The proportion of persons aged 60 years and above is growing worldwide, faster than any other age group, due to a decline in fertility and mortality, i.e., low birth rates, combined with long life expectancies. Older people have limitations in their functional and regenerative abilities, and are more prone to diseases and infirmities, when compared to younger adults [1,2].
Normal ageing brings with it a myriad of changes in all systems of the body, including the nervous, sensory, endocrine, immune, cardiovascular, respiratory, excretory, gastrointestinal and musculoskeletal systems. Ageing is seen to decrease physical fitness, which includes the components of endurance, strength, flexibility and agility. This decrease can lead to difficulties in functioning normally and carrying out activities of daily living [3,4].
Exercise training has been seen to have positive effects on fitness levels, cardiorespiratory functions, fall risk and cognitive function in elderly individuals [5,6]. Regular exercise and physical activity can benefit people of all age groups, and in the elderly, it can promote independent living, prevent or decrease disability, and lead to better quality of life. Exercise can promote healthy ageing and thus can help to decrease the burden posed to economies by healthcare of elderly individuals [7].
Functional mobility and functional exercise capacity are components of fitness which have a huge influence on the day- to- day living of elderly subjects. The 8 UG test and 6 MWT are reliable and valid tests used in the elderly to measure functional mobility and functional exercise capacity respectively [8,9].
Quality of life is described as a wellness which comes about from a combination of physical, functional, emotional and social factors. Exercise has been suggested as a means of improving physical functions and independent living, thus improving health related quality of life. The SF-36 (Medical Outcomes Study 36-item Short Form Health Survey) is one of the most widely used instruments to measure Health Related Quality of Living (HRQOL). The SF-36 has been translated and validated in many different languages and cultures and in more than 40 countries [10-14].
Promoting independent living among elders is essential to maintain productivity of the society and reduce healthcare costs. There was a need to study the effect of a multi-component exercise program on the functional mobility, functional exercise capacity and quality of life, which are the most important factors influencing independent living. Hence, the present study aimed at evaluating the effect of a multi-component exercise program, including aerobic, strengthening, and functional and balance training, on functional mobility, exercise capacity and HRQOL in elderly individuals.
Materials and Methods
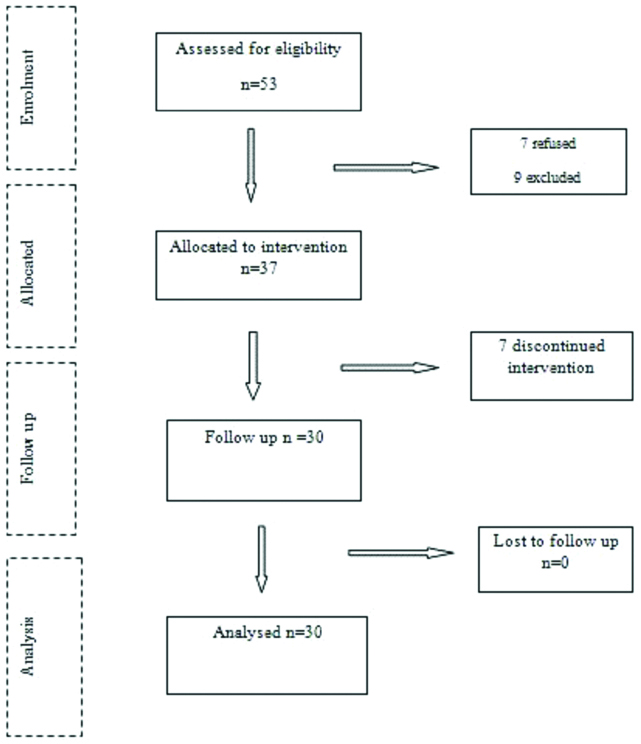
The present quasi-experimental study was conducted on 30 community dwelling older adults aged 65 years and older, which comprised of 15 men and 15 women selected purposively from areas in and around Mangaluru, India. The present study was part of a larger study being conducted with the same objectives. The methodology of the study is depicted in [Table/Fig-1].
Flowchart of progress of participants through the stages of the study.
Ethical clearance was obtained for the study from the Institutional Ethical Committee of NITTE Institute of Higher Education, Mangaluru. Informed consent was obtained from each subject prior to participation. The participants had to be able to ambulate independently and able to understand instructions. Those with acute neurological impairment such as Parkinson’s disease, acute stroke, lower limb weakness, those with severe cardiac or pulmonary disease, and those with severe psychiatric illness were excluded. Also, excluded were those with other severe physical illness such as recent unhealed fracture, vestibular impairment, uncontrolled diabetes mellitus or hypertension, acute myocardial infarction, substance abuse or terminal illness.
