Permanent Maxillary First Molar with Two Rooted Anatomy: A Rare Occurrence
Renita Soares1, Ida De Noronha De Ataide2, Karla Maria Carvalho3, Neil De Souza4, Sergio Martires5
1 Senior Resident, Department of Conservative Dentistry and Endodontics, Goa Dental College and Hospital, Bambolim, Goa, India.
2 Professor and Head of Department, Department of Conservative Dentistry and Endodontics, Goa Dental College and Hospital, Bambolim, Goa, India.
3 Lecturer, Department of Oral and Maxillofacial Pathology, Goa Dental College and Hospital, Bambolim, Goa, India.
4 Lecturer, Department of Pedodontics and Preventive Dentistry, Goa Dental College and Hospital, Bambolim, Goa, India.
5 Senior Resident, Department of Orthodontics and Dentofacial Orthopedics, Goa Dental College and Hospital, Bambolim, Goa, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Renita Soares, Senior Resident, Department of Conservative Dentistry and Endodontics, Goa Dental College and Hospital, Bambolim, Goa-403202, India.
E-mail: renita.soares2289@gmail.com
The basis of successful endodontic therapy resides on sound and thorough knowledge of the root canal anatomy and its variations and the clinician’s skills. The importance of the knowledge of the anatomy of root canals cannot be overemphasized. Unusual root and root canal morphologies associated with maxillary molars have been reported in several studies in the literature. The morphology of the maxillary first molar has been studied and reviewed extensively. However the presence of two roots in a maxillary first molar is a rare occurrence and such cases have seldom been reported in literature. This clinical report presents a permanent maxillary first molar with an unusual morphology of two roots with two canals.
Aberration, Incidence, Root canal systems, Two canals
Case Report
A 42-year-old female patient with a non contributory medical history presented to the department of conservative dentistry and endodontics with a chief complaint of pain in the region of the maxillary right first molar. She gave a history of intermittent pain for the last 2 months which had increased in intensity since 3 days.
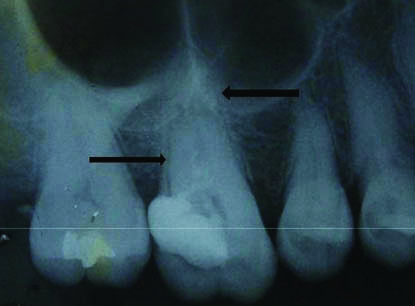
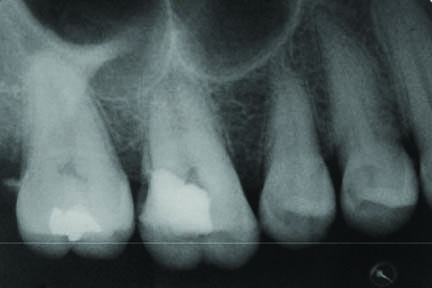
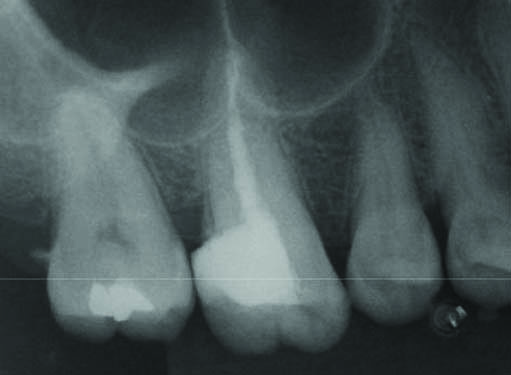
Clinical examination revealed a large interim restoration with the maxillary right first molar. The tooth was tender on percussion. Tooth sensibility testing with electric pulp tester (Gentle-Pulse, Parkell Electronics Division) elicited an early response while thermal testing with heated gutta percha produced an intense lingering response in right maxillary first molar while the other posterior teeth in the quadrant were normal. Widenened periodontal ligament space was noted on the preoperative periapical radiograph with the right maxillary first molar. The radiograph also revealed an unusual anatomy of presence of two roots in the involved tooth [Table/Fig-1]. In order to confirm the atypical anatomy as seen on the preoperative radiograph, supplemental radiographs were taken at different horizontal angulations [Table/Fig-2]. Based on the clinical and radiographic findings, diagnosis of symptomatic irreversible pulpitis in right maxillary first molar with acute periapical periodontitis was made and endodontic treatment was planned.
