Coronary Artery Disease (CAD) is a leading cause of morbidity and mortality across the globe. Various risk assessment scores are used for identifying presence and severity of CAD. Risk assessment score systems like Gensini score, clinical Syntax score, Mayo clinic score, and Euroheart scores have been proposed and evaluated for predicting the severity of CAD and for assisting the attending physician to make treatment decisions. The scoring systems consider severity of stenosis, overall coronary anatomy and morphology of arteries for prediction. While these scoring systems are effective in predicting long and short term CAD risk, the main pitfall is that they require results of coronary angiography or coronary computed tomography angiography [1-4]. Furthermore, it is not always feasible to advise coronary angiography for asymptomatic patients (who might be at a risk of developing CAD due to strong family history and lifestyle factors) as well as patients with atypical chest pains [5].
The CHADS2 score was first proposed in the year 2004 as a prediction approach for estimating the risk of stroke in the patients with non valvular Atrial Fibrillation (AF). AF hampers blood flow to the upper heart chambers and thus leads to the formation of mural thrombus [6]. Such mural thrombus can dislodge from its position and can reach the brain via bloodstream to cut-off the blood supply and precipitate stroke. The CHADS2 scoring system is thus implemented to determine the requirement for anticoagulation or antiplatelet therapy in AF patients in order to reduce the risk of stroke [7]. The CHA2DS2-VASc is a refinement of CHADS2 score which include additional stroke modifying risk factors and has outperformed its predecessor in multiple patient groups including patients with AF who are receiving outpatient elective electrical cardioversion [6].
Since both the CHADS2 and CHA2DS2-VASc scores include risk factors which are also associated with the development of CAD, they have been shown to predict the severity of CAD. In order to improve the risk prediction for CAD, these scores were further reformulated as CHA2DS2-VASc-HS. This scoring system includes hyperlipidemia and smoking as other major risk factors for CAD and considers male gender as a high risk factor. Previous studies have compared the three scoring systems for predicting CAD and have identified CHA2DS2-VASc-HS to be the best scoring system [8].
In this study, we assessed the accuracy of CHA2DS2-VASc-HS scoring system for predicting CAD in tertiary hospital settings. We also compared the CHA2DS2-VASc-HS score with the Gensini score in the CAD risk stratification of patients undergoing angiography.
Materials and Methods
Study Design and Study Settings
The study was a single center, prospective, observational cohort study of the patients requiring diagnostic angiography. The patients admitted were observed for Gensini score and CHA2DS2-VASc-HS scores. Consecutive patients admitted for diagnostic angiography and abiding the eligibility criteria were enrolled. The study was carried out at Amrita institute of medical sciences, Kochi, Kerala, India during the one year study period between November 2014 and October 2015. The study was approved by the local ethics committee. Patient’s anonymity was maintained strictly and informed consents were obtained.
Eligibility Criteria
Patients admitted for an elective diagnostic coronary angiography having symptoms suggestive of CAD and/or abnormal non-invasive stress tests based on positive treadmill testing or myocardial perfusion imaging test were enrolled for the study. Patients with acute ischemic stroke or Transient Ischemic Attack (TIA), history of Coronary Artery Bypass Grafting (CABG) or Percutaneous Transcatheter Coronary Intervention (PTCA), patients with symptoms of cardiac failure, and acute coronary syndrome were excluded from the study. Patients undergoing repeat angiography were also excluded.
Study Method and Definitions
A detailed medical history of all patients was taken which included observations of clinical and physical examination, results of 12 lead electrocardiogram, and outcomes of echocardiography, history of diabetes mellitus, hypertension, and hyperlipidemia, along with history of chronic heart failure, acute ischemic stroke, TIA and peripheral artery disease. National Cholesterol Program-3 recommendations were referred to identify hyperlipidemia [9]. Also, patients taking cholesterol lowering drugs were also identified as hyperlipidemic. Considering the definition used for smoking by previous studies which validated CHA2DS2-VASc-HS score, a person smoking 10 or more cigarettes per day from last one year without any efforts for quitting was considered a smoker [8]. The CHA2DS2-VASc-HS scores were calculated, as shown in [Table/Fig-1] by a cardiologist who was blinded to the angiography results.
