Aesthetics is the most desirable quality giving a feeling of contentment to all people around the world. Now a days, a rapidly growing interest is seen for the smile aesthetics [1]. Smile aesthetics is influenced by various factors such as lip position, gingival display, colour, shape, position and visibility of teeth, and teeth arrangement of the dentition especially anterior teeth alignment [2]. To create beautiful smiles, understanding the associated factors is of utmost importance. Gingival display is one of the most important variables considered during smile analysis [3,4]. If there is excessive gingival display or gummy smile, it may lead to unpleasing smile. There exists different views regarding the acceptable amount of gingival display in previous studies [3,5,6].
The importance has also been given to the incisor arrangement to analyse the smile aesthetics. A person’s smile is mostly influenced by the labiolingual inclination (proclination/retroclination) and the incisor flare [7]. Now a days, the value for improving aesthetics has risen rapidly rather than seeking of orthodontic treatment just for the sake of functional advantage, as it used to be earlier. According to the reports from study conducted by Baldwin DC, the desire to improve appearance is the most important factor for the adult patients to get motivated for orthodontic treatment [8]. Hence, orthodontists need to be aware about the facial/dental aesthetics and current public fondness for beauty.
Increased gingival display is not perceived as unaesthetic by the general public. It is documented in previous study that most of the women, models and actresses were believed to be quite beautiful and good looking even though they displayed their gingiva while smiling [9]. In the study conducted by Kokich VO et al., they reported that the distance of 3 mm from gingiva was considered unpleasing by lay person and orthodontists [10]. Aesthetic insight being a subjective entity varies from one individual to another. Moreover, the considerable distinguishing features between pleasant and unpleasant smile are difficult to appreciate especially for the people who do not have any knowledge regarding ideal oral structures. Knowing such features would help the orthodontists in proper diagnosis and treatment and ultimately yield satisfactory results at accomplishment of the treatment.
Limited number of studies, evaluating the perception about the effect of gingival display on incisor inclination, was found in dental literature [5-7]. Hence, a study was carried out in Saudi Arabia, to assess the aesthetic perceptions of dentists, orthodontist and lay persons regarding the effect of gingival display on the incisor inclination.
Materials and Methods
An observational, cross-sectional questionnaire based study was carried out among orthodontists, general dentists and lay persons in Riyadh, Saudi Arabia for a period of five months, from September 2015 to January 2016. Prior to the conduct of the study, ethical clearance was obtained from the Review Board and Ethics Committee of Riyadh Colleges of Dentistry and Pharmacy (RCsDP), Riyadh, Saudi Arabia (Registration number FPGRP/43434001/121).
The sample size of 30 per group was calculated based on an alpha significance level of 0.05, and a power of 80%. Hence, making a final sample of 90 subjects, 30 orthodontists from Saudi Orthodontics Society, 30 general practitioners from Saudi dental Society and 30 persons without any knowledge about aesthetics (lay persons). All those subjects, who were willing to participate and gave consent of participation, were selected for study.
A postgraduate male dental student (age 29 years) voluntarily agreed to participate in the research. An informed consent form was obtained from the subject. The subject agreed to undergo clinical examination, photography and lateral cephalometric radiography. He was selected as he fulfilled the following criteria: (a) harmonious smile in frontal, oblique and profile views; (b) Class I canine and Class I molar relationship with minimal overjet and overbite; (c) maxillary incisors were well-positioned according to cephalometric standards [Table/Fig-1] and (d) profilometric measurements were within the normal range [Table/Fig-2].
Values of initial maxillary incisor inclination of the subject compared with the values of Bumann A et al., [28].
| Incisor inclination (°) | Norm | Subject |
|---|
| UInc/SN | 102-105 | 108 |
| UInc/FH | 111±5 | 114 |
| UInc/A-Pog | 26 | 24 |
| UInc/NA | 22±4 | 23 |
Values of facial profile of the study subject according to Arnett GW and Bergman RT and Fitzgerald JP et al., [29, 30].
