Thyroid USG has been used in differentiating benign from malignant nodules and for guiding Fine Needle Aspiration Cytology (FNAC) for nodules suspected of being malignant [1-3]. However, fewer than 5.0%-6.5% of incidentally discovered thyroid nodules are malignant. Therefore, it is necessary according to malignancy risk, that a criteria is established for selecting thyroid nodules for FNAC [4].
There is increasing complexity of terminology used in ultrasound reporting and treating physician and surgeons face a lot of difficulty in understanding the actual meaning of those terms. So, there was a need to introduce a system through which radiologists could communicate better with the clinicians. TIRADS classification system was developed with the main goal to standardise the reporting of results of thyroid ultrasound that can be understood by clinicians and also stratify the risk of malignancy of a lesion based on the USG features of the lesion. The terminology TIRADS was first used by Horvath E et al., drawing inspiration from the “Breast Imaging and Reporting Data System” (BIRADS) of the American College of Radiology [5]. Russ G et al., proposed a TIRADS classification that was further modified and they proposed that TIRADS will be more helpful in the settings where Fine Needle Aspiration Biopsy (FNAB) is not readily available and so decisions will therefore be based to a great extent on the US features of the lesions and TIRADS classification as this implies the potential risk for malignancy [6].
This study was conducted with an aim to assess the USG characteristics which are highly suggestive of malignancy and to assess the reliability of TIRADS in the differentiation of malignant from benign thyroid nodules.
Materials and Methods
The present study was an observational study conducted on 200 consecutive patients from December 2014 to December 2016 in the Department of Radiodiagnosis in collaboration with the Department of Pathology and Surgery in Jawaharlal Nehru Medical College and Hospital, Faculty of Medicine, AMU, Aligarh, India. The patients presenting to the surgery outpatient department for neck swelling were initially clinically evaluated for thyroid swelling. They were referred to the radiology department and underwent ultrasound of the thyroid. Colour and power Doppler were used as and when necessary. This study was approved by Institutional Ethics and Research Advisory Committee. Written informed consent was obtained from all the patients who participated in the study. The patients of any age or sex were included in the study who presented with clinically suspected thyroid nodules were included in study. Patients with diffuse thyroid disease were excluded from the study.
Sonographic Evaluation
All US scans and power Doppler US examinations of the thyroid gland were performed using Samsung MedisonSonoaceX8 with a linear-array transducer (5-12 MHz) that provides enough penetration (about 5 cm depth) and excellent resolution (0.7-1 mm) using an optimised gain. Power Doppler examinations were performed by using the standard equipment settings for thyroid ultrasound. The patient was examined in supine position with the neck hyperextended (a pillow may be placed below the shoulders to achieve neck hyperextension). US features of all of the thyroid nodules were prospectively recorded for clinical use according to the internal component, echogenicity, margins, calcifications, shape and vascularity. Using the modified Russ classification, each nodule was classified into a TIRADS category (I, II, III, IVA, IVB and V) based on the US features [Table/Fig-1] [6]. Based on the results of a previous study marked hypoechogenicity, microcalcifications, irregular margins or microlobulation, and a taller-than-wide shape were counted as suspicious US features [6].
