T2DM is a metabolic disorder, with multiple causative factors, in which chronic hyperglycaemia and fat, carbohydrate and protein metabolism disturbances are seen [1]. Diabetes has become a global issue and epidemiological evidence suggests that effective control and prevention programmes are necessary to prevent escalation of the global diabetes burden [2,3].
Diabetes is a major non-communicable disease which is reducing national and individual productivity and can have serious negative implications on the economies of developing and developed nations [4]. The rapid rise in population, aging, urbanization and increasing prevalence of obesity and physical inactivity is a major reason for surge in the number of people suffering from diabetes [5]. Area of adiposity also has significance in the severity of risk factors, people with abdominal obesity being more prone for developing T2DM [6].
It is well known fact supported with various studies that, exercise plays a key role in promoting health. On comparison to the prescribed physical activity guidelines given by United States Centre for Disease Control, for adult age group of 18 years and over, it is found that only 49.2% of them met the aerobic exercise and just 20.8% are up to the level considering aerobic and anaerobic exercise [7-9]. In general, the common advice on exercise to general public with diabetes and other Non-Communicable Diseases (NCDs) is to adopt an increase in Physical Activity (PA). The prescription of exercise by physical therapists and other exercise related professionals does follow the FITT principle (Frequency, Intensity, Time and Type), but they fail to prescribe a problem specific exercise regimen for controlling diabetes and other NCDs [10]. A study states that family physicians interested in prescribing lifestyle medicine to improve health behaviours and decrease the impact of chronic diseases must be trained in it [11].
For the people suffering from diabetes, selecting an appropriate form of PA to address their needs poses a problem, and most of them are not sure what type of PA will help them to control diabetes. An extensive search for an exercise which takes into consideration all the factors which can influence NCDs and their control through physical exercise led the authors to zero in on exercise for the abdominal muscles. It has been proven that abdominal obesity, as measured by the waist hip ratio, has direct link with development of T2DM and to the degree of insulin resistance seen in people with T2DM [12-14].
Despite acknowledgement of the importance of abdominals and research on various aspects of abdominal muscles and its anatomical and physiological functions, the influence of training of the abdominal muscles on diabetes has not been studied with due importance. With the available background on the exercises and abdominals on diabetes, it is evident that there are no established abdominal training protocols to address diabetes as well as no common exercise to cater to people of varying age group and economic backgrounds.
The need of one exercise protocol that considered all the factors which influenced adherence of people who performed it, namely, cost, duration, equipment required, feasibility and need for monitoring, was recognised. As an attempt to design such an effective and practical exercise protocol, an abdominal exercise program named ABON was designed and validated [15]. The abdominal training program ABON was designed by the principal investigator (SSG, a physical therapist) and its efficiency tested on a pilot study, which established the effectiveness of the abdominal training program in reducing body weight and decreasing blood pressure [15]. There was no similar protocol of abdominal strengthening available in the literature which could be expected to have an effect on diabetes.
This study incorporates an attempt to study such a dynamic, prospectively effective protocol that has influence on abdominal obesity, blood pressure and blood glucose levels which consider specificity, less time spent working out, simplicity to follow and cost effectiveness in promoting health. Elevated blood pressure, abdominal obesity and high blood sugar are seen to be closely interrelated. Since it was seen that the ABON has a positive effect on obesity and high blood pressure [15], the present study aimed to study the effect of the abdominal training program on blood glucose levels, and compare it with the effect of other general exercises.
Materials and Methods
A pre- post experimental trial was designed in which 100 participants who fulfilled the inclusion criteria were identified from the faculty, post graduate students and general public attending physiotherapy at Vels University, Chennai, India. The trial was conducted during the time period from October 2014 to March 2016. Ethical clearance was obtained from Institutional Ethical Committee, Vels University. The candidates were given a briefing about the study purpose and procedure and signature was obtained on an informed consent form. The study included type 2 diabetics of both gender with age group of 25 to 45 years, males with a waist hip ratio more than 0.96 and females with waist hip ratio more than 0.81 [16], those with abdominal muscle weakness of grade 4 and below in Manual Muscle Testing (MMT) [17], elevated fasting blood sugar of 126 mg/dL and above [18] and systolic blood pressure >120 mmHg and diastolic >80 mmHg [16]. Subjects with Type 1 diabetes mellitus, acute abdominal muscle injury or pain, abdominal or inguinal hernia, spinal conditions or low back ache and pregnancy, subjects with any medication for weight loss or participating in any regular fitness programme were not included for the study. The study is represented in the following [Table/Fig-1], explaining the stages of selection to exit by the experimental and control group.