| Measurements | Norm (SD) | Subject |
|---|
| Facial angle (°) | 87.85 (1.71) | 88 |
| Angle of convexity (°) | 0.65 (5.30) | 3.8 |
| ANB (°) | 2.18 (1.97) | 2 |
| SGn/FH (°) | 57.52 (3.32) | 58.6 |
| SGn/Sn (°) | 66.32 (4.14) | 64 |
| FMA (°) | 20.54 (5.59) | 18.2 |
| Nasolabial angle (°) | 114.08 (9.58) | 105.2 |
| Profile angle (G’-Sn-Pog’) (°) | 165-175 | 176 |
| Nasal projection (Sn-NT) (°) | 16-20 | 18 |
| Upper lip/Sn-Pog’ (mm) | +3.5 (1.4) | +2 |
| Lower lip/Sn-Pog’ (mm) | +2.2 (1.6) | +3.2 |
SD:Standard deviation
Image Alteration
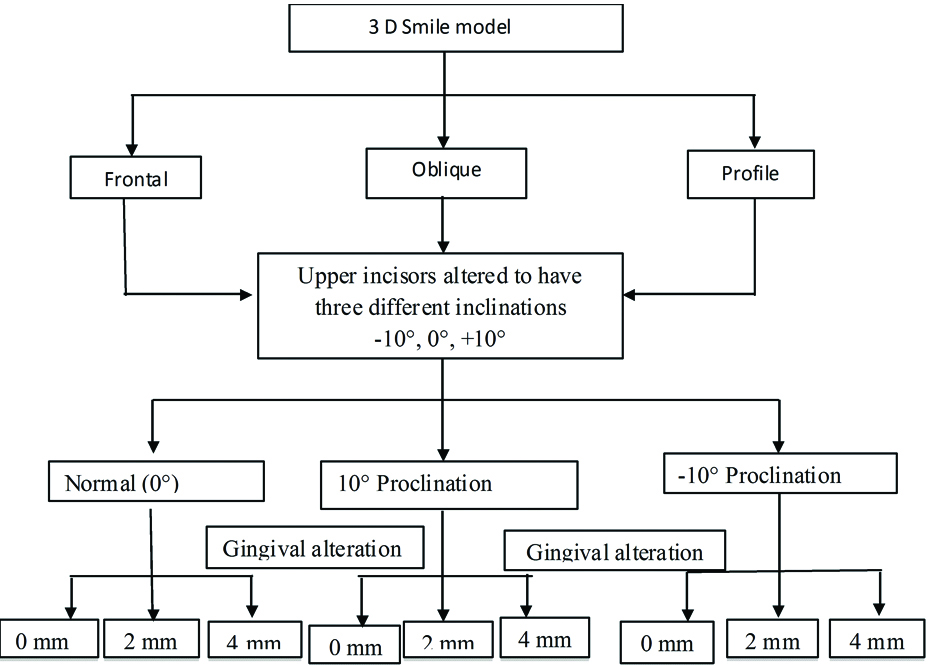
The image was captured using 3D scanner (Sense 3D scanner, 3D systems, South Carolina, USA) which was transferred to Maya 2016 software in order to create a 3D smile model and make changes in the upper incisor inclination and gingival level.
In each view (frontal, oblique and profile), three different groups according to upper incisor inclination (normal, 10° proclination and 10° retroclination) were obtained and under each group, three different gingival levels (0 mm, 2 mm and 4 mm) were used. The total images hence, obtained were 27 (nine in frontal view, nine in oblique view and nine profile view) [Table/Fig-3].
Questionnaire and Observers
A self administered questionnaire [Appendix 1] included the edited photographs with options to choose. The self administered questionnaire was checked for its reliability by test-retest method and using kappa statistics which was found to be satisfactory. Its validity was assessed using Intra Class Corelation (ICC) which was found to be 0.81.
The photographs were coded with serial numbers from 1 to 27. Photographs sharing same view (frontal/oblique/profile) and same inclination (normal/10° proclination/10° retroclination) but with different gingival levels were placed adjacent to each other.
Each group comprised of three pictures with different gingival levels (0 mm, 2 mm and 4 mm) but with same view and inclination. The raters were asked to rank the pictures (sharing same view and same inclination but with different gingival levels) from most to least proclined upper incisor
Four options were available under each picture (no difference, most, moderate and least), in the questionnaire. To eliminate duplicate answers only one option could be selected under each picture. If the rater selected “no difference” as his option then all other options under the pictures would be blocked. After that, the raters were asked to choose a picture that has the highest aesthetics in each view (frontal, oblique and profile) [Appendix 2]. Overall, nine pictures were available under each view. The questionnaires were sent through emails to the study participants.