| Category | Features |
|---|
| TIRADS category I | Normal thyroid |
| TIRADS category II | Benign aspect-simple cyst, benign spongiform, isolated macrocalcification and typical subacute thyroiditis |
| TIRADS category III | Probably benign-nodules with none of high suspicious US feature, isoechoic or hyperechoic nodule |
| TIRADS category IVA | Low suspicious-Nodules with no signs of high suspicious US features* and moderately hypoechogenic nodules |
| TIRADS category IVB | High suspicious-Nodules with 1 or 2 suspicious US features* and no metastatic lymphadenopathy |
| TIRADS category V | High suspicious aspects-Nodules with ≥3 suspicious US features* and/or metastatic lymphadenopathy |
| *USG features highly suspicious of Malignancy | taller-than-wide shape irregular or microlobulated margins, microcalcifications, marked hypoechogenicity |
USG Guided FNAC
USG-guided FNAC was performed by the same radiologists who performed the initial scans for each thyroid nodule without administration of local anaesthesia. About 3-4 smears were made for each nodule using 23-gauge needle attached to a 2 mL disposable plastic syringe. Materials obtained from aspiration biopsy were used to prepare smears, immediately placed in 95% ethyl alcohol and sent to the Department of Pathology for papanicolaou staining. Cytopathologists of the hospital interpreted the smears. Reporting of thyroid cytology, FNAC results were classified as benign, indeterminate, suspicious for papillary thyroid carcinoma, malignant, or inadequate [7,8]. Also, those patients who have undergone surgery their histopathological reports were also collected.
Statistical Analysis
All statistical analysis was performed using the statistical software SPSS 22.0 (SPSS Inc, Chicago, USA) and MedCalc 12.7. Sensitivity, specificity, PPV and NPV were calculated for each of the suspicious US features that are highly suggestive of malignancy as described in USG section. The threshold for statistical significance was set at 0.05.
Results
A total of 200 patients were evaluated in present study. FNAC reports showed indeterminate result in ten cases and there was inconclusive report owing to inadequate sampling/technical error in nine patients. Thus, 19 patients were excluded from the study. The age range of the patients in the study was 11 to 75 years. The largest group of patients was in the 21-30 years age group followed by 31-40 years age groups. There were only 3 patients above 70 years. A female preponderance was noted in patients with thyroid nodules in all age groups. There were 169 female and 31 male patients in the study.
Out of 181 patients, 11 nodules (6.07%) were malignant and rest 170 (93.9%) nodules were benign. The majority of the nodules were predominantly solid in its internal content. All of the 11(100%) malignant nodules were predominantly solid and majority of the predominantly cystic nature of the nodules were benign in nature. Majority of the nodules with oval to round shape were benign 154 (90.6%). Microcalcification was more specifically associated with the malignant nodule and seen in the 27.3% cases [Table/Fig-2].
Frequency analysis of USG characteristics of benign and malignant thyroid nodules.
| Characteristics | Benign Nodules | Malignant Nodules |
|---|
| Internal Contents | Predominantly Solid | 130 (76.5%) | 11 (100%) |
| Predominantly Cystic | 40 (23.5%) | 0 (0%) |
| Echogenicity | Anechoic | 11 (6.5%) | 0 (0%) |
| Hypoechoic | 18 (10.6%) | 7 (63.6%) |
| Isoechoic | 118 (69.4%) | 4 (36.4%) |
| Hyperechoic | 23 (13.5%) | 0 (0%) |
| Margin | Smooth | 145 (85.3%) | 5 (45.5%) |
| Spiculated | 0 (0%) | 1 (9.1%) |
| Lobulated | 19 (11.2%) | 1 (9.1%) |
| Ill-defined | 6 (3.5%) | 4 (36.4%) |
| Calcification | Microcalcification | 2 (1.2%) | 3 (27.3%) |
| Macrocalcification | 21 (12.4%) | 0 (0%) |
| Shape | Ovoid to round | 154 (90.6%) | 6 (54.5%) |
| Taller-than-wide | 2 (1.2%) | 3 (27.3%) |
| Irregular | 14 (8.2%) | 2 (18.2%) |
| Vascularity | Peripheral | 85 (50%) | 3 (27.3%) |
| Intranodular | 12 (7.1%) | 3 (27.3%) |
| Both | 40 (23.5%) | 4 (36.4%) |
Specificity of spiculated margin, taller-than-wide shape and hypoechogenicity was 100%, 98.8% and 89.4% respectively showing they were more specifically associated with malignancy. Malignant nodules revealed highest specificity for spiculated margin, followed by microcalcification and taller-than-wide shape as some malignant USG characteristics. However, the sensitivity was low for all these features. Highest sensitivity was noted for predominantly solid nature (100%) for malignant nodules. Highest PPV was noted for spiculated margins (100%). Among the benign USG characteristics anechoic (93.5%) nature showed the highest specificity followed by macrocalcification (87.6%), hyperechoic (86.5%) and predominantly cystic (76.5%) nature [Table/Fig-3].
