Eyelid Discoid Lupus Erythematosus Misdiagnosed as Leishmaniasis
Amir Feily1, Farhang Houshmand2, Marigdalia K Ramirez-Fort3
1 Dermatologist, Department of Dermatology, Skin and Stem Cell Research Center, Tehran University of Medical Sciences, Tehran, Iran.
2 Dermatopathologist, Department of Pathology, Jahrom University of Medical Sciences, Jahrom, Iran.
3 Senior Resident, Department of Radiation Oncology, Medical University of South Carolina, South Carolina, USA.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Amir Feily, Dr. Feily Clinic of Dermatology, Skin and Stem Cell Research Center, Tehran University of Medical Sciences, Tehran, Iran; Moalem BLVD, Jahrom, Fars, Iran.
E-mail: dr.feily@yahoo.com
A 42-year-old man presented to the clinic of Dermatology and Hair Transplantation, with a two-year history of right eyelid scarring and associated eyelash alopecia. Upon initial presentation of the patient’s symptomatology, he had a positive smear test for leishmania. Therefore, he was diagnosed and treated for eyelid leishmaniasis with several rounds of cryotherapy and glucantim for two years; his lesions were refractory to this initial therapy.
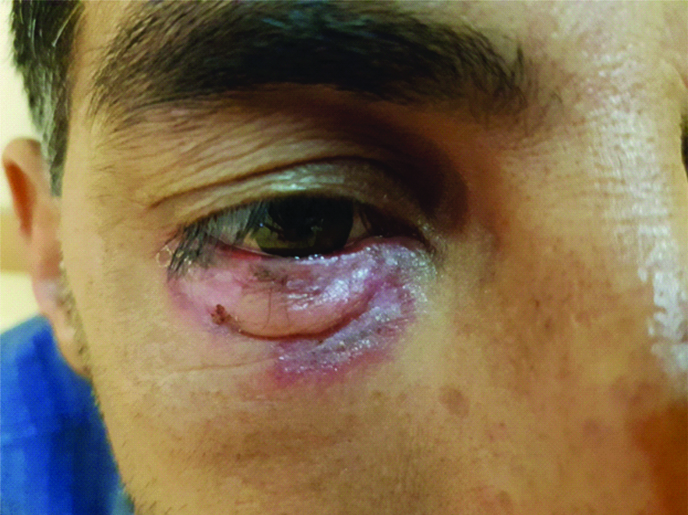
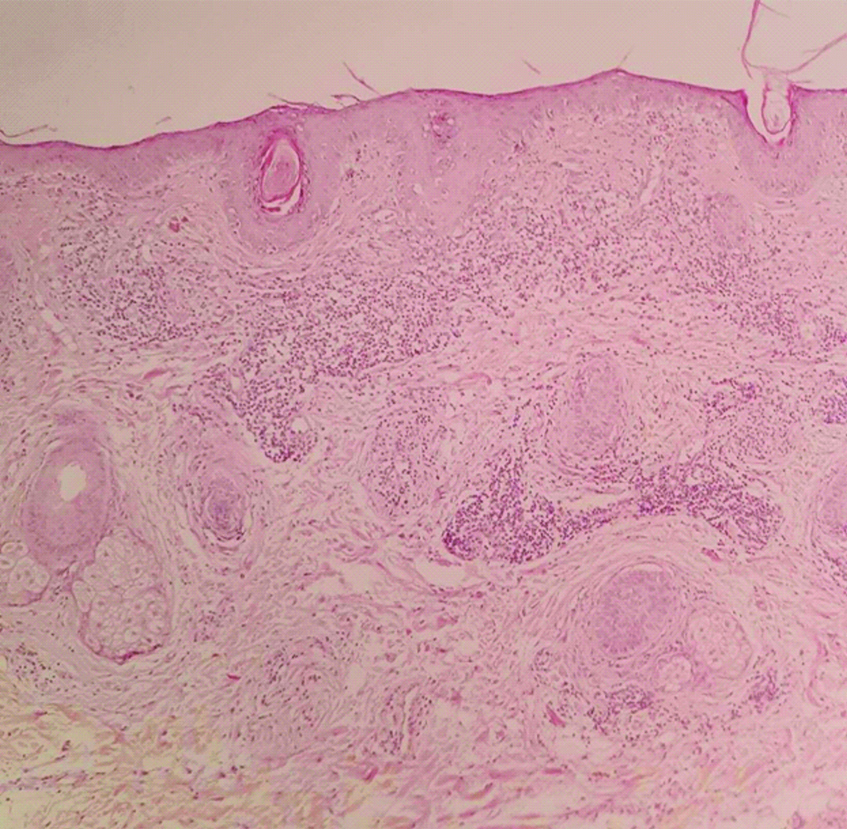
General physical examination was unremarkable. Right eye examination revealed, periocular erythematous, oedematous plaques with active borders, central scarring and lower lid madarosis [Table/Fig-1]. There was no other skin lesion on the body. The lesion was clinically suspicious for cutaneous lupus and a biopsy was performed. Histopathological analysis confirmed Discoid Lupus Erythematosus (DLE) [Table/Fig-2]. Specifically, the sections showed hyperkeratosis with follicular plugging. Thinning and flattening of the stratum Malpighi with focal hydropic degeneration of the basal layer was identified. A brisk perivascular and periadnexal mononuclear lymphocytic infiltrate with some admixed melanophages, around hair follicles was seen. Vasodilation of upper dermal vessels was also present.