Preoperative periapical radiograph showing two roots i.e., buccal and palatal.
Periapical radiograph with mesial angulation.
A 2% lignocaine containing 1:80000 epinephrine was administered to obtain local anaesthesia and the tooth was isolated with a rubber dam. Following removal of interim restoration and caries excavation, access cavity was prepared using access cavity burs (Endo Z Access Kit, Dentsply Tulsa, Oklahoma, USA).
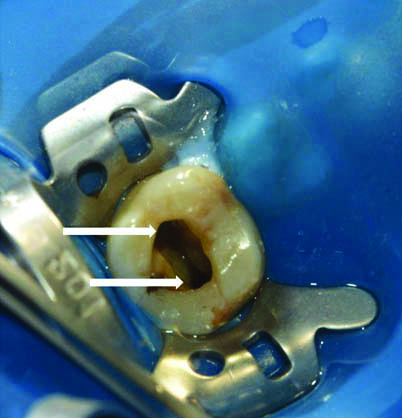
Clinical examination of the pulp chamber floor revealed the presence of only two canal orifices which was further assessed and confirmed with the aid of 3.2x magnification using dental loupes (Admetec Solutions Ltd., Haifa, Israel) with fibreoptic light source that permitted magnification. One orifice was located toward the buccal aspect and was larger in diameter when compared to the typically found buccal orifice in a maxillary first molar. The second orifice was located towards the palatal aspect [Table/Fig-3]. Further close inspection and exploration of the pulpal floor was done for search of additional orifices with the aid of DG-16 explorer under magnification. Additionally, the dentinal map pattern also suggested the presence of two canals.
Pulp chamber floor revealing two large orifices, buccal and palatal.
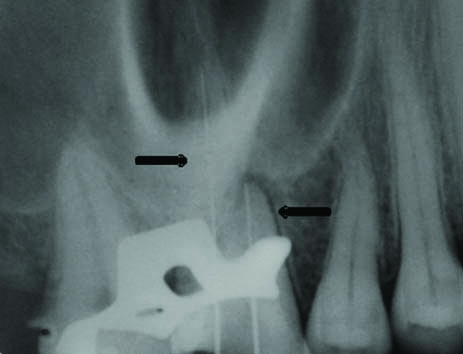
Working length was calculated using an electronic apex locator (Propex Pixi Apex locator, Dentsply Maillefer, Switzerland) as well as the radiographic method. Angulated working length radiograph also suggested positioning of endodontic files in separate buccal and palatal canal [Table/Fig-4]. The canals were cleaned and shaped using rotary ProTaper nickel-titanium instruments (Dentsply Maillefer, Switzerland) using crown down technique under copious irrigation with 2.5% NaOCl and 17% EDTA. After the canals were properly dried using paper points, calcium hydroxide (Avue Cal, Dental Avenue, Param Enterprises, Pune, India) intracanal dressing was placed and access cavity was provisionally sealed with an interim restoration (MD Temp, Meta Biomed, Korea). At the recall appointment 2 weeks later, the patient was completely asymptomatic. The obturation was completed with cold lateral condensation and resin-based sealer (AH Plus, Dentsply DeTrey, Konstanz, Germany) [Table/Fig-5]. The tooth was then restored with nanofiller composite (CeramX, Dentsply DeTrey).
Angulated working length radiograph showing separate buccal and palatal root.
Post obturation radiograph.
Discussion
The basis for success in any endodontic procedure depends on a clinician’s sound scientific knowledge, accurate diagnosis and precise clinical skills. The suitable utilisation of diagnostic aids, including high resolution imaging modalities and magnification equipments that further augment our understanding of the intricacies of the root canal anatomy, can assist in achieving predictable, long term success in our endodontic procedures.