Consort (Consolidated Standards of Reportng Trials) diagram showing th flow chart of prgress of participants through the stages of the study.
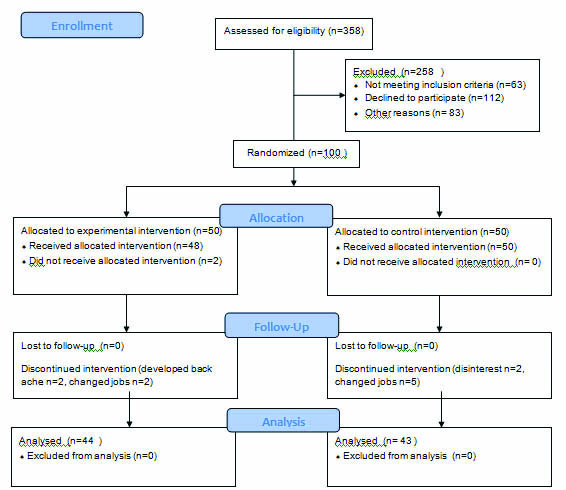
The subjects were randomly divided into two equal groups, 50 subject in control group and 50 subjects in experimental group, using a lottery system. Subjects in both the groups underwent a supervised training program for 30 minutes a day, three days a week, for duration of 12 weeks during the department working hours 8 AM to 3 PM. Experimental Group (A) underwent a regular ABON designed by the team of experts in the study which included leg raise, abdominal tucks, quadruped abdominal crush, breathing training and abdominal grading exercises according to the grade of the abdominal muscles and in addition to it, warm-ups, stretches and active extremity exercises were prescribed. The exercise was done for 15-30 minutes a day (depending on individual variation in finishing the sets), three times a week for 12 weeks. The intensity of each exercise was progressed from eight repetitions to 12 to 15 repetitions every fourth week. The subjects in the experimental group were also encouraged to do walking for 40 minutes a day and continue their regular lifestyle. The control group (B) were instructed not to involve in any form of abdominal muscle training for three months. They were also instructed on a home program consisting of breathing exercises, general body stretches that was for a total duration of 15 minutes. They were also encouraged to do walking and continue regular lifestyle. The outcome measures were random blood glucose and HbA1C obtained using the HPLC method, which were measured at baseline and at the end of the treatment duration and subjected to statistical analysis. The HPLC method is a rapid, precise method of assessing HbA1c which is considered the gold standard method for determination of HbA1c. It has the advantage of using a relatively small amount of sample and can be done in an automated manner [19]. Overall participation was 84.5% with 16 dropouts due to various reasons and the groups ended up with a sample size of 44 in the experimental and 43 in the control group.
Outcome Measures
Random Blood Glucose (RBS): It was measured by the Accu-Chek® Aviva glucometer, a standard brand which tests blood sugar by blood samples taken by fingertip needle prick and test strips. The procedure and recordings were done by a qualified nurse.
HbA1C: The HPLC method [19] was used to estimate the HBA1c levels [13]. Values were taken twice, once before and once after completing the exercise program, at the end of twelve weeks.
Description of Interventions
Experimental Group (A): The exercise protocol included general body stretches, pelvic correction and an Abdominal training program ABON [15] that consist of following exercises:
Abdominal tucks: In standing position, contracting the abdominal muscles so that the navel is pulled towards the spine. This is done initially for three sets of 10 repetitions each and progressed up to five sets of 25 repetitions each.
Leg raises: In supine position, the lower limbs are raised together to 30-40 degrees of flexion and lower it without touching the supporting surface and repeat to the prescribed number. These exercises are also done initially for three sets of 10 repetitions each, and progressed to 25 repetitions done for five sets.
Quadruped abdominal crush: Starting from standing with arms by the side and feet together, the subject bends forward without bending the knees, and places hands on the ground firmly as close as possible to the knees. Then a rocking movement is done as if shifting the body weight alternatively from leg to hand, carefully avoiding breath holding. Two sets of this exercise are done with 25 repetitions each.
Breathing training: In a sitting position, the subject takes in a few relaxed breaths, then takes a deep inhalation and holds it for a maximum of 10 seconds, then exhale. This is done for approximately four times per minute and continued for three minutes. A timer is used for guidance till the timing is learnt by the subject.