Diagnostic accuracy of USG findings for malignant and benign nodules.
| Characteristic | Sensitivity (%) | Specificity (%) | NPV (%) | PPV (%) | Accuracy |
|---|
| Malignant nodule |
| Taller-than-wide | 27.3 | 98.8 | 95.5 | 60 | 94.5 |
| Spiculated margin | 9.1 | 100 | 94.4 | 100 | 94.4 |
| Hypoechoic | 63.6 | 89.4 | 97.4 | 28 | 87.9 |
| Predominantly solid | 100 | 76.5 | 100 | 21.6 | 77.9 |
| Micro-Calcification | 27.3 | 98.8 | 95.5 | 60 | 94.8 |
| Benign nodule |
| Anechoic | 0 | 93.5 | 93.5 | 0 | 87.8 |
| Hyperechoic | 0 | 86.5 | 93.1 | 0 | 81.22 |
| Macrocalcification | 0 | 87.6 | 93.1 | 0 | 82.3 |
| Predominantly Cystic | 0 | 76.5 | 92.2 | 0 | 71.8 |
| Peripheral | 27.3 | 50 | 91.4 | 3.4 | 48.6 |
| Isoechoic | 36.6 | 30.59 | 88.1 | 3.28 | 30.9 |
| Smooth | 45.5 | 14.7 | 80.6 | 3.3 | 16.5 |
In present study, TIRADS grading was done based on previously described different ultrasound characteristics used to differentiate benign and malignant nodules. Out of total 181 patients, maximum number of the patients belonged to TIRADS Grade 3 (n=147) (Benign=145 and Malignant=2). TIRADS Grade IVA and IVB had 7 and 8 patients respectively. Out of 181 nodules, the PPV was 100% for Grade V malignant nodules followed by 75% for Grade IVB malignant nodules [Table/Fig-4]. There was significant difference between IVA and IVB malignant nodules with IVA having very low risk for malignancy and IVB having significantly high risk for malignancy.
Distribution of Benign and Malignant nodule in each TIRADS Category with PPV for malignancy.
| Tirads Grading | Total (n=200) | Benign (n=170) | Malignant (n=11) | PPV (%) | NPV (%) |
|---|
| I | 0 | 0 | 0 | 0 | 0 |
| II | 19 | 18 | 0 | 0 | 94.25 |
| III | 159 | 145 | 2 | 1.36 | 82 |
| IVA | 9 | 5 | 2 | 28.57 | 95.5 |
| IVB | 12 | 2 | 6 | 75 | 97.41 |
| V | 1 | 0 | 1 | 100 | 95.2 |
Discussion
Thyroid USG is now increasingly being used to evaluate thyroid diseases to characterise the morphology of the lesion and suggest a pathologic diagnosis. The role has expanded to assess the local extent of the lesions, any nodal involvement and guide FNAC wherever indicated.
In present study, 27.3% of malignant thyroid nodules were of taller-than-wide shape. The sensitivity and specificity of taller-than-wide shape in the detection of malignant lesions were 27.3% and 98.8% respectively. This shows that the taller-than-wide shape has a high specificity for malignancy. In present study irregular shape of the nodule also shows high specificity (98.8%). Result of current study is in consistent with the study conducted by Moon WJ et al., [9].