Calculation of CHA2DS2-VASc-HS score [8].
| Acronym | Risk factor | Score |
|---|
| C | Congestive heart failure | 1 point |
| H | Hypertension | 1 point |
| A2 | Age more than 75 years | 2 points |
| D | Diabetes mellitus | 1 point |
| S2 | Previous stroke or TIA | 2 points |
| V | Vascular disease | 1 point |
| Sc | Sex category | Male: 1 point; Female: 0 point |
| H | Hyperlipidemia | 1 points |
| S | Smoker | 1 point |
| Maximum score possible= | 11 points |
TIA: Transient ischemic attack
Coronary artery angiography was performed by a trained cardiologist who also evaluated the angiograms as well as calculated Gensini score, as shown in [Table/Fig-2] for each patient. Severe (Obstructive) CAD was diagnosed if there was 50% diameter stenosis in at least one major epicardial coronary artery. Single vessel disease was defined as the presence of 50% luminal diameter stenosis in at least one major coronary artery. Multivessel coronary disease was defined as the presence of 50% luminal diameter stenosis involving at least two major epicardial coronary arteries; left main coronary artery narrowing of ≥50% was considered as two vessel disease [8].
Steps to calculate Gensini score.
| Score according to the severity of coronary artery stenosis |
|---|
| 1 | 1% to 25% narrowing |
| 2 | 26% to 50% narrowing |
| 4 | 51% to 75% narrowing |
| 8 | 76% to 90% narrowing |
| 16 | 91% to 99% narrowing |
| 32 | Completely occluded artery |
| Multiply the score with the multiplication factors according to the affected artery |
| 5 | For a left main coronary artery |
| 2.5 | For proximal LAD artery and proximal circumflex artery |
| 1.5 | For LAD artery |
| 1 | For distal LAD artery, mid or distal circumflex artery, and RCA |
| 0.5 | For any other branch |
LAD: Left anterior descending artery; RCA: Right coronary artery
Once both the CHA2DS2-VASc-HS score and Gensini scores were obtained, the patients were divided in to three groups according to the level of coronary stenosis. The three groups were: 1) Normal coronary arteries; 2) Mild CAD (stenosis <50%); 3) Severe CAD (stenosis ≥50%) [8]. The severe CAD group was further classified as Single Vessel Disease (SVD); Double Vessel Disease (DVD); and Triple Vessel Disease (TVD). The two scores were then compared in the following manner:
CHA2DS2-VASc-HS score and Gensini Score of the three groups were compared with each other and two groups were arbitrarily divided into CHA2DS2-VASc-HS score <3 and ≥3 [8]. Gensini scores of the above mentioned two groups were compared.
Statistical Analysis
Continuous data were presented as mean±SD and/or median (minimum-maximum). One way ANOVA or Kruskal-Wallis test was used to compare the average CHA2DS2-VASc-HS score and Gensini score among number of diseased vessels category. Spearman’s rank correlation was used to find correlation between CHA2DS2-VASc-HS score and Gensini score. Mann-Whitney test was applied to compare the Gensini score among the CHA2DS2-VASc-HS score in the two groups (<3 and ≥3). A p-value <0.05 was considered as statistically significant. Statistical analysis was conducted using SPSS 17.0 for Windows.
Results
A total of 100 patients were studied. Mean age of the study population was 59.4±8.9 years. Around 70% of the study population were males (n=70). Of the 100 patients, 19 patients (19%) had normal angiograms, 22 patients (22%) had mild CAD, and 59 patients had obstructive (severe) CAD. Of the patients having obstructive (severe) CAD, 12 (12%) had SVD, 25 (25%) had DVD and 22 (22%) had TVD. A comparison of the baseline demographics and characteristics of the three groups (normal coronary arteries, mild CAD, and severe CAD) are presented in [Table/Fig-3]. CHA2DS2-VASc-HS and Gensini scores were significantly different among the three groups and between each other. A significant increase in both the scores was observed with increase in severity of CAD (p<0.001). From group one to group three, a significant increase in the mean age, percentage of male patients, and trend of hypertension, diabetes mellitus, hyperlipidemia, and smoking was noted.