As described by Burns RC the maxillary first molar is possibly the most treated and least understood posterior tooth. Therefore a thorough understanding of the variations occurring in the root canal system is an absolute necessity in achieving endodontic success [1]. The classical presentation of the root canal anatomy of the maxillary first molar is that of three roots with three canals with an incidence as high as 97.6% to 100% [2].
The commonest variation is the presence of a second mesiobuccal canal with an incidence ranging between 18% to 96.1% [3,4]. Other variations include one [5], two [2], four [6] and five [7] roots and unusual morphology of root canal systems within individual roots [8].
The presence of two roots in a maxillary first molar is a rare occurrence with limited cases being reported in literature. Such a variation is more likely to be seen in maxillary second molars.
We conducted an extensive literature search using PubMed to identify cases reporting the unusual anatomy of two roots in a maxillary first molar. The case reports with their respective morphology are summarized in [Table/Fig-6] [2,9-15].
Detailed tabulation of cases reporting the unusual anatomy of two roots: one buccal and one palatal, in a maxillary first molar.
| Authors | No. of canals | Canal Configuration |
|---|
| Buccal | Palatal |
|---|
| Malagnino V et al., [9] | 02 in buccal root01in root | Type II | Type I |
| Fava LR [10] | 02 in buccal root01 root | Type IV | Type I |
| Yilmaz Z et al., [11] | 03 in buccal root01 root | C shaped canal | Type I |
| Ma L et al., [12] | 01 in buccal root01 in palatal root | Type I | Type I |
| Rahimi S and Ghasemei N [13] | 01 in buccal root01 in palatal root | Type I | Type I |
| Shoukie S et al., [14] | 01 in buccal root01 in palatal root | Type I | Type I |
| Pakseat S et al., [15] | 02 in buccal root01 in palatal root | Fusion of MB and DB roots forming a C shaped canal Type I MB2 canal | Type I |
| Sharma S et al., [2] | 01 in buccal splitting at the apical third01 in palatal root | Type V canal configuration in the fused buccal root | Type I |
It is quite uncharacteristic for a maxillary first molar to exhibit two roots, while such a finding may seem to occur more frequently in the case of the maxillary second molar. Cleghorn BM et al., published an exhaustive review on the root and canal systems in the maxillary first molar [16]. The incidence of occurrence of two rooted teeth was reported at 3.8%. In the present case the canal pattern evident in each of the two roots was Vertucci’s Type 1 canal configuration.
Neelakantan P et al., published a detailed report on the root canal morphology of molars in an Indian population by using CBCT [17]. The authors observed that the most common morphology was that of 3 separate roots in the first molars (96.8%). Single-rooted first molars were identified in 0.9% of the teeth studied. Two rooted first molars without fusion were detected in 1.3%, whereas four separate roots were found in 0.9% of the first molars studied. The authors further added that two-rooted first molars showed 2 canal systems, type I (1%) and type IV (0.5%).
Prior to start any endodontic procedure the morphology of the root canals should be examined and carefully evaluated with the help of radiographs projected from different horizontal angulations. A good technique to detect any abberations in the root canal morphology and anatomy is to take a preoperative radiograph and additional radiographic views from a 20° mesial or distal angle. Recent imaging techniques such as Cone Beam Computed Tomography (CBCT) greatly enhance our understanding of the canal morphology. However, CBCT image could not be obtained for this case, due to the patient’s financial constraints. Hence, we took IOPA radiographs and ascertained the morphology with the aid of 3.2x magnification loupes.
Patient consent for this case report was obtained.
Conclusion
The present case report highlights the need to recognise variations in root canal anatomy as a prerequisite for successful endodontic diagnosis and treatment. As clinicians we need to develop our observational and clinical skills as well as amend our understanding of the intricacies of the canal anatomy.
