Retroperitoneal Teratoma Mimicking Renal Calculus
Debansu Sarkar1, Arun Kumar Maurya2, Debasish Chakraborty3, Dilip Kumar Pal4
1 Associate Professor, Department of Urology, Institute of Post Graduate Medical Education and Research, SSKM Hospital, Kolkata, West Bengal, India.
2 Post Doctoral Trainee, Department of Urology, Institute of Post Graduate Medical Education and Research, SSKM Hospital, Kolkata, West Bengal, India.
3 Associate Professor, Department of Pathology, Institute of Post Graduate Medical Education and Research, Kolkata, West Bengal, India.
4 Professor, Department of Urology, Institute of Post Graduate Medical Education and Research, SSKM Hospital, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dilip Kumar Pal, Professor, Department of Urology, Institute of Post Graduate Medical Education and Research, SSKM Hospital, Kolkata-700020, West Bengal, India.
E-mail: urologyipgmer@gmail.com
Kidney stone, Mature teratoma, Sebaceous gland
A 16-year-old female with no prior health problem presented to us with complaint of pain in left flank for the past six months. She described the pain as intermittent, non radiating. No significant surgical or medical history was notified. On physical examination patient had soft abdomen, with no tenderness or palpable lump. Ultrasound (USG) revealed a heterogenous left upper polar cystic mass of 6×6 cm with a calculus at the end of cyst causing posterior acoustic shadow. A Contrast Enhanced Computerized Tomography (CECT) scan of the kidney, ureter and bladder revealed a cystic suspicious area with a shadow mimicking stone in upper pole moiety (at junction of bifid pelvis, Hounsfield Unit-118) [Table/Fig-1a,b]. The left adrenal gland not identified separately. Patient on evaluation was found to be non hypertensive, since mass was present in supra renal area plasma levels of aldosterone, cortisol, catecholamines, rennin, and adrenocorticotropic hormone were done which were found to be within the normal range. As per history and imaging study initially provisional diagnosis was of bifid pelvis with obstructed upper polar pelvicalyceal system by a calculus and a differential diagnosis of a nonfunctional adrenal mass with calcification or a retroperitoneal mass. Keeping these possibilities in mind open surgery was planned. Intraoperative mass was found to be adhering to the surrounding structures just lateral to inferior vena cava. Thick cheesy material came from mass [Table/Fig-2]. Carefully mass was dissected and removed. On histopathology, various sweat gland, sebaceous gland, cartilaginous structure was found [Table/Fig-3]. Till the write up of this case, patient visited us twice in 12 month interval without any signs of recurrence.
CECT scan of the kidney, ureter and bladder revealed a cystic mass found over the upper pole of right kidney having a hyperdense area near renal pelvis.(white arrows).

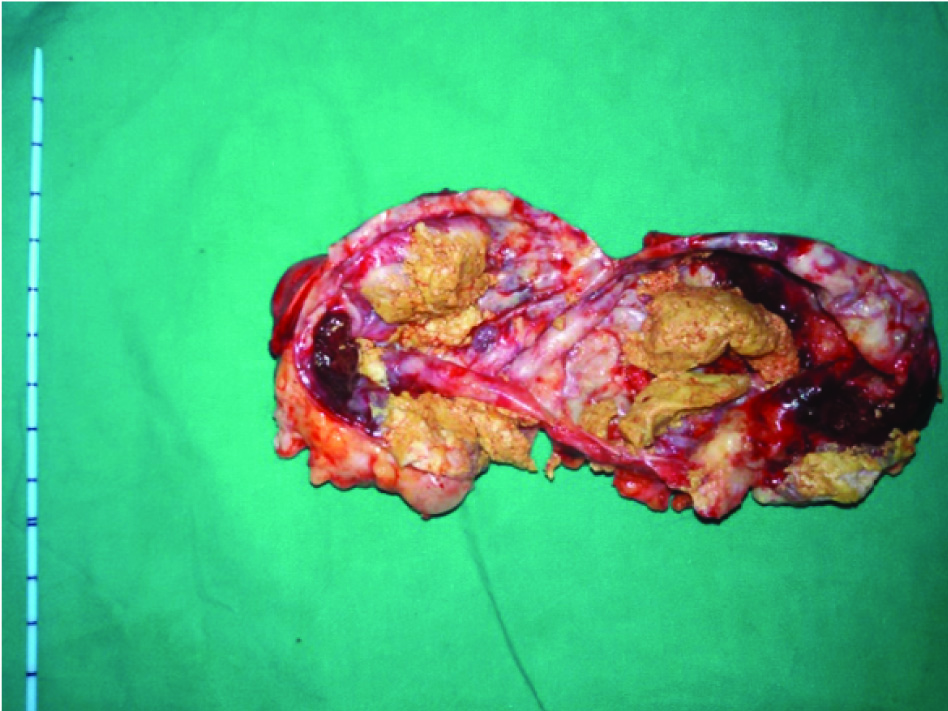
The mass showing thick cheesy material (characteristic feature of sebaceous gland).
