Chronic Unresolved Haematoma of Thigh with Acute Expansion- Emulating Neoplasm
Pankaj Kumar Mishra1, Pratyush Goyal2, Manish Kumar Verma3, Deepak Singh Maravi4, Aashish Gohiya5
1 Assistant Professor, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
2 Student, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
3 Student, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
4 Professor, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
5 Professor, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pankaj Kumar Mishra, E- 115/4 Shivaji Nagar, Bhopal-462016, Madhya Pradesh, India.
E-mail: drpankajv@yahoo.com
Chronic haematoma formation and its acute expansion are rare in clinical scenario. Its clinical presentation may simulate to malignant soft tissue lesion. Usually they remain inactive for long time but sometimes shows sudden spurt of growth. The accepted treatment is excision of the haematoma. Here we are presenting the chronic haematoma of thigh in young boy, which remained dormant for years. But until recently it became huge and rendered the surgeon in dilemma for diagnosis making, which was managed after clinico-radiological evaluation. Here we are sharing our experience of a young patient with acutely expanded huge haematoma swelling which emulated to neoplasm.
Excision, Swelling, Treatment
Case Report
A 10-year-old male presented to our hospital with a huge, pumpkin size swelling over his left posterior aspect of the thigh. The father of patient stated that swelling appeared about three years back. Initially, it was painless and gradually increased in size since the last six months. The swelling was asymptomatic and did not bother in day to day activities. He did not get any consultation for it previously. Three weeks, prior to the visit to the hospital, the swelling had increased in size rapidly, attaining the size of about 35 x 25 cm. This prompted the patient to seek medical attention.
On examination, there was a gross swelling occupying the distal three fourth of postero-lateral aspect of the left thigh [Table/Fig-1]. It was spherical in shape with smooth margin and shiny skin with engorged veins. There were no other associated features with swelling i.e., history of trauma, bleeding dyscrasia and significant family or past history. On palpation, it was non-tender, with local rise of temperature, boggy, smooth in consistency, compressible (but not-reducible), non-adherent to skin and free from the underlying bone. Range of movement at left knee and hip joint was normal. Clinically the base of swelling was not felt, and the swelling was unaffected by the muscle contractions.
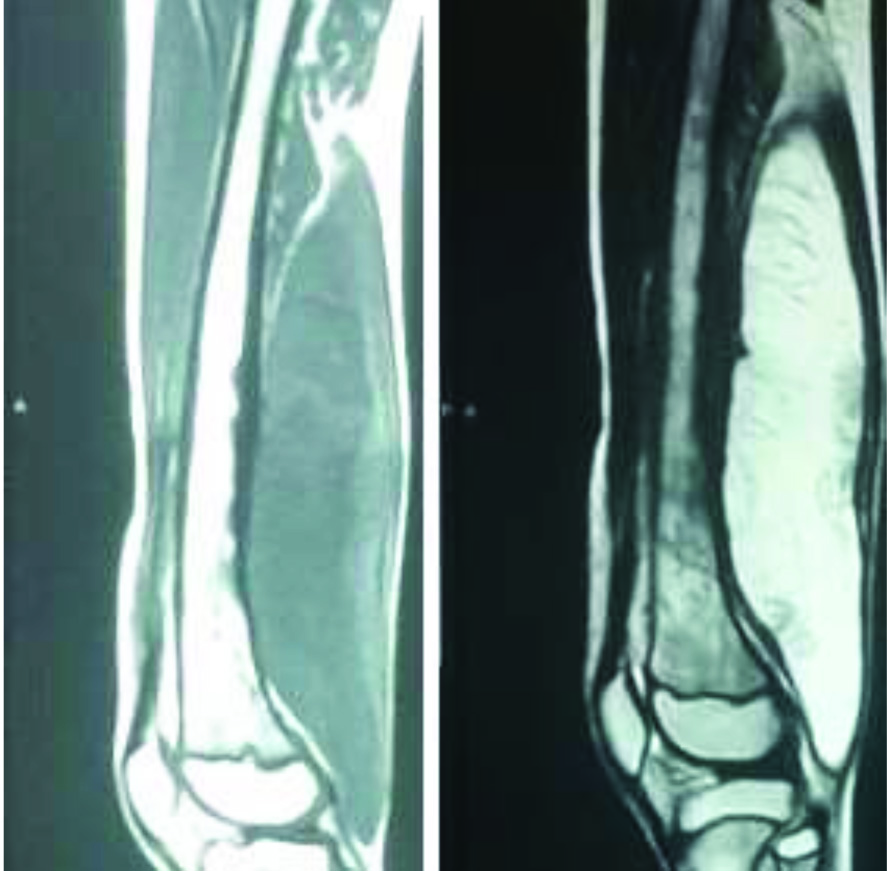
After clinical examination, antero-posterior and lateral X-rays [Table/Fig-2] showed the scalloping effect of the cortex over the postero-lateral aspect of femur. Furthermore the clinico-radiological differential diagnosis of pseudotumor, haemangioma, abscess and sarcoma were considered. MRI of the left thigh revealed the well defined cystic lesion with fluid intensity in a deep posterior muscle compartment of middle and distal thigh [Table/Fig-3]. Within the mass the fluid debris level was seen, so the chronic haematoma was conceded as the final diagnosis.
