Isolated Traumatic Chronic Anterior Dislocation of Radial Head
Akshay Rakeshmohan Bhardwaj1, Gaurav Mahesh Sharma2
1 Senior Resident, Department of Orthopaedics, DDU Hospital, New Delhi, India.
2 Assistant Professor, Department of Orthopaedics, Prakash Institute of Medical Sciences, Islampur, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Gaurav Mahesh Sharma, F-5, New Mahavirjyot Appartment, Govardhan Nagar, LBS Marg Mulund, West Mumbai, Mumbai, Maharashtra, India.
E-mail: sharmagaurav@live.com
Isolated traumatic anterior radial head dislocation is extremely rare and very commonly missed injury. A 12-year-old male had a fall on outstretched hand with pronated forearm. He presented after 6 weeks with complaints of swelling around the antero-lateral aspect of right elbow joint with restriction of movements. The dislocation was treated with open reduction and trans-capitellar K wire fixation. There were no signs of recurrence at one year follow-up. Probability of radial head dislocations should always be kept in mind while dealing with such injuries. Early detection can alleviate the need for open reduction at a later stage.
Elbow joint, Forearm, Radial head dislocation
Case Report
A 12-year-old male child presented to the orthopaedic outpatient department with complaint of difficulty in movement of the forearm and minimal tenderness at right elbow joint since past 6 weeks. The child had a history of fall on an outstretched hand with the forearm in pronation following which he developed pain and swelling around the elbow joint. He was initially treated by a quack in the form of massage and plaster cast application. After six weeks, the plaster cast was removed and the child was then referred to our institute to manage the disability.
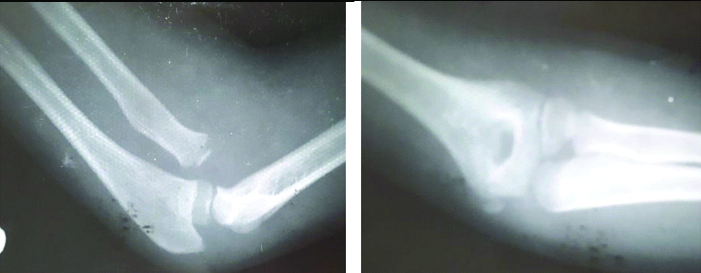
There was fullness at the anterolateral aspect of the right elbow with tenderness. The skin condition over the swelling was normal. There was an extension of -100, flexion was restricted till 1300 and the supination and pronation at forearm were 600 and 700 respectively. Antero-posterior and lateral radiographs of the right elbow joint revealed an anterior dislocation of the radial head with no evidence of fracture either at the radius or the ulna [Table/Fig-1].
Antero-posterior and lateral radiographs of the right elbow joint showing radial head dislocation.
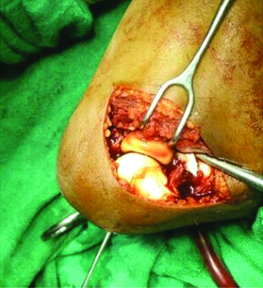
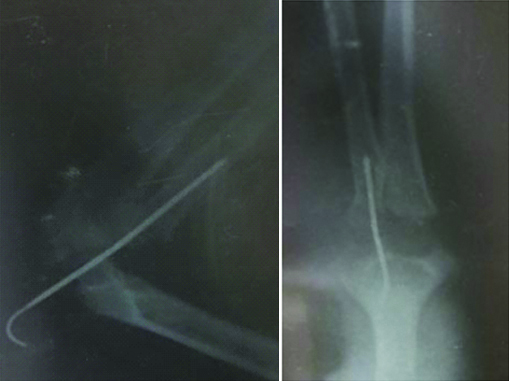
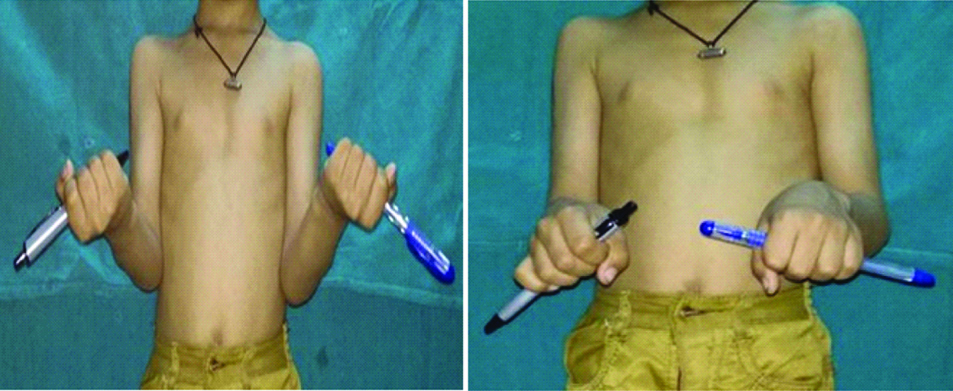
The patient was planned for a closed reduction of the radial head. Under general anaesthesia, an attempt for closed reduction was made which failed and thus, a decision for open reduction was made. Under pneumatic tourniquet coverage, a postero-lateral incision starting from lateral epicondyle distally 5 cm was made. Boyd approach was used and the plane between anconeus and extensor carpi ulnaris was used. The radial head was identified and the proximal radio-ulnar joint was exposed. The