Fistulotomy Around The Sphincter (FATS) Procedure: A Simple New Sphincter-Sparing Concept to Treat High Fistula-In-Ano
Pankaj Garg1
1 Senior Consultant, Department of Colorectal Surgery, Indus Super Specialty Hospital, Mohali, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pankaj Garg, Garg Fistula Research Institute, 1041/15, Panchkula-134113, Haryana, India.
E-mail: drgargpankaj@yahoo.com
Fistulotomy Around The Sphincter (FATS) is a novel sphincter sparing procedure for high anal fistulas. In FATS procedure, the fistula tract from internal opening to external opening is laid open except that the sphincter complex is not cut and is completely preserved. The fistula tract passing through the sphincter complex (TISC-Tract Inside Sphincter Complex) is thoroughly cleaned, curetted and debrided but is not widened. The final wound should form a double cone, one each at internal as well as external opening. The wide end of the cone should be at the mucosa and the skin respectively whereas TISC should form the tip of both the cones. The wound heals by secondary intention (granulation tissue). The aim is that TISC heals first. Subsequently, both the wounds at the internal and the external openings heal, from TISC towards the respective openings. This article is about three patients with high fistula-in-ano in whom FATS was done. All of the three patients were males with a mean age of 43.0±0.5 years and with a median follow-up of 8 months. The fistula healed in all patients with no change in incontinence scores (Vaizy’s incontinence scores). FATS is a simple and effective novel sphincter-sparing procedure to treat high fistula-in-ano especially with wide internal opening.
Anal fistula, Fecal incontinence, Recurrence
Case Series
High fistula-in-ano (which involve more than one-third of sphincter complex) pose a therapeutic challenge. The conventional sphincter cutting procedures like fistulotomy and cutting seton (ksarsutra) entail a high risk of incontinence in such patients [1,2]. Newer sphincter-sparing procedures are usually recommended for such fistulas [1-5]. However, if these high fistulas get associated with wide internal opening (caused by injudicious use of cutting seton), then even the newer sphincter-sparing procedures become ineffective in these fistulas making their treatment even more challenging. In these difficult fistulas (high fistulas with wide internal opening), FATS procedure seems to be an effective sphincter-sparing procedure. The experience of FATS procedure in three patients is being described.
Case-A
A 55-year-old male presented with regular pus discharge due to recurrent fistula operated three times earlier over a period of five years. He had undergone a tightening seton procedure (ksarsutra) by an ayurvedic doctor. Due to this, the whole tract in right posterior region had been partially cut leading to widening of external as well as the internal opening [Table/Fig-1,2]. The tract was involving more than 75% sphincter complex and was graded as per different classifications [1].
a) (left panel): Preoperative, b) (middle panel): Immediate postoperative c) (right panel): Postoperative (6 weeks) photographs of a FATS procedure in a 55-year-old man (Patient A) with recurrent high fistula (involving more than 75% of sphincter complex).

The schematic diagram and MRI images (coronal & axial) of a 55-year-old man (Patient A) with recurrent high fistula (involving more than 75% of sphincter complex).

Case-B
A 53-year-old male presented with episodic pus discharge due to recurrent fistula operated two times earlier over a period of three years. He had undergone a fistulectomy and a tightening seton procedure (ksarsutra). There was a wide tract in left posterior region and a wide internal opening [Table/Fig-3,4]. The tract was very high involving more than 80% sphincter complex and was graded as per different classifications [Table/Fig-5].
a) (upper panels): Preoperative, b) (lower left panel): Immediate postoperative, c) (lower right panel): postoperative (6 weeks) photographs of FATS procedure: in a 53-year-old man (Patient B) with high fistula (involving more than 80% of sphincter complex). He had a wide internal opening and no external opening.

The schematic diagram and preoperative and postoperative MRI images (coronal & axial) of a 53-year-old man (Patient B) with a high fistula (involving more than 80% of sphincter complex). He had a wide internal opening and no external opening.