Abdominal grading exercises (Kendall’s) [20]: The exercises used for grading the abdominal muscles from grade 1 to 5 as given by Kendall were given according to the grade of the respective subject’s abdominal muscles. The starting position was crook lying, with pelvis neutral, and care was taken to avoid breath holding. Initially three sets of 10 repetitions were done, and progression was done with increments of two repetitions each up to 16 repetitions in a set. The exercise is changed and progressed with increasing strength up to grade 5.
Control Group (B): The subjects in the control group were given the following exercises under supervision:
Breathing exercises: In sitting position, the subject takes a deep breath through the nose, holds for a few seconds and blows out through the nose. The normal inspiration to expiration ratio is maintained, and the exercise repeated five times.
Pelvic correction: In a standing or supine lying position, the pelvis is tried to be maintained in neutral for as long as possible, avoiding breath holding.
General body exercise and stretches: The stretches are done in a suitable adaptation of the standing position. Three stretches with a hold time of five seconds is done for the following muscles: sternocleidomastoid, deltoids, biceps, triceps, long flexors of wrist, and extensors of wrist, quadriceps, hamstrings and calf muscles.
Warm up and cool down exercises: It involves active range of movement exercises to the neck, spine and limb joints, done for three repetitions in a relaxed manner.
Statistical Analysis
The data collected pre and post study duration from both the groups were analysed statistically using StatistiXL Version 2.0 and Stats Direct Statistical Analysis Software. The Wilcoxon signed rank test was applied to compare the scores within the groups, and to compare between the scores of control group and experimental group, the Mann- Whitney two tailed test was used. A p-value of < 0.01 was considered to be significant.
Results
The results of the Wilcoxon signed rank test show that the experimental group A had a significant difference (p=0.000) in both RBS and HbA1c when the values before and after treatment were compared [Table/Fig-2]. This difference was not observed (p=0.200) in the control group [Table/Fig-3].
Pre- post difference of RBS in both the groups.
| Group | Pre median | Post median | t | p |
|---|
| A | 146.000 | 120.000 | 0.000 | <0.01 |
| B | 163.500 | 153.000 | 383.500 | 0.200 |
Wilcoxon Signed Rank test was used to compare scores of each group before and after treatment. A p-value of <0.01 was considered to be significant.
Pre- post difference of HbA1C in the groups.
| Group | Pre Median | Post Median | t | p |
|---|
| A | 6.7 | 5.9 | 0.000 | 0.01 |
| B | 7.250 | 7.050 | 273 | 0.118 |
A p-value of <0.01 was considered to be significant.
[Table/Fig-4,5] show the comparison of the difference in values of HbA1c and RBS values between the two groups using the Mann-Whitney U test. There was a significantly higher improvement seen in the experimental group in both the outcome measures when the differences before and after treatment were compared (p< 0.01).
Comparison of difference in pre- post HbA1C between the groups.
| Group | Median | U | p |
|---|
| A | 10.000 | 1859.500 | <0.01 |
| B | 1.252 |
Mann-Whitney U test was used. A p-value of <0.01 was considered to be significant.
Comparison of difference of pre- post RBS between both groups.
| Group | Median | U | p |
|---|
| A | 14.615 | 1836.000 | <0.01 |
| B | 1.806 |
Mann-Whitney U test was used. A p-value of <0.01 was considered to be significant.
Discussion
The results of the present study show that the subjects who underwent an abdominal muscle training program ABON of 12 weeks duration, designed by the authors had significant reduction in random blood sugar and glycosylated haemoglobin when compared with a control group. The abdominal muscles are major core muscles of the human body whose main functions are trunk stabilization and maintenance of intra- abdominal pressure. It is understood well that the abdominal muscle has to be maintained in optimal strength to maintain general health [20].
Abdominal exercises are used in sports and various therapeutic regimens for varying conditions. Previous study has discussed the need for conservational training programs on core muscles including abdominals to manage sports hernias [21]. Others have found that training of the trunk muscles including the abdominal muscles can play a major role in improving the performance of many daily living activities [22]. The present study has attempted a new initiative focussing on the role of an abdominal training program on blood glucose levels in young individuals.
From a study of the available literature, the benefits of exercises are doubtless, but the problem appears to be one of plenty, where there are multiple studies available about the efficacy and the dosage for appropriate effects of a number of exercises interventions. The only consensus seems to be the one stated by Chris A, that “some exercise is better than none, and more is better than less” [23].