Statistical Analysis
The data was entered into the statistical software (SPSS version 20.0). Descriptive statistics including number and percentages for categorical variables and mean and Standard Deviations (SD) for continuous variables were calculated. Chi-square test was used to calculate inferential statistics. The level of significance for all tests was set at p≤0.05.
Results
The current study involved a final sample of 90 subjects, 30 orthodontists having average age of 33.07±5.87 years, 30 general dentists aged 29.93±3.05 years; and 30 lay persons of age 27.40±4.38 years.
In the present study, it was found that in frontal view, at normal incisor inclination; 25 (83.3%) orthodontists reported no difference in inclination when compared to 5 (16.7%) dentists and 3 (10%) lay person while 5 (16.7%) orthodontists, 25 (83.3%) dentists and 27 (90%) lay person reported more upper incisors inclination when the gingival level increased [Table/Fig-4]. In frontal view, at 10° incisor proclination in the images; a higher number of 28 (93.3%) lay persons, followed by 25 (83.3%) dentists reported high upper incisor inclination when the gingival level increased. On the other hand, 26 (86.7%) orthodontists reported no difference in perceived inclination. In oblique view, at 10° retroclination; 27 (90%) lay person, followed by 26 (86.7%) dentists reported high upper incisor inclination when the gingival level increased; while 28 (93.3%) orthodontists reported no difference in perceived inclination.
Frequency distribution of the subjects as per their ratings in frontal view with normal incisor inclination and with 10° incisor retroclination, in oblique view with normal incisor inclination and with 10° incisor proclination, in profile view with normal incisor inclination and with 10° incisor proclination.
| Participants (n) | Frontal normal, n (%) | Frontal 10° retroclined, n (%) | Oblique normal inclination | Oblique 10° proclined | Normal profile | Profile 10°proclined |
|---|
| No difference(0 mm, 2 mm, 4 mm) | Difference(0 mm, 2 mm, 4 mm) | No difference(0 mm, 2 mm, 4 mm) | Difference(0 mm, 2 mm, 4 mm) | No difference(0 mm, 2 mm, 4 mm) | Difference(0 mm, 2 mm, 4 mm) | No difference(0 mm, 2 mm, 4 mm) | 0 mm#ModestLeast | 2 mm#LeastModest | 4 mm#MostMost | No difference(0 mm, 2 mm, 4 mm) | Difference(0 mm, 2 mm, 4 mm) | No difference(0 mm, 2 mm, 4 mm) | Difference (0 mm, 2 mm, 4 mm) |
|---|
| Orthodontist (30) | 25 (83.3) | 5 (16.7) | 25 (83.3) | 5 (16.7) | 29 (96.7) | 1 (3.3) | 28 (93.3) | 2 (6.7) {1*, 1#} | 28 (93.3) | 2 (6.7) | 29 (96.7) | 1 (3.3) |
| Dentist(30) | 5 (16.7) | 25 (83.3) | 6 (20.0) | 24 (80.0) | 6 (20.0) | 24 (80.0) | 6 (20.0) | 24 (80.0) | 4 (13.3) | 26 (86.7) | 4 (13.3) | 26 (86.7) |
| Lay person(30) | 3 (10.0) | 27 (90.0) | 5 (16.7) | 25 (83.3) | 4 (13.3) | 26 (86.7) | 2 (6.7) | 28 (93.3) | 4 (13.3) | 26 (86.7) | 4 (13.3) | 26 (86.7) |
| chi-square=42.4888, p-value<0.001** | chi-square=35.278, p-value<0.001** | chi-square=52.398, p-value<0.001** | chi-square= 52.138, p-value<0.001** | chi-square=53.333, p-value<0.001** | chi-square=57.369, p-value<0.001** |
* indicates the sequence (from modest to least to most) of perception by orthodontists in case of oblique 10° proclined view.
# indicates the sequence (from least to modest to most) of perception by orthodontists in cases of oblique 10° proclined view.
** indicates highly significant
In oblique view, at 10° proclination; 24 (80%) dentists and 28 (93.3%) lay person reported high upper incisor inclination when the gingival level increased. Only 2 (6.7%) orthodontists reported different perception for upper incisor inclination with different gingival level; 1 (3.3%) ranked upper incisor inclination as follows (0 mm= modest proclined, 2 mm=least proclined and 4 mm=most proclined) the other one rated upper incisors inclination from least to most as gingival level increased (0 mm=least proclined, 2 mm=modest proclined and 4 mm=most proclined).