Baseline demographics and clinical parameters.
| Number of diseased vessels |
|---|
| Normaln=19 | Mild CADn=22 | Severe (obstructive) CAD, n=59 |
|---|
| SVDn=12 | DVDn=25 | TVDn=22 |
|---|
| Age (Years) | 53.4±4.8 | 55.5±6.7 | 60.9±6.9 | 61.9±10.0 | 65.7±8.0 |
| GenderMaleFemale | 8 (42.1)11 (57.9) | 13 (59.1)9 (40.9) | 10 (83.3)2 (16.7) | 21 (84.0)4 (16.0) | 18 (81.8)4 (18.2) |
| CHA2DS2-VASc-HS score* | 1.4±0.81.0 (0.0-3.0) | 2.1±0.92.0 (1.0-5.0) | 2.6±1.03.0 (1.0-4.0) | 3.9±1.14.0 (2.0-7.0) | 4.7±1.15.0 (3.0-7.0) |
| Gensini Score* | 0.0±0.00.0 (0.0-0.0) | 2.0±1.21.5 (1.0-6.0) | 13.8±7.113.5 (3.0-24.0) | 42.4±26.034.0 (4.0-100.0) | 60.4±34.056.3 (18.0-153.0) |
| C | -- | -- | -- | -- | 1 (4.5) |
| H | 4 (21.1) | 12 (54.5) | 6 (50.0) | 20 (80.0) | 18 (81.8) |
| A2 | -- | -- | 1 (8.3) | 2 (8.0) | 5 (22.7) |
| D | 6 (31.6) | 6 (27.3) | 5 (41.7) | 14 (56.0) | 19 (86.4) |
| S2 | -- | -- | -- | 2 (8.0) | 2 (9.1) |
| V | -- | -- | -- | 1 (4.0) | 3 (13.6) |
| A | -- | 2 (9.1) | 2 (16.7) | 8 (32.0) | 9 (40.9) |
| Sc | 8 (42.1) | 13 (59.1) | 10 (83.3) | 21 (84.0) | 18 (81.8) |
| H’ | 9 (47.4) | 12 (57.1) | 5 (41.7) | 19 (76.0) | 17 (77.3) |
| S | -- | 1 (4.5) | 1 (8.3) | 7 (28.0) | 4 (18.2) |
Data are expressed as mean±SD and/or median (minimum to maximum) or count (percentage) for categorical variables; Mann-Whitney test or unpaired t-test was applied. A p-value <0.05 was considered as statistically significant.
* p-value <0.001
Furthermore, when the study population was divided arbitrarily on the basis of CHA2DS2-VASc-HS score in to two groups (<3 and ≥3), there was significant difference among the two groups in terms of Gensini scores with a significant p-value <0.001. Mean Gensini score in the group with CHA2DS2-VASc-HS score <3 (n=44) was 2.34±4.13 (median-1, range 0-21), while the mean Gensini score in the group with CHA2DS2-VASc-HS score ≥3 (n=56) was 43.66±31.95 (median-33.8, range 0-153).
The CHA2DS2-VASc-HS score also increased as the number of diseased vessels increased, ranging from a mean of 1.4±0.8 (median-1, range 0-3) in patients with normal angiograms, to a mean of 4.7±1.1 (median-5, range 3-7) in patients with TVD. There was a significant p-value for trend (<0.001). Similarly, the Gensini scores also showed an increasing trend as the number of diseased vessels increased, starting from 0 in patients with completely normal angiograms, to a mean of 60.4±34.0 (median-56.3, range 18.0-153.0) in patients with TVD. There was a significant p-value for trend (<0.001).
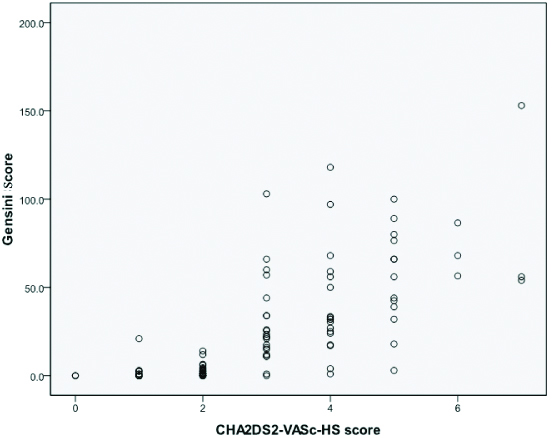
There was a positive correlation between CHA2DS2-VASc-HS score and Gensini score using Spearman’s rank correlation test (correlation coefficient 0.813, p<0.001) [Table/Fig-4].
