Materials and Methods
This observational study was done in the Department of Anatomy, Christian Medical College, Vellore, Tamil Nadu, India. The study was done over a period of 18 months from October 2015 to March 2017. Ethical clearance from Institutional Review Board of the institution was obtained. Thirty five formalin fixed cadavers (Male 22; Female 13) donated to the Department of Anatomy of the institution for the purpose of teaching and research was used for the study. Foot length was measured from the most posterior point of the heel to the tip of great toe using standard anthropometric instruments. Dissection was done on the dorsum of foot of both right and left side. The skin over the dorsum of the foot was removed extending from the ankle to web spaces of toes. In all the 70 limbs the NVB, EHBMT junction and the first and second tarsometatarsal joints was identified. The relationship of the NVB to the neighbouring structures like the tendons of extensor hallucis longus and extensor digitorum longus was observed from distal border of extensor retinaculum to the first web space. The relationship of NVB to the EHB muscle was specifically looked into. The length of the transition zone of EHB was measured by using digital vernier caliper.
Statistical Analysis
Pearson correlation coefficient p-value ≤0.05 was considered significant between the length of the foot and length of musculotendinous junction of EHB using SPSS version 16.0.
Results
In the dorsum of foot, proximally the NVB was present between the tendons of EHL and EDL. In the middle it passed behind the EHB. Distally the NVB was present between the extensor hallucis longus and Extensor hallucis brevis tendons medially and the tendon of extensor digitorum longus to the second toe laterally [Table/Fig-1]. The relationship of medial branch of DPN and DPA in the NVB varied at the level of distal border of extensor retinaculum. In 30 out of 70 feet (42.85%) the DPN was medial to DPA [Table/Fig-1] and in 40 feet (57.14%) it was lateral to DPA [Table/Fig-2].
Left dorsum of foot showing the presence of neurovascular bundle (NVB) between the tendons of Extensor Hallucis Longus (EHL) and Extensor Digitorum Longus (EDL).
Note: The deep peroneal nerve (white arrow) is medial to the dorsalis pedis artery (black arrow). The distance between the two asterisks indicates the length of musculotendinous junction of Extensor Hallucis Brevis (EHB).

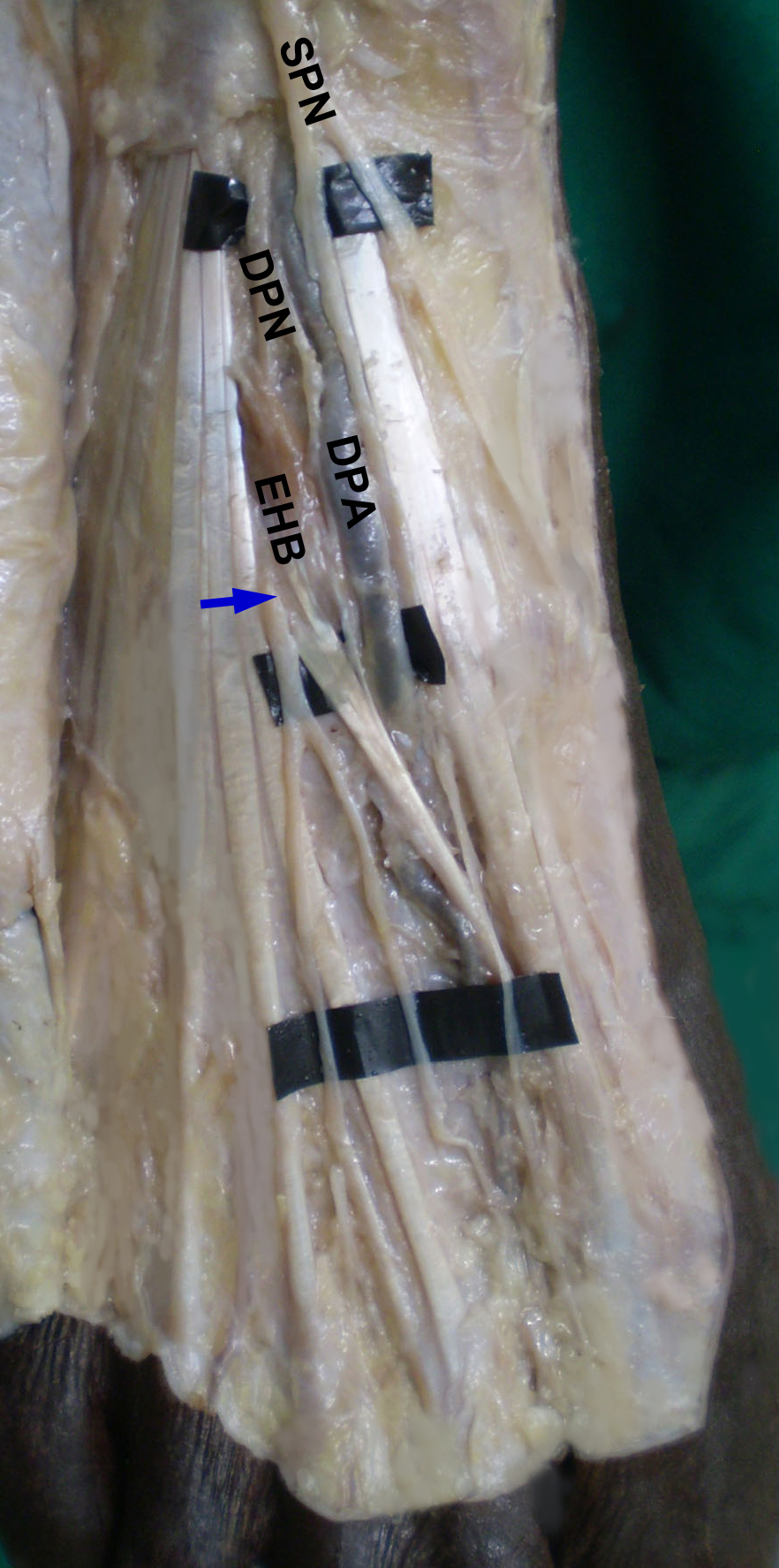
Right dorsum of foot showing the presence of DPA medial to the DPN.
