasco JR, Left musculussternalisClin Anat 2003 16(4):350-54.10.1002/ca.1012012794922 [Google Scholar] [CrossRef] [PubMed]
[2]. Clemente CD, Gray’s anatomyIn: Muscle and fasciae 1985 30th edPhiladelphiaLea and Febiger [Google Scholar]
[3]. Sadler TW, Langmans Medical Embryology 2004 9th edBaltimoreLippincott Williams & Wilkins:199-209. [Google Scholar]
[4]. Harish K, Gopinath KS, Sternalis muscle: importance in surgery of the breastSurg Radiol Anat 2003 25(3-4):311-14.10.1007/s00276-003-0119-912898192 [Google Scholar] [CrossRef] [PubMed]
[5]. Jelev L, Georgiev G, Surchev L, The sternalis muscle in the Bulgarian population: classification of sternalesJ Anat 2001 199(3):359-63.10.1046/j.1469-7580.2001.19930359.x11554516 [Google Scholar] [CrossRef] [PubMed]
[6]. Loukas M, Bowers M, Hullett J, Sternalis muscle: a mystery stillFolia Morphol (Warsz) 2004 63(2):147-49. [Google Scholar]
[7]. Bailey PM, Tzarnas CD, The sternalis muscle: a normal finding encountered during breast surgeryPlast Reconstr Surg 1999 103(4):1189-90.10.1097/00006534-199904010-00013 [Google Scholar] [CrossRef]
[8]. Oneil MN, Folan-Curran J, Case report: Bilateral sternalis muscle with a bilateral pectoralis major anomalyJ Anat 1998 193(2):289-92.10.1046/j.1469-7580.1998.19320289.x9827645 [Google Scholar] [CrossRef] [PubMed]
[9]. Bhat KM, Potu BK, Gowda S, Sternalis muscle revisted in South Indian male cadaver: a case reportCases J 2009 2:631810.4076/1757-1626-2-6318 [Google Scholar] [CrossRef]
[10]. Cherian SB, Gandhalam AJ, Rectus sternalis muscle: An anatomical variant of anterior chest wallOA Anatomy 2014 2(2):16 [Google Scholar]
[11]. Mehta V, Arora J, Yadav Y, Suri RK, Rath G, Rectus thoracisbifurcalis: a new variant in the anterior chest wall musculatureRom J Morphol Embryol 2010 51(4):799-801. [Google Scholar]
[12]. Stines J, Tristant H, The normal breast and its variations in mammographyEur J Radiol 2005 54(1):26-36.10.1016/j.ejrad.2004.11.01715797291 [Google Scholar] [CrossRef] [PubMed]
[13]. Cawson JN, Papadopoulos T, Variants of sternal insertions of the pectoral muscle on mammography: a pictorial reviewClin Radiol 2002 57(6):442-48.10.1053/crad.2001.082812069458 [Google Scholar] [CrossRef] [PubMed]
[14]. Raikos A, Paraskevas GK, Tzika M, Faustmann P, Triaridis S, Kordali P, Sternalis muscle: an underestimated anterior chest wall anatomical variantJ Cardiothorac Surg 2011 6:7310.1186/1749-8090-6-7321575244 [Google Scholar] [CrossRef] [PubMed]
[15]. Young Lee B, Young Byun J, Hee Kim H, Sookkim H, Cho Mee S, Lee Hoo K, The sternalis muscles: incidence and imaging findings on MDCTJ Thorac Imaging 2006 21(3):179-83.10.1097/01.rti.0000208287.04490.db16915061 [Google Scholar] [CrossRef] [PubMed]
[16]. By Jonathan Aarons MD . Pain Management Comments. 2015 June 7 [Google Scholar]
[17]. Raikos A, Paraskevas GK, Yusuf F, Kordali P, Loannidis O, Saberi B, Sternalis muscle: a new crossed subtype, classification, and surgical applicationsAnn Plast Surg 2011 67(6):646-48.10.1097/SAP.0b013e31820d688b21407048 [Google Scholar] [CrossRef] [PubMed]
[18]. Khan UD, Use of the rectus sternalis in augmentation mammoplasty: case report and literature searchAesthetic Plast Surg 2008 32(1):21-24.10.1007/s00266-007-9046-117965818 [Google Scholar] [CrossRef] [PubMed]