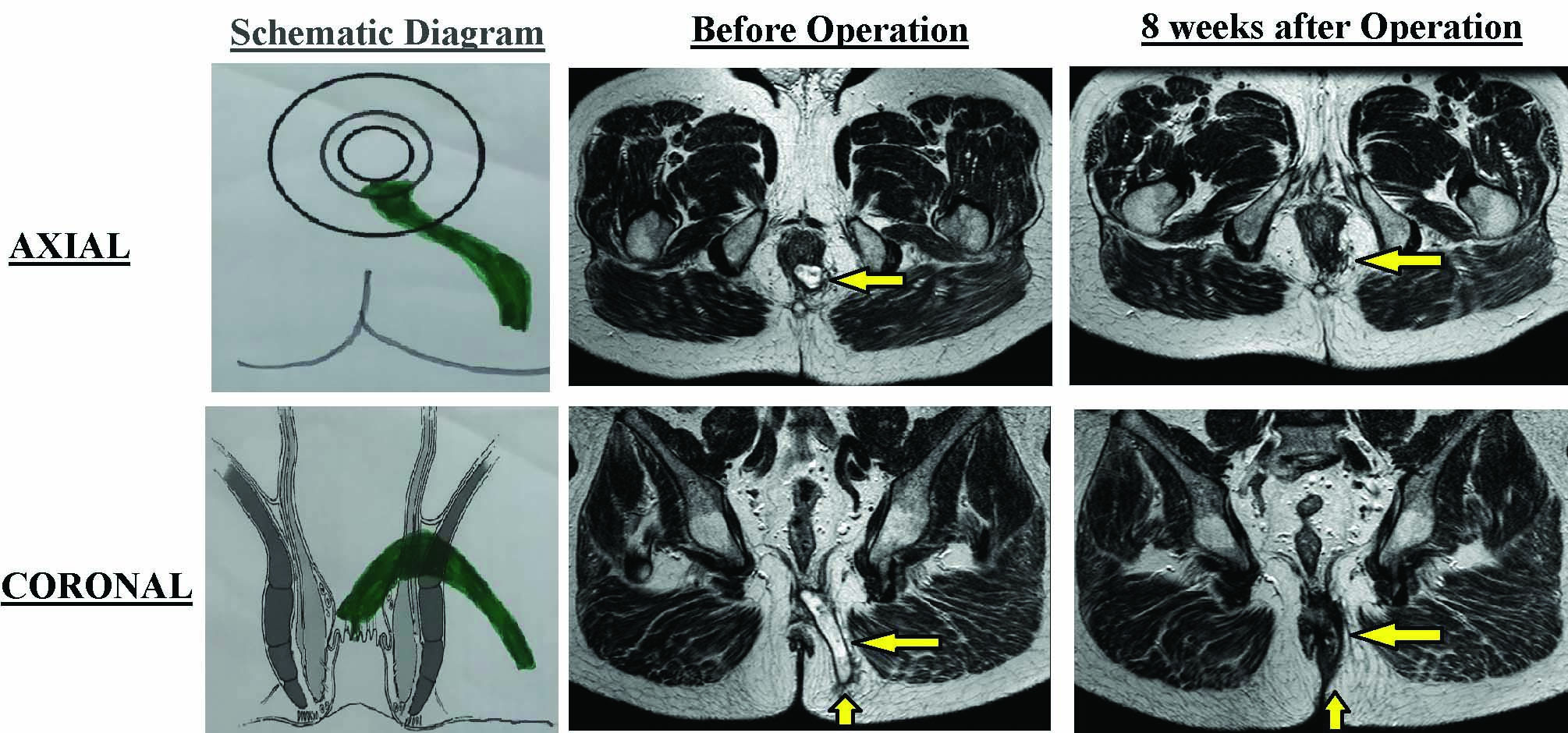
Table comparing the characteristics of the patients included in case-series.
| Patient A | Patient B | Patient C |
|---|
| Age/Sex | 55 yr/Male | 53 yr/ Male | 55 yr/Male |
| Previous Operations | Operated 3 times earlier | Operated 2 times earlier | Operated once earlier |
| Location of fistula | Right Posterior | Left Posterior | Left Anterior |
| High/Low (Amount of Sphincter involvement) | High (75% Sphincter involved) | High (80% Sphincter involved) | High (75% Sphincter involved) |
| External Opening | 7 o’clock | Nil | 1 o’clock |
| Internal Opening | 6 o’clock | 6 o’clock | 12 o’clock |
| Number of Tracts | 1 | 1 | 1 |
| Classification | | | |
| Park’s | II | II | II |
| St James University Hospital | III | III | III |
| Garg’s | III | III | III |
Case-C
A 55-year-old male suffering from a recurrent complex fistula-in-ano had history of continuous pus discharge for several weeks. He had undergone a coring out of fistula tract with an advancement flap procedure six month back. The internal opening was widened; the tract was involving more than 75% sphincter complex and was graded as per different classifications [Table/Fig-5].