Note: The DPN (blue arrow) piercing EHB and DPA passing behind the musculotendinous junction of EHB, SPN.
The length of EHB musculotendinous junction ranged from 10.43 to 16.92 mm and was significantly longer in males (p= 0.02). The mean foot length was also significantly longer in males (p < 0.001) [Table/Fig-3]. There was a positive correlation between foot length and EHBMT junction, which was statistically significant (p< 0.05).
Measurement of EHBMT junction length (EHBMT JL) and foot length.
| Minimum length (mm) | Maximum length (mm) | Mean (mm) | Standard Deviation | p-value |
|---|
| M | F | M | F | M | F | M | F |
|---|
| EHB MT JL | 10.65 | 10.43 | 16.92 | 15.28 | 13.7 | 12.9 | 1.46 | 1.23 | =0.02 |
| Foot Len-gth | 195 | 195 | 250 | 230 | 223.7 | 209.3 | 12.38 | 9.36 | <0.001 |
In 68 out of seventy specimens (97.14%), NVB was found consistently behind the EHB musculotendinous junction [Table/Fig-1]. Two specimens on the right side showed the medial branch of DPN piercing the EHB muscle proximal to the musculotendinous junction. However, the DPA passed behind the musculotendinous junction [Table/Fig-2].
Discussion
Surgical approaches of dorsum of foot are important for different conditions ranging from elective arthrodesis procedure to traumatic injuries like Lisfranc or tarsometatarsal joints [6]. During any surgical procedure, care must be taken to avoid injuries to the NVB present in that region. The anterocentral portal in ankle arthroscopy has a high risk of DPN injury [7,8]. It has been reported that the incidence of neuroma formation following midfoot surgeries is 6-8% due to injury to medial branch of DPN [9]. In addition, injury to the DPN in foot can occur due to trauma or repetitive mechanical irritation. In anterior tarsal tunnel syndrome, compression of DPN occurs inferior to the extensor retinaculum [10]. However, the nerve is most susceptible to iatrogenic injury along its more distal anatomic course [4].
There are studies that described the relationship between the DPN and DPA in the foot [5,11]. Standard gross anatomy textbooks describe that the DPN lies lateral to DPA [2]. Study done by Rab M et al., showed that in 26 out of 28 feet, the DPN was positioned posterolateral to the accompanying DPA at the level of inferior extensor retinaculum [11]. The present study indicated that the DPN may lie on the lateral aspect of DPA at a higher incidence (57.14%). In 30 out of 70 feet (42.86%), DPN was medial to DPA which is in accordance with Ranade AV et al., who reported in 32.4% where the DPN was medial to the DPA [5].
In the present study, there was a statistically significant correlation between the foot length and the length of musculotendinous junction of EHB which is in contrast with Loveday DT et al., who reported no correlation between the two parameters [3].
Although, studies describing the relationship between DPN and DPA have been done by various authors like Lawrence SJ and Botte MJ [4], the relationship of the NVB to the musculotendinous junction of EHB has been described in only one previous study [3]. In the present study, in 68 out of 70 feet (97.14%), the NVB passed behind the EHB musculotendinous junction and in the remaining two feet (2.85%) medial branch of DPN pierced the muscle proximal to the musculotendinous junction. This finding is in accordance with Loveday DT et al., who reported 9 out of 10 limbs (90%) NVB passed behind the EHB musculotendinous junction and in the remaining one limb (10%) DPN passed between the muscle belly of EHB [3]. During trauma, bruising, inflammation or in any other deformed conditions of the foot, identification of this NVB is difficult due to unclear normal anatomy. Similar problem occurs while approaching elective conditions like osteophytes, cyst or subluxation of joint. In such conditions, musculotendinous junction of EHB and the underlying NVB are easy to locate either by tracing the muscle from proximal or the tendon from distal aspect [3]. Thus the musculotendinous junction of EHB is found out to be the reliable landmark to identify NVB in all surgical approaches involving dorsum of midfoot [3].
Limitation
The limitation of the present study was the small sample size.
Conclusion
The relationship of the NVB to the musculotendinous junction of EHB is reliable and reproducible and therefore, EHBMT junction can be used as a landmark to identify the DPN.