This abdominal training program ABON gives an alternate thought to exercise intervention and help attain all the health benefits of exercise with ease. The results of the present study show a marked reduction in the blood glucose levels and HbA1c values in the subjects who underwent the abdominal muscle training program when compared to those who underwent a general exercise program. ABON being a forerunner of its kind, specifically trains the core muscles in such a way that the efficiency of the muscle and its dependent or interrelated functions are enhanced by a mechanism yet to be ascertained. The other direct and indirect mechanisms like efficient glucose disposal, mitochondrial biogenesis, sensitivity of muscle to insulin, reduction in blood pressure and abdominal obesity could also be a possible reason for the outcome of the study.
Blood glucose levels are related to blood pressure and abdominal obesity, and an abdominal muscle training program can influence blood glucose levels indirectly by decreasing blood pressure and abdominal obesity. Ross R et al., on studying the effect of varying amount and intensity of exercise on abdominal obesity and glucose tolerance has found that exercises, especially high intensity exercises, are effective in reducing abdominal obesity and improving glucose tolerance [8]. Bohm A et al., have stated that exercise is widely accepted and recommended as a key prevention strategy for diabetes throughout the world [24].
Exercise training improves glucose disposal in the body by a number of non- muscle adapatations such as enhanced capillarization, increase in muscle mass, mitochondrial biogenesis and changes of muscle fibres from one type to another. Changes also occur at a molecular level, some of which are attributed to increased abundance of proteins which are important in uptake and oxidation of fatty acids and glucose. There are also seen altered post translational modifications of these same proteins [25]. Exercise training programs are also known to improve the sensitivity of muscles, especially skeletal muscles to insulin [26]. It is also found that aerobic exercise increases insulin binding to the receptors of monocytes, which in turn causes higher production of insulin and thus greater glucose absorption, and finally reduces the blood sugar level. Exercise enhances the capillary bed and increases the number of insulin receptors. Since working muscles are more sensitive to insulin than resting muscles, each unit of insulin will cause more glucose absorption during exercise. This reduces blood sugar, especially in mild- to moderate-intensity exercises. Thus, aerobic exercises, which are safe and easy, can increase insulin sensitivity and decrease insulin resistance [27].
The study was designed specifically targeting people who are not able to invest time and money and have limited access to health centres but yet wish to gain health benefits of exercise and thereby control diabetes mellitus. In addition, many people with diabetes mellitus find it difficult to perform weight bearing exercises due to involvement of the foot in the form of sensation loss or ulcers. The exercise program tested in this study was simple in terms of frequency, intensity, time, accessibility and posed little or no financial burden. The dropouts in the study were minimal and no one had discontinued citing any of the reasons above. The design of the exercise program was unique in attempting a practical solution that can be universally practiced to promote general health and control diabetes.
Based on the available resources on abdominal exercises the abdominal training program ABON was carefully carved out so that it specifically influences the blood glucose. It was also designed in such a way that it could be practiced with ease by people of all age groups, without being considered a burden and adhered to even after the study period. It is also economical in terms of cost, since it does not require any expensive equipment and once learnt, can be practiced without being monitored. The time and ease of practice at their comfortable space and pace will make it more feasible to be adopted by people of all walks of life there by influencing the lifestyle and promoting physical activity level.
The authors hope that the results of this study was useful for those looking for a specific exercise protocol which can be useful for managing type 2 diabetes mellitus. Further studies should explore the different variables which influence the efficiency of this exercise protocol in controlling diabetes mellitus.
Limitation
The relatively big number of dropouts, since the availability of samples for long term follow up demanded tedious efforts, and the wide age range of the participants. The effect of medications and duration of diabetes was not considered.
Conclusion
The ABON was effective in decreasing blood glucose levels in people with raised blood glucose levels, hypertension and abdominal obesity and weakness. The authors recommend the ABON as a simple and effective way to control blood glucose levels in people suffering from type 2 diabetes mellitus.
Wilcoxon Signed Rank test was used to compare scores of each group before and after treatment. A p-value of <0.01 was considered to be significant.
A p-value of <0.01 was considered to be significant.
Mann-Whitney U test was used. A p-value of <0.01 was considered to be significant.
Mann-Whitney U test was used. A p-value of <0.01 was considered to be significant.