Due to wide internal opening and high fistula, all these three patients were unfit for fistulotomy, Anal Fistula Plug (AFP) procedure [2], ligation of Intersphincteric Fistula Tract (LIFT) [3], Video-Assisted Anal Fistula Procedure (VAAFT) [4], advancement flap and PERFACT procedure [5]. FATS procedure was carried out in these patients. The wound was cleaned regularly (at least twice daily) in the post operative period. Vaizey’s incontinence scores were evaluated preoperatively and postoperatively at 6 weeks [6]. All the patients were followed for 8 months (median). All three patients recovered well after the procedure with complete healing of the fistula tracts. There was no change in incontinence scores (Vaizey’s scores). In one patient (patient-B), a postoperative MRI was also done to confirm the healing of the fistula tracts [Table/Fig-4].
Discussion
High fistula-in-ano is difficult to treat and there is a significant risk of incontinence with conventional methods. Cutting seton (ksarsutra) is not indicated to treat high fistulas as the risk of incontinence is high. However, routine use of cutting seton even in high fistulas leads to widening of internal opening. This makes the treatment of such partially treated high fistula even more difficult.
FATS procedure is a new procedure which has not been described in the literature. In this, the fistula tract is laid open from the internal opening to the external opening while completely preserving the sphincter complex. Due to this, there is minimal risk of incontinence. In fistulotomy with primary sphincter reconstruction (FPR) procedure, the fistula tract is excised, the sphincter complex is cut and then the sphincter is repaired (sutured back). In FPR, though the sphincter is repaired, yet there is always some risk of sphincter repair failure (dehiscence) which can have serious consequences. The intention behind cutting the sphincter is to effectively remove the fistula tract [7,8].
In FATS, the aim is to achieve the same result as FPR (to effectively remove the fistula tract) in such a way so that the steps of cutting and immediately repairing the sphincter could be omitted. Hence the risk of sphincter repair failure (dehiscence) is negated. The incision is given as in conventional fistulotomy. The incision joins the external and the internal opening. The incision starts a small distance beyond (lateral to) the external opening [Table/Fig-6]. The external opening, perianal skin and the internal opening are incised. The incision extends slightly beyond the internal opening. The incision is deepened till the level of the sphincters [Table/Fig-6]. The sphincter complex (internal plus external sphincter) is not cut and is completely preserved. The fistula tract, including the part passing through the sphincter complex, is thoroughly cleaned, curetted and debrided. A finger is kept in the rectum while curetting the tract to prevent accidental injury to the rectum.
The concept of FATS procedure (Drawn by author).

It is important that the fistula tract passing through the sphincter complex (TISC- tract in sphincter complex) is curetted and cleaned but is not widened. This is vital as TISC should heal before the healing of outer and inner parts of the fistula tract. Subsequently, the wounds around the internal and the external openings heal from TISC towards the openings. The operative wound should form two inverted cones with TISC forming the conical part (tip) of both the cones. The wide end of the cone should be at the mucosa and the skin respectively [Table/Fig-6]. The aim is that TISC heals first. The whole wound heals by secondary intention (granulation tissue).
The fecal matter or the mucus usually doesn’t pass through the wound as the TISC is the narrowest part of the wound and is kept collapsed by sphincter muscle pressure.
As demonstrated in the present study, the three patients suffering from high anal fistula and a wide internal (primary) opening underwent FATS procedure. The fistula in all the patients healed totally in three months with complete resolution of all the fistula tracts. In one patient (patient B), the healing was even demonstrated on a postoperative MRI scan [Table/Fig-4]. Along with complete healing, there was no change or deterioration in continence levels in any of the patients, as measured objectively by Vaizey’s incontinence scores [6]. The procedure was minimally morbid as all the patients could resume their normal daily activities within 48 hours of the surgery.