Gaitini D et al., described that the risk of malignancy was more with solid nodule [10]. Our experience shows that all the malignant nodules were solid and all the cystic nodules were benign in nature. however, 3/4th of the benign nodules were also solid in consistency. Thus in solid lesions, we need to see other feature which might suggest malignancy. In the present study, there was one case of intacystic intracystic papillary carcinoma which had cystic internal consistency with large internal solid component. FNAC was taken from the solid area and diagnosed to be a malignant intracystic papillary neoplasm. Hypoechogenicity was noticed in 63.6% of the malignant nodule with the sensitivity and specificity of 63.6% and 89.4% respectively whereas hypoechogenicity seen in 10.6% cases of benign nodules. Hypoechogenicity was more specifically associated with the malignancy. Moon WJ et al., and Gaitini D et al., in their study reported that the frequency of hypoechogenicity was significantly different between benign and malignant nodules and hypoechogenicity was highly specific for diagnosing malignant nodules [9,10].
Out of the 11 proven malignant nodules, 5 (45.5%) had smooth margin followed by ill-defined margin which was seen in 4 cases (36.4%). However, sensitivity and specificity of spiculated margin in the detection of malignant nodule was 9.1% and 100% respectively. This shows that spiculated margin is highly specific feature of a malignant nodule. Moon WJ et al., reported similar result with sensitivity of 48.3% and specificity of 91.8% for speculated margin in the detection of malignant nodule [9].
In the current study, 3 cases (27.3%) of malignant nodules showed microcalcification whereas (1.2%) benign nodules showed microcalcification. Microcalcification was more specifically associated with the malignant nodule and seen in the 27.3% cases with sensitivity and specificity of 27.3% and 98.8% respectively. Moon WJ et al., reported that the microcalcifications have a high PPV (41.8%-94.2%) but a low sensitivity (26.1%-59.1%) in the detection of malignant nodule [9]. In present study the PPV of microcalcification for the diagnosing malignant nodule was 60.0% and macrocalcification showed high NPV of 93.1% [Table/Fig-5,6].
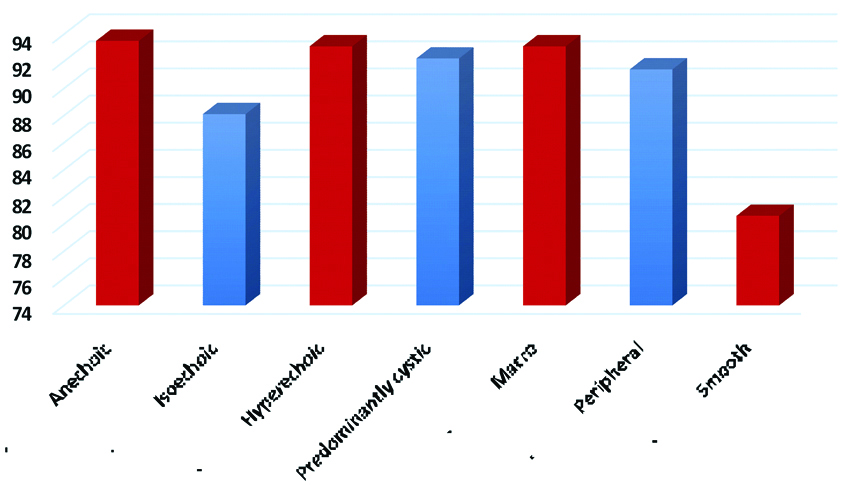
Positive predictive value (PPV) for malignancy of various USG characteristics.
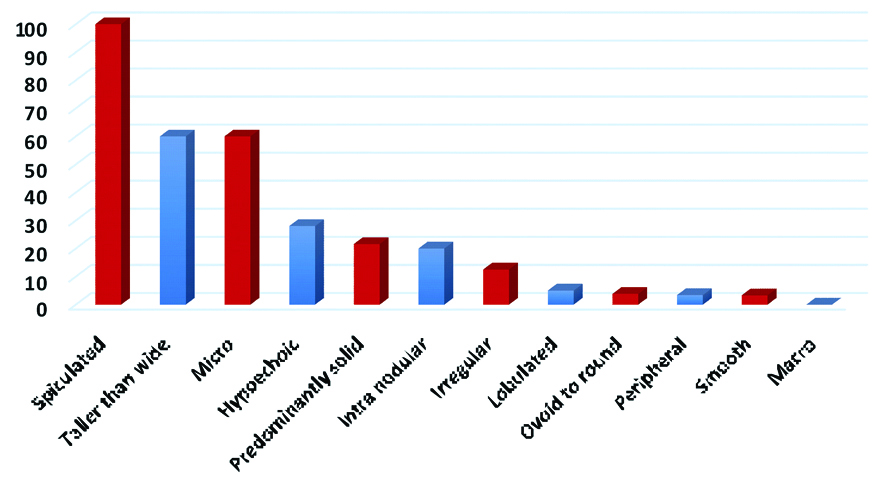
Negative predictive value (NPV) for malignancy of various USG characteristics.