radial head was visible through the vent in the annular ligament which prevented its reduction. The annular ligament was fibrosed completely and thus, the remnants were removed. Once the fibrosis was cleared, the radial head could be relocated well. The congruity of the radial head was checked after the tissues were excised and was found to be good. A 2 mm Kirshner wire was then introduced posteriorly through the capitellum and the radiocapitellar joint, and finally passed in the intramedullary canal of the radius to stabilise the radial head [Table/Fig-2]. A stable reduction was achieved with this technique [Table/Fig-3]. Post-operatively, an above elbow plaster cast with the elbow in 90 degree flexion and forearm in supination was applied for 6 weeks. The K wire was removed at the time of plaster cast removal. Gradual passive followed by active assisted range of movements were started following cast removal. The patient was regularly followed-up at 1,3,6 and 12 months respectively. There was an extension of 0o, flexion of 140o and supination of 90o at the end of one year. There was a lag of terminal 50 pronation. Inspite of this lag, the patient was able to do his activities of daily living with ease [Table/Fig-4].
Post-operative radiograph showing K wire in place.
Range of movements at one year follow-up.
Discussion
Isolated dislocation of the radial head is an uncommon injury without association of ulna fracture and can be easily missed [1]. Radial head dislocation can be either traumatic, which is more common in adults or can be congenital, secondary to abnormalities such as diaphyseal aclasis, Ehler-Danlos syndrome, achondroplasia or nail patella syndrome [2,3].
The diagnosis of isolated radial head dislocation especially in children is rare and easily missed due to paucity of knowledge for this condition. In children, presence of ossification centre further adds to the dilemma in such cases. The present case was initially missed and was treated by a quack which later resulted in swelling and restriction of movements. Majority of the times, this condition has a co-relation with ulna fracture or ulna bowing [1,4].
Lincoln TL et al., in their retrospective study over a period of 8 years concluded that the traumatic radial head dislocation is almost always associated with some form of ulnar bowing [5]. They described the ulnar bow sign which states that the radial head subluxation or dislocation should be suspected if there is a deviation of >0.01 mm of lateral ulnar border in a true lateral radiograph. There was no evidence of ulnar bowing in the present case report.
Fall on an outstretched hand with forearm in pronation is the most common mechanism of injury which can further help in determining the manipulation technique for reduction of these dislocations. Our patient had the similar form of injury and thus, supinated position of the elbow helped in maintaining the reduction after removal of the fibrosed annular ligament.