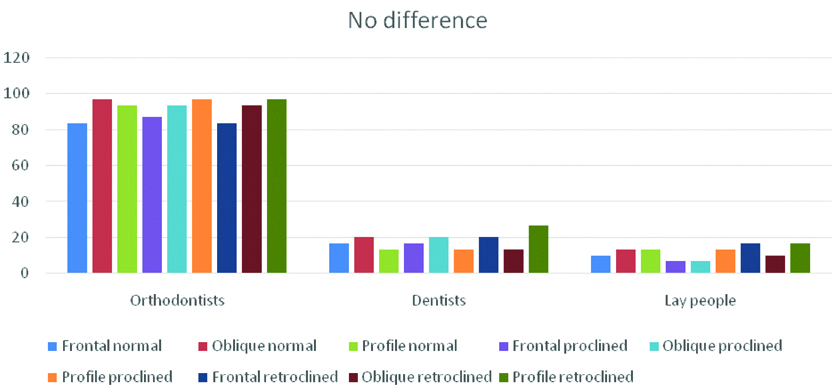
Frequency distribution of the subjects as per their ratings in frontal view with 10° incisor retroclination, oblique view with normal incisor inclination, oblique view with 10° incisor proclination, profile view with normal incisor inclination and profile view with 10° incisor proclination; is given in [Table/Fig-4] respectively. [Table/Fig-5] shows the ratings by the participants for the images showing no difference.
Percentage graph indicating ratings by the participants for the images showing no difference.
Two-way cross-tabulation showed regardless of actual upper incisor inclination (normal/proclined/retroclined) as the gingival display increased the upper incisor were perceived more proclined by dentists and lay person but not by orthodontists. Pearson chi-square test showed this association to be statistically significant (p<0.05), for the total groups. When the ratings of dentists and lay person were compared for different views of images, a non significant difference was found between them (for frontal normal, p=0.71; oblique normal, p=0.73; profile normal, p=1.00; frontal proclined, p=0.42; oblique proclined p=0.25; profile proclined, p=1.00; frontal retroclined, p=1.00; oblique retroclined, p=1.00 and profile retroclined, p=0.36)
Discussion
It is well known fact that aesthetic perception varies from person to person, due to which the perception of specialists might differ from those of the dentists and general population. The patient’s views about orthodontic treatment outcome may vary from those of the dental specialists; hence, it is quite important for the orthodontists to know and understand the patient’s perception towards beauty and aesthetics in order to achieve a satisfactory as well as efficient treatment outcome. A gummy smile is one of the main problems of facial aesthetics. Several previous researches have studied about the suitable extent of gingival display. Peck S and Peck L, had defined Gingival Smile Line (GSL) as a “continuous band of gingiva superior to the maxillary anterior teeth and often posterior teeth [11]. Van Der Geld P et al., reported that subjects with gingival display of 2 to 4 mm were considered most attractive [12].
It was found that in frontal plane (with normal incisor inclination); majority (90%) of lay person, 83.3 % of dentists and 16.7% of orthodontists, reported more upper incisor inclination when the gingival level increased. Majority of the orthodontists (83.3%) reported no difference in inclination when compared to dentists (16.7%) and lay person (10%). These findings indicate that the perception of incisor proclination increases as the gingival show increases regardless of the actual incisor inclination as perceived by dentists and lay person but not by orthodontists. The lay persons and dentists seem to have similar opinions, this finding was in accordance with the previous study conducted by Kokich VO et al., wherein they compared the perceptions of dental professionals and lay person [5]. Both the groups agreed that 3 mm of gingival display resulted in an unattractive smile. The study hence, concluded that there was no difference between lay person and dentists in their perceptions of gummy smile [5].
In the present study, a higher number of lay person (93.3%), followed by dentists (83.3%) reported high upper incisor inclination in the frontal 10° proclined images when the gingival level increased. On the other hand, majority of the orthodontists (86.7%) reported no difference in perceived inclination; thereby, orthodontists being more critical in evaluation. On the contrary, it has been documented in earlier studies that the perception of lay persons and patients regarding the facial harmony was more critical than that of specialist dentists [13-15].