Microscopic feature of mass matched with various tissues characterstics: A. Cartilaginous tissue, B. Sebaceous gland, C. Hair follicle and D. Adipose tissue [100X].

Teratomas are classified as mature and immature forms, immature teratomas are made up of more than one germ cell layers these lesions arise from pleuripotent malignant precursor cells [1]. The most common site for origin of teratomas is sacrococygeal region followed by ovary (29%). Retroperitoneal teratoma comprises 4% of all teratoma. It is most commonly found in younger population with female predominance [2]. Although there is no side predilection for retroperitoneal, but there are literature available which shows that the left side is more commonly involved [3]. In 50-60% cases of retroperitoneal teratomas calcification is present. However in this case site of calcification, presence of cyst and ipsilateral non visualization of adrenal gland has produced the entire diagnostic dilemma. In literature teratoma arising from kidney and adrenal gland are rare [4-6]. Teratomas can be solid or cystic. Solid lesions are more commonly malignant and predominantly found in adults. Surgical excision followed by histopathological examination is the mode of choice for diagnosis and treatment of teratomas as they are chemo and radioresistant in nature [7]. Sometimes imaging study did not lead us to a concrete diagnosis in that scenario it is always better to go with open surgery with all possibilities in mind.
[1]. Shanmughapriya S, SenthilKumar G, Balakrishnan K, Vasanthi N, Vinodhini K, Natarajaseenivasan K, Bilateral ovarian teratoma complicated with carcinosarcoma in a 68 year old woman: a case reportBMC Cancer 2011 11:21810.1186/1471-2407-11-21821639901 [Google Scholar] [CrossRef] [PubMed]
[2]. Grosfeld JL, Billmire DF, Teratomas in infancy and childhoodCurr Probl Cancer 1985 9(9):01-53.10.1016/S0147-0272(85)80031-3 [Google Scholar] [CrossRef]
[3]. Chaudhary A, Misra S, Wakhlu A, Tandon RK, Wakhlu AK, Retroperitoneal teratomas in childrenIndian J Pediatr 2006 73(3):221-23.10.1007/BF0282548516567916 [Google Scholar] [CrossRef] [PubMed]
[4]. Nirmal TJ, Krishnamoorthy S, Korula A, Primary intrarenal teratoma in an adult: A case report and review of literatureIndian J Urol 2009 25(3):404-06.10.4103/0970-1591.5618419881142 [Google Scholar] [CrossRef] [PubMed]
[5]. Lam KY, Lo CY, Teratoma in the region of adrenal gland: A unique entity masquerading as lipomatous adrenal tumorSurgery 1999 126:90-94.10.1067/msy.1999.9892410418600 [Google Scholar] [CrossRef] [PubMed]
[6]. Yavuz A, Ceken K, Alimoglu E, Akkaya B, Mature cystic renal teratomaIranian Journal of Radiology 2014 11(1):e1126010.5812/iranjradiol.11260PMC3955850 [Google Scholar] [CrossRef] [PubMed]
[7]. Mikio K, Yoshio T, Noriyoshi S, Junichi W, Primary retroperitoneal teratoma in an adult: a case reportInternational Journal of Urology 1997 4:219-21.10.1111/j.1442-2042.1997.tb00175.x9179701 [Google Scholar] [CrossRef] [PubMed]