Annular ligament is one of the primary and major stabilizers of the proximal radio-ulnar joint which encircles the radial head and gets inserted at the anterior and posterior margins of the sigmoid notch at the ulna [6]. It prevents the forward, backward and lateral displacement of the radial head [4]. Due to its dynamic nature, many authors strongly advocate the reconstruction of this ligament [1,7]. Various reconstruction techniques have been described in the past namely, Fascia lata graft [7], Palmaris longus tendon [8] or Triceps tendon [2,8]. Bell-Tause procedure and its modification by Lloyd-Roberts and Bucknill has been popular but can be associated with complications such as excessive tension of the ligament, notching of the radial neck, growth disturbances and even elbow [2,5]. The current consensus states that annular ligament reconstruction is not required in all the cases of chronic radial head dislocation [1,2,5,8]. The reconstruction of annular ligament or additional procedure like ulnar osteotomy was not required in the present case because of the stable fixation with K wire and thus not contemplated. No pin tract infection or growth disturbances were seen in the present case.
Clinical dilemma always exists in cases with isolated radial head dislocation without ulnar bowing or ulna fracture and thus, majority of these injuries are missed initially. A true lateral radiograph can usually help in determining the relation of radio-capitellar ratio with the deviation of as much as 20 degrees and thus, detects even small subluxations [9]. A timely diagnosis can avoid the need for open reduction at a later stage and can give optimal results at any age group.
Conclusion
Isolated radial head dislocation is an uncommon injury which requires open reduction majority of the times. We believe that the decision for annular ligament reconstruction should be made intra-operatively after assessing the stability of the reduction.
[1]. Hayami N, Omokawa S, Lida A, Krasarin J, Moritomo H, Mahakkanukrauh P, Biomechanical study of isolated radial head dislocationBMC Musculoskelet Disord 2017 18:47010.1186/s12891-017-1829-129157249 [Google Scholar] [CrossRef] [PubMed]
[2]. De Boeck H, Treatment of chronic isolated radial head dislocation in childrenClin Orthop Relat Res 2000 (380):215-19.10.1097/00003086-200011000-0002911064994 [Google Scholar] [CrossRef] [PubMed]
[3]. Gupta V, Kundu ZS, Sangwan SS, Lamba D, Isolated post-traumatic radial head dislocation, a rare and easily missed inury- a case reportMalaysian Orthopaedic Journal 2013 7(1):74-78.10.5704/MOJ.1303.00325722812 [Google Scholar] [CrossRef] [PubMed]
[4]. Pike JM, Athwal GS, Faber KJ, King GJ, Radial head fractures-an updateJ Hand Surg Am 2009 43(3):557-65.10.1016/j.jhsa.2008.12.02419258159 [Google Scholar] [CrossRef] [PubMed]
[5]. Lincoln TL, Mubarak SJ, "Isolated" traumatic radial-head dislocationJ Pediatr Orthop 1994 14(4):454-57.10.1097/01241398-199407000-000068077426 [Google Scholar] [CrossRef] [PubMed]
[6]. Manasseh N, Madhuri V, Jepegnanam TS, Kayalakagathu VT, Isolated, traumatic anterior dislocation of the radial head in an adultEuropean Journal of Trauma 2005 31(2):170-73.10.1007/s00068-005-1409-1 [Google Scholar] [CrossRef]
[7]. Tan L, Li YH, Sun DH, Zhu D, Ning SY, Modified technique for correction of isolated radial head dislocation without apparent ulnar bowing: a retrospective casestudyInt J Clin Exp Med 2015 8(10):18197-202. [Google Scholar]
[8]. Marinello PG, Wagner T, Styron J, Maschke S, Evans PJ, Annular ligament reconstruction with triceps autograft for chronic radial head instabilityTech Hand Up Extrem Surg 2016 20(1):21-25.10.1097/BTH.000000000000010926709571 [Google Scholar] [CrossRef] [PubMed]
[9]. McCann F, Canet F, Sandman E, Petit Y, Rouleau DM, Does radiographic beam angle affect the radiocapitellar ratio measurement of subluxation in the elbow?Clinical Orthopaedics and Related Research 2013 471(8):2556-62.10.1007/s11999-013-3027-223653100 [Google Scholar] [CrossRef] [PubMed]