Other procedures when attempted in similar high anal fistula would lead to either high incontinence rates or much lower success rates. Fistulotomy done in such high fistulas would lead to unacceptably high risk of incontinence [9]. Therefore, fistulotomy should not be attempted in such high fistulas. The newer sphincter sparing procedures like LIFT, VAAFT and Anal Fistula Plug would lead to high failure rates in such fistulas with wide internal opening [2-4]. FATS is technically as simple as is fistulotomy [9] and doesn’t require costly gadgets as in VAAFT or Plug procedure [2,4].
FATS procedure is quite similar to fistulotomy with primary sphincter reconstruction (FPR) except that the sphincter is not cut and repaired. Therefore, it is much safer as there is no risk of secondary infection leading to wound dehiscence and subsequent danger of incontinence. The morbidity is also less in FATS as compared to FPR. FATS procedure is also better than fistulotomy as the sphincter complex is completely preserved. FATS is a novel procedure which has not been described in the literature before.
Conclusion
FATS procedure seems effective in patients suffering from high fistula-in-ano especially with wide internal opening. However, long term results in larger number of patients are needed to confirm these observations.
[1]. Garg P, Comparing existing classifications of fistula-in-ano in 440 operated patients: Is it time for a new classification?Int J Surg 2017 42:34-40.10.1016/j.ijsu.2017.04.01928414118 [Google Scholar] [CrossRef] [PubMed]
[2]. Garg P, Song J, Bhatia A, Kalia H, Menon G, The efficacy of anal fistula plug in fistula-in-ano: a systematic reviewColorectal Dis 2010 12:965-70.10.1111/j.1463-1318.2009.01933.x19438881 [Google Scholar] [CrossRef] [PubMed]
[3]. Hong KD, Kang S, Kalaskar S, Wexner SD, Ligation of intersphincteric fistula tract (LIFT) to treat anal fistula: systematic review and meta-analysisTech Coloproctol 2014 18:685-91.10.1007/s10151-014-1183-324957361 [Google Scholar] [CrossRef] [PubMed]
[4]. Garg P, Singh P, Video Assisted Anal Fistula Treatment (VAAFT) in Cryptoglandular fistula-in-ano: A systematic review and proportional meta-analysisInt J Surg 2017 46:85-91.10.1016/j.ijsu.2017.08.58228882770 [Google Scholar] [CrossRef] [PubMed]
[5]. Garg P, Garg M, PERFACT procedure: a new concept to treat highly complex anal fistulaWorld J Gastroenterol 2015 21:4020-29.10.3748/wjg.v21.i13.402025852290 [Google Scholar] [CrossRef] [PubMed]
[6]. Vaizey CJ, Carapeti E, Cahill JA, Kamm MA, Prospective comparison of faecal incontinence grading systemsGut 1999 44:77-80.10.1136/gut.44.1.779862829 [Google Scholar] [CrossRef] [PubMed]
[7]. Ratto C, Litta F, Donisi L, Parello A, Fistulotomy or fistulectomy and primary sphincteroplasty for anal fistula (FIPS): a systematic reviewTech Coloproctol 2015 19:391-400.10.1007/s10151-015-1323-426062740 [Google Scholar] [CrossRef] [PubMed]
[8]. Arroyo A, Perez-Legaz J, Moya P, Armananzas L, Lacueva J, Perez-Vicente F, Fistulotomy and sphincter reconstruction in the treatment of complex fistula-in-ano: long-term clinical and manometric resultsAnn Surg 2012 255:935-39.10.1097/SLA.0b013e31824e911222504192 [Google Scholar] [CrossRef] [PubMed]
[9]. Abramowitz L, Soudan D, Souffran M, Bouchard D, Castinel A, Suduca JM, The outcome of fistulotomy for anal fistula at 1 year: a prospective multicentre French studyColorectal Dis 2016 18:279-85.10.1111/codi.1312126382623 [Google Scholar] [CrossRef] [PubMed]