The study was carried out in the time period between March 2016 and January 2017. Outcome measures were obtained prior to the intervention, and at 10 weeks, after completion of the intervention. The outcome measures were: 1) 8 UG test to measure functional mobility; 2) 6 MWT to measure exercise capacity; and 3) the SF-36 to measure health related quality of life which were all standard, reliable and valid measures of their respective variables [9-11]. The Kannada and Malayalam versions of the SF-36 were used in those subjects who were unable to comprehend English.
The intervention given to the selected participants was a supervised multi-component exercise protocol consisting of progressive resisted exercises, balance exercises, functional training and aerobic exercise for three days a week for 10 weeks. The exercise program had the following components:
Progressive resisted training: This was given for major muscle groups of upper limb and lower limb at 40-80% of 1 repetition maximum, 1-3 sets of 8 repetitions using free weights. The muscles trained were: pectoralis major and minor, biceps brachii, triceps brachii, the deltoid muscles, iliopsoas, glutei maximus, medius and minimus, quadriceps, hamstrings and calf muscles. Theraband exercises, isometric exercises and functional resisted exercises like wall push-ups, squats, lunges etc., were also included progressively. The Theraband exercises were done progressing from yellow to red to blue, green and black coloured therabands. The progression was done on a weekly basis, based on the improvement observed in the patient. Support was provided as and when necessary, especially during the functional resisted exercises [15].
Balance training: Progressively challenging balance exercises adjusted to individual needs, like standing with feet together, tandem standing, perturbations, obstacle courses etc., [16].
Functional training: Exercises designed to improve functional activities, like walking, stepping, transfers, mat exercises, catching and throwing a ball etc. The intensity of the exercises was increased based on individual needs and abilities [17].
Aerobic training: Approximately 15-60 minutes of continuous or discontinuous aerobic activity, at 55-90% of maximal heart rate (40-80% of VO2 max) progressed in intensity gradually [18].
The subjects were allowed rest periods during the exercise as necessary, and their heart rate and blood pressure were monitored before and after the exercise session, and in between if required. Each exercise session was of approximately 90 minutes duration, including the rest periods.
Statistical Analysis
After completing the exercise program, all the scores were tabulated and subjected to statistical analysis. Analyses were carried out using SPSS software (IBM SPSS Version 20.0). Descriptive statistics were used to describe the baseline statistics of the participants. The paired t-test was used for calculating the pre- to post difference in the outcome measures. A repeated measures ANOVA was used to analyse the changes in the measures taken every two weeks. A probability level of <0.01 was considered to be significant.
Results
A total of 30 subjects were recruited into the study, and data collected from 15 men and 15 women were analysed after discounting dropouts. The participants varied in ages from 63 to 91 years (mean age 72.8±6.408).
The paired t-test results for the three outcome measures namely 8 UG, 6 MWD and SF-36 are shown in [Table/Fig-2]. There was a significant difference in all three measures when post-intervention scores were compared with pre-intervention scores (p<0.01).
Comparison of means of 8 UG, 6 MWD and SF-36 pre- and post-intervention using paired t-test.
| Measure | Paired differences | t | df | Sig. 2-tailed |
|---|
| Mean | Standard deviation | Standard error mean | 95% confidence interval of the difference |
|---|
| Lower | Upper |
|---|
| 8 UG | 1.28000 | 0.67333 | 0.12293 | 1.02857 | 1.53143 | 10.412 | 29 | 0.001 |
| 6 MWD | -1.8433 | 12.15328 | 2.21888 | -22.971 | -13.895 | -8.308 | 29 | 0.001 |
| SF 36 | -5.8666 | 4.04912 | 0.73927 | -7.3786 | -4.3547 | -7.936 | 29 | 0.001 |
8 UG: 8-foot up and go test; 6 MWT: Six minute walk test; SF-36: short form 36 scale
The multivariate analysis to test the significance of the values obtained at intervals of two weeks during the intervention, i.e., pre-intervention, at the second week, fourth week, sixth week, eighth week and 10th week as shown in [Table/Fig-3]. The test showed that all the three outcome measures showed a significant difference between the weeks (p<0.01).