Correlation between CHA2DS2-VASc-HS score and Gensini score.
Spearman’s correlation has been applied; p<0.05 has been considered statistically significant.
Discussion
The two major findings of the study were: 1) A significant increase in CHA2DS2-VASc-HS score can be observed with increase in severity of CAD; and 2) A significant positive correlation can be found between increase in CHA2DS2-VASc-HS score and Gensini score.
Advancing age, male gender, chronic hypertension, chronic hyperlipidemia, and diabetes mellitus along with continued smoking for more than one year are all well accepted risk factors for the development of CAD [10]. While CAD remains one of the major leading causes of morbidity and mortality around the world, its development is often treacherous. CAD can appear without any warning signs and therefore it is important to have a risk assessment tool which can predict CAD based on the known risk factors which can be modified. Early assessment can improve the provision of medical assistance, improve survival rates, and reduce economic burden [11]. In order to prescribe effective preventive strategies, the cardiologist requires a reliable and quantitative risk stratification tool which works independent of results of invasive diagnostics.
Several scoring systems like Framingham risk score, Reynold’s risk score, PROCAM risk algorithm, and WHO/ISH risk predictions charts, which operate independent of coronary angiography results, have been proposed for CAD risk stratification [12-15]. These scoring systems predict CAD risk by analysing risk factors like age, gender, hypertension and diabetes status, presence of chest pain, hyperlipidemia status, and smoking habits. However, these scoring systems have their own limitations. These scoring systems stratify a high risk patient on the basis of the defined risk factors however, they usually fail to identify low risk patients who have multiple marginal abnormalities. Also, these risk models identify only those patients who are at risk of developing CAD within a defined period (e.g., 10 years for CHD in the Framingham model) [11]. These approaches do not consider lifetime risk which could be significantly higher and rectifiable with aggressive risk factor management [16]. Only the 2013 ACC/AHA guideline for CAD assessment offers lifetime risk estimation, overestimation 10 years risk for CAD is also a major drawback of this approach [17]. CAD risk increases with advanced age, but none of the above mentioned tools include age specific risk factor (age >75 years) for assessment.
The newly designed CHA2DS2-VASc-HS score has not been evaluated extensively for risk stratification of CAD as well as its clinical implementation in treatment decision making process. Only two studies are available which have evaluated CHA2DS2-VASc-HS score for CAD prediction. The studies reported the scoring system as an effective and easy tool for risk stratification. However, both the studies were performed on Turkish people and the outcomes cannot be generalised in Indian origin people due to racial differences [8,18]. The present study evaluated the CHA2DS2-VASc-HS score in Indian population and found similar effectiveness for CAD risk assessment. Similar to the earlier studies, the present study found that risk factors used for CHA2DS2-VASc-HS score calculation like hypertension, male gender, smoking status, diabetes mellitus, and hyperlipidemia are significantly associated with increased risk of CAD in Indian population [18]. The earlier study reported that CHA2DS2-VASc-HS score >2 indicates CAD risk [8]. The present study also shows that an arbitrary CHA2DS2-VASc-HS value more than two can be used to differentiate patients with mild CAD from those with severe CAD.
A significantly high correlation was found between Gensini score and CHA2DS2-VASc-HS score (p<0.001) which suggested that this newly developed scoring system is an effective, convenient as well as rapid screening method. Since, the scoring system does not require complicated computations (like Gensini score) and results of invasive diagnostics, it can be applied in emergency hospital settings to reduce time lapse in treatment decision making process.
Limitation
The only limitation of the study was its single center and small population study design. A large scale study performed at different study sites which include patients with variable demographic characteristics is further needed to validate the repeatability of the new scoring system.
Conclusion
The present study found that CHA2DS2-VASc-HS scoring system is correlated with the severity and complexity of CAD. The positive correlation of this scoring system with well-studied Gensini scoring system proves its accountability. The CHA2DS2-VASc-HS is a convenient and rapid scoring system which does not require any sophisticated diagnostic procedures to predict severity of CAD. The scoring system can be used in emergency setting to prevent crucial time lapse.
Data are expressed as mean±SD and/or median (minimum to maximum) or count (percentage) for categorical variables; Mann-Whitney test or unpaired t-test was applied. A p-value <0.05 was considered as statistically significant.
* p-value <0.001