In the present study, for the frontal (10° proclined view); Only 6.7% of orthodontists reported different perception for upper incisor inclination with different gingival levels, 3.3% ranked upper incisor inclination as follows (at 0 mm gingival level, incisors perceived as modest proclined, at 2 mm as least proclined and at 4 mm as most proclined) other 3.3% rated upper incisors inclination from least to most as gingival level increased (at 0 mm as least proclined, at 2 mm as modest proclined and at 4 mm as most proclined). An 80% of the dentists and 93.3% of lay persons reported high upper incisor inclination with the increase in gingival level. A visual difference between orthodontists and lay persons has been observed in previous study as far as aesthetics and occlusal characteristics are concerned [16]. On the contrary, McNamara L et al., and Krishnan V et al., determined a considerable association between orthodontists and lay persons regarding judgement of smile aesthetics [17,18].
In the present study, in the profile view, the orthodontists perceived normal upper incisor inclination being of high aesthetic value whereas lay person perceived 10° retroclination in the upper incisor as highest aesthetic. This finding is in contrast to the results reported by Ghaleb N et al., wherein the authors evaluated the most aesthetic inclination in the profile view of a smile and correlated it with facial features [19].
In the present study, the highest aesthetic images according to the orthodontists in the frontal view was picture number 2 (normal upper incisor inclination and 0 mm gingival display), in the oblique view it was picture number 14 (10° upper incisor proclination and 0 mm gingival display) and in the profile view it was picture number 20 (normal upper incisor inclination and 0 mm gingival display). For the dentists, the highest aesthetic images were picture number 2 in frontal view, picture number 10 (normal upper incisor inclination and 0 mm gingival display) in oblique view and picture number 20 (profile with normal upper incisor inclination and 0 mm gingival display) in profile view. According to lay persons, the highest aesthetic in the frontal view was similar to the other participants, in the oblique images, picture number 14 similar to orthodontists and in the profile images, picture number 25 (10° upper incisors retroclination and 0 mm gingival display). In general, the difference in maxillary anterior aesthetic perceptions between dental professionals and patients or lay persons has been demonstrated in several previous studies [20-23].
The patients are more familiar to the frontal view of the face than the oblique and profile views. The orthodontic treatment is mostly based on the profile view of the patient’s face, hence there exists differences in their perception while evaluation [24].
In the present study, the lay persons and dentists reported higher incisor proclination as the gingival display increased while the orthodontists were able to recognise actual inclination, suggestive of the fact that the dentists and general public are less critical about the aesthetics of the smile. Peck H and Peck S, reported that the layman’s perception of aesthetics is purely motivated by external opinions, and that the mass media is effective in unifying the general public’s perceptions of beauty while as the perception of smile by an orthodontist is due to his/her professional experience [25]. It is mentioned in a yet another previous study that orthodontists being specially trained are found to analyse the aesthetic parameters more efficiently than public and general dentists [26]. Due to difference in the perceptions; the outcome of the orthodontic treatment might not be acceptable to the patient aesthetically; hence, there arises a need for systematic discussion with the patient to identify his/her aesthetic preference regarding the face, smile, and dental arrangement before determining a suitable treatment plan. It is documented in past study that the clinical decision making is mostly dependent on the analysis of the role played by gingiva and incisors with respect to overall perception of aesthetics [27].
Conclusion
Within the limitations of present study, the following conclusions were drawn: gingiva plays an important role in the aesthetics of the smile, and its increased exposure yielded more incisor proclination perception regardless of their actual inclination. Orthodontists significantly identified the actual incisor inclination at different gingival levels better than dentists and lay persons. There was a general concordance between the dentists and the lay person in their perception of upper incisor inclination at different gingival levels. Frontal, oblique and profile views of the same smiles did not necessarily receive similar aesthetic ratings indicating that perception of aesthetic smile depends on the view in which it is observed.
Areas of Future Research
Future studies should consider taking into account all the factors that may cause differences in perceptions and include various other aesthetic parameters for evaluation. Present study may be extended to include the Visual Analog Scale (VAS) to measure the extent of the relation between gingival level and upper incisors inclination in term of perception. Future research may include the effect of other aetiological factors of gummy smile such as vertical maxillary excess and altered passive eruption in perceiving upper incisor inclination. Different malocclusions (class II and class III) and different facial type (delicofacial and brachyfacial) need to be considered during conducting a new study in this field.
SD:Standard deviation
* indicates the sequence (from modest to least to most) of perception by orthodontists in case of oblique 10° proclined view.
# indicates the sequence (from least to modest to most) of perception by orthodontists in cases of oblique 10° proclined view.
** indicates highly significant