Multivariate analysis of the measures at two- week intervals using repeated measures ANOVA.
| Measure | Wilks Lambda | HoDf | Error Df | F | p-value |
|---|
| 8 UG | 0.181 | 5 | 24 | 21.73 | p<0.01 |
| 6 MWD | 0.136 | 5 | 24 | 30.57 | p<0.01 |
| SF 36 | 0.295 | 5 | 24 | 11.47 | p<0.01 |
8 UG: 8-foot up and go test; 6 MWT: Six minute walk test; SF-36: short form 36 scale
Discussion
The present study was aimed at assessing the effect of a multi-component exercise program on functional mobility, functional exercise capacity and health related quality of life in older adults. Post- exercise testing was completed by 30 of the 37 subjects recruited into the study; seven subjects discontinued exercise citing various reasons, though none of the subjects reported exacerbation of any health problems as a result of participation in the exercise program. The results showed that there was a significant improvement in all the three parameters after a 10 week exercise program and at two week-intervals during the program.
Functional mobility is an essential component for meaningful existence of an older adult, as it contributes to participation in physical, social and cultural activities. Outdoor physical activity, especially walking, is an important component of maintaining physical independence in elderly subjects. Mobility, or walking ability, is a result of the integrated functioning of the cardiorespiratory, musculoskeletal and the sensorineural systems [19].
In the present study, the mean 8 UG and 6 MWT scores of the participants before intervention were 12.13 seconds and 287.3 metres, both of which were in the less than average category for the specified age group, indicating a population which was at risk for becoming functionally dependent [20,21]. The mean of the SF-36 total scores was 63.13, calculated by averaging the physical and mental scores [22]. Post intervention, all the three outcome measures showed significant improvement, and the improvement was consistent throughout the two week intervals at which the measurements were made. These findings have clinical importance in a population of community dwelling elderly such as the one studied by us, since even modest improvements in mobility go a long way in maintaining an elderly individual’s functional independence in the community.
A multicomponent exercise program is one which involves multiple components, which may include exercises targeting strength, power, muscle endurance, cardiovascular endurance, balance and postural control [23]. This kind of exercise program has been recommended by the American College of Sports Medicine (ACSM) for promoting optimal ageing, minimising the adverse effect of ageing, and prevention and treatment of diseases in the elderly [24].
Postural balance and lower extremity strength are two of the most important pre- requisites for walking [19]. An exercise program such as the one carried out in the present study can address these two issues with the components of progressive resistance training and balance training. Functional training, as carried out by us has also been seen to improve walking ability in previous studies [25]. Vincent HK et al., showed in a review that aerobic exercise combined with resistance training is able to improve functional mobility in obese older adults [26]. The Lifestyle Interventions and Independence for Elderly (LIFE) study results published in 2014 showed that a structured moderate intensity physical activity program which included aerobic, resistance and flexibility exercises was more efficient than a health education program in improving mobility in elderly individuals [27].
Exercise has been seen to have more positive effects in those above 65 of years of age when compared to any other age group [28]. Participation in an exercise and physical activity program can improve health related quality of life by improving mobility, functional independence and overall well being. Gill DL et al., found that quality of life was both an outcome and a motivator for exercise and physical activity, and elderly people tend to associate exercise with social and emotional benefits as much as physical benefits [29].
The present findings add to the present body of literature which quote the benefits of multiple components of physical exercise in improving mobility; there are very few studies which have explored this relationship in community dwelling elderly in India. Walia S et al., have shown a specific balance strategy training program to be effective in improving mobility in a sample of elderly Indian adults, and their results were comparable to that of present study [30]. A physical exercise program should be recommended to all elderly adults in order to improve their health and mobility, which in turn will help maintain their productivity and functional independence. This is especially important in a country like India where the elderly population is fast growing, and a majority of elderly people tend to be inactive and even housebound [31].
Limitation
The limitations of the present study were the absence of a control group, a relatively small sample size, the lack of stratification of the samples into different age groups, and the lack of long term follow- up. These issues should be addressed in further studies.
Conclusion
A 10-week multicomponent exercise program comprising of aerobic, resistance, functional and balance exercises significantly improved the mobility, functional exercise capacity and health- related quality of life in elderly individuals. Further studies should focus on the specific effects of different types of exercises in particular age groups of elderly people.
8 UG: 8-foot up and go test; 6 MWT: Six minute walk test; SF-36: short form 36 scale
8 UG: 8-foot up and go test; 6 MWT: Six minute walk test; SF-36: short form 36 scale