Right eyelid examination; periocular erythematous, oedematous plaques with active borders, central scarring and lower lid madarosis.
The skin lesion biopsy (H&E staining; Low power).
The patient was successfully treated with hydroxychloroquine 200 mg BID and prednisolone 15 mg daily, resulting in lesional resolution in six months [Table/Fig-3].
Successful treatment of the patient with hydroxychloroquine and prednisolone and lesional resolution in six months.

DLE is a chronic, autoimmune disorder that is limited to the skin; morphologically, DLE presents with characteristic acute erythema and discoid lesions [1]. Rarely does DLE involve the eyelid and periocular region [2]. Early diagnosis of DLE is important towards initiating the correct treatment and prevention of permanent scarring and discolouration [1,2]. The differential diagnosis of periocular DLE includes: psoriasis, rosacea, lupus vulgaris, sarcoidosis, Bowen’s disease, polymorphous light eruptions, lichen planopilaris, dermatomyositis, granuloma annulare, granuloma faciale and leishmaniasis [2]. There are many misdiagnosed cases in the literature based on the clinical similarities of the aforementioned conditions [3-6]. Similarly, the present patient’s treatment was delayed due to an incorrect laboratory-based diagnosis, without noticing the clinical signs. A higher index of suspicion for DLE could have accelerated the biopsy and correct management; the presented clinical scenario, emphasises the importance of physical examination and histopathological examination in dermatological diagnoses.
Patient’s consent was obtained before publishing the clinical images.
[1]. Uva L, Miguel D, Pinheiro C, Freitas JP, Gomes MM, Filipe P, Cutaneous manifestations of systemic lupus erythematosusAutoimmune Dis 2012 2012:83429110.1155/2012/83429122888407 [Google Scholar] [CrossRef] [PubMed]
[2]. Yaghoobi R, Feily A, Behrooz B, Yaghoobi E, Mokhtarzadeh S, Palpebral involvement as a presenting and sole manifestation of discoid lupus erythematosusScientific World Journal 2010 10:2130-31.10.1100/tsw.2010.20921057726 [Google Scholar] [CrossRef] [PubMed]
[3]. Sisti A, Fallaha A, Tassinari J, Nisi G, Grimaldi L, Eisendle K, Melanoma in situ mimicking a Lichen planus-like keratosisActa Biomed 2018 88:496-98. [Google Scholar]
[4]. Yaghoobi R, Feily A, Ranjbari N, Lotfi J, Yaghoobi E, Lepromatous leprosy: a commonly misdiagnosed diseaseScientific World Journal 2010 10:2348-49.10.1100/tsw.2010.206 [Google Scholar] [CrossRef]
[5]. Maor D, Ondhia C, Yu LL, Chan JJ, Lichenoid keratosis is frequently misdiagnosed as basal cell carcinomaClin Exp Dermatol 2017 42:663-66.10.1111/ced.1317828636260 [Google Scholar] [CrossRef] [PubMed]
[6]. Feily A, Namazi MR, Seifmanesh H, Generalized pustular psoriasis-like dermatophytosis due to Trichophyton rubrumActa Dermatovenerol Croat 2011 19:209-11. [Google Scholar]