[1]. Burns RC, Access openings and tooth morphology. In: Cohen S, Burns RC, editorsPathways of the pulp 1987 4th edLouisThe CV Mosby Co:120-01. [Google Scholar]
[2]. Sharma S, Mittal M, Passi D, Grover S, Management of a maxillary first molar having atypical anatomy of two roots diagnosed using cone beam computed tomographyJ Conserv Dent 2015 18:342-45.10.4103/0972-0707.15975626180423 [Google Scholar] [CrossRef] [PubMed]
[3]. Kulild JC, Peters DD, Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molarsJ Endod 1990 16:311-17.10.1016/S0099-2399(06)81940-0 [Google Scholar] [CrossRef]
[4]. Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS, Effect of magnification on locating the MB2 canal in maxillary molarsJ Endod 2002 28:324-27.10.1097/00004770-200204000-0001612043874 [Google Scholar] [CrossRef] [PubMed]
[5]. De Souza N, Shetty K, Kolipaka R, Chalakkal P, The use of spiral CT in the detection and management of a permanent maxillary first molar with single root and single canal: A rare occurrenceJ Clin Exp Dent 2017 9:e1172-75.10.4317/jced.5407429075424 [Google Scholar] [CrossRef] [PubMed]
[6]. Christie WH, Peikoff MD, Fogel HM, Maxillary molars with two palatal roots: a retrospective clinical studyJ Endod 1991 17:80-84.10.1016/S0099-2399(06)81613-4 [Google Scholar] [CrossRef]
[7]. Barbizam JV, Ribeiro RG, Tanomaru Filho M, Unusual anatomy of permanent maxillary molarsJ Endod 2004 30:668-71.10.1097/01.DON.0000121618.45515.5A15329575 [Google Scholar] [CrossRef] [PubMed]
[8]. Kottoor J, Velmurugan N, Sudha R, Hemamalathi S, Maxillary first molar with seven root canals diagnosed with cone-beam computed tomography scanning: A case reportJ Endod 2010 36:915-21.10.1016/j.joen.2009.12.01520416446 [Google Scholar] [CrossRef] [PubMed]
[9]. Malagnino V, Gallottini L, Passariello P, Some unusual clinical cases on root anatomy of permanent maxillary molarsJ Endod 1997 23:127-28.10.1016/S0099-2399(97)80260-9 [Google Scholar] [CrossRef]
[10]. Fava LR, Root canal treatment in an unusual maxillary first molar: A case reportInt Endod J 2001 34:649-53.10.1046/j.1365-2591.2001.00445.x11762503 [Google Scholar] [CrossRef] [PubMed]
[11]. Yilmaz Z, Tuncel B, Serper A, Calt S, C-shaped root canal in a maxillary first molar: A case reportInt Endod J 2006 39:162-66.10.1111/j.1365-2591.2006.01069.x16454798 [Google Scholar] [CrossRef] [PubMed]
[12]. Ma L, Chen J, Wang H, Root canal treatment in an unusual maxillary first molar diagnosed with the aid of spiral computerized tomography and in vitro sectioning: A case reportOral Surg Oral Med Oral Pathol Oral Radiol Endod 2009 107:e68-73.10.1016/j.tripleo.2009.01.05119464648 [Google Scholar] [CrossRef] [PubMed]
[13]. Rahimi S, Ghasemi N, Maxillary first molar with two root canalsSultan Qaboos Univ Med J 2013 13:E346-49.10.12816/000325123862051 [Google Scholar] [CrossRef] [PubMed]
[14]. Shakouie S, Mokhtari H, Ghasemi N, Gholizadeh S, Two-rooted maxillary first molars with two canals: A case seriesIran Endod J 2013 8:29-32. [Google Scholar]
[15]. Pakseat S, Rahimi S, Root canal treatment of a two-rooted C-shaped maxillary first molar: a case reportIran Endod J 2014 9(4):301-03. [Google Scholar]
[16]. Cleghorn BM, Christie WH, Dong CC, Root and root canal morphology of the human permanent maxillary first molar: A literature reviewJ Endod 2006 32:813-21.10.1016/j.joen.2006.04.01416934622 [Google Scholar] [CrossRef] [PubMed]
[17]. Neelakantan P, Subbarao C, Ahuja R, Subbarao CV, Gutmann JL, Cone-beam computed tomography study of root and canal morphology of maxillary first and second molars in an Indian populationJ Endod 2010 36:1622-27.10.1016/j.joen.2010.07.00620850665 [Google Scholar] [CrossRef] [PubMed]