Kim BM et al., previously reported the same result that hypoechogenicity, marked hypoechogenicity, and taller-than-wide shape were the ultrasound features which best predicted the chance of malignancy in thyroid nodules [8]. These features were considered to be suspicious for malignancy in study conducted by Kwak JY et al., Nam-Goong IS et al., Salmaslioglu A et al., and Tae HJ et al., [7,11-13].
Some investigators suggest a combination of these features is known to provide better diagnostic accuracy than a single feature alone. However, considerable variation in the sensitivity and specificity of the US findings for malignant thyroid nodules are reported. Factors that may affect the findings reported in previous studies include the use of different USG equipment, operator’s experience and the different US criteria for identifying a malignancy.
Comparing the diagnostic performance of TIRADS in the present study with other studies [Table/Fig-7]. The studies done by Hovarth E et al., Kwak JY et al., Kim BM et al., Park JY et al., Moifo B et al., and Chandramohan A et al., show that the risk of malignancy increases as we advance the grading of TIRADS from Grade III to Grade V [5,7,8,14-16]. The result shows that present study for TIRADS Grade II, IVA, IVB and V is correlating with the other studies while present study for TIRADS Grade III is correlating with the study of Kwak JY et al., [7]. In present study, it was also noted that there is substantial increase in the risk of malignancy (i.e., from 28.57% to 75%) was noted from TIRADS Grade IVA to Grade IVB and V. Any lesion with Grade IV and V should always be biopsied because the overall risk of malignancy is very high.
Comparison of the diagnostic performance of the present study with other studies on the performance of TIRADS showing percentage risk of malignancy with various TIRADS categories.
| TIRADS Category | Horvath E et al., [5] | Kwak JY et al., [7] | Kim BM et al., [8] | Park JY et al., [14] | Moifo B et al., [15] | Chandramohan A et al., [16] | Current Study |
|---|
| TIRADS 2 | 0 | 0 | 0 | 1.8 | 0 | 0 | 0 |
| TIRADS 3 | 14.1 | 1.5 | 0 | 9.6 | 2.2 | 6.6 | 1.36 |
| TIRADS 4A | 45.0 | 3.9 | 34.1 | 31.1 | 5.9 | 32 | 28.57 |
| TIRADS 4B | | 69.3 | 83.9 | 76.8 | 57.9 | 36 | 75 |
| TIRADS 5 | 89.6 | 74.9 | 99.4 | 100 | 100 | 64 | 100 |
Limitation
The major limitation of the study was that in present study we encounted only 11 confirmed nodules of malignancy. However, the results are consistent with the few published papers. The benign lesions were not operated because of consent and ethical issues.
Conclusion
USG is the best diagnostic tool in the assessment of thyroid nodules. The number of diagnosed non palpable thyroid nodules is increasing as a consequence of the widespread use of USG. Among all the clinically palpable lesions, incidence of malignancy is low. Therefore, it becomes very important to differentiate benign from malignant nodules and to guide FNAC of nodules suspected for malignancy. There are combinations of USG features that can suggest the possibility of malignancy. TIRADS serves as a convenient classification system which can guide the clinicians to biopsy the TIRADS IV and V nodules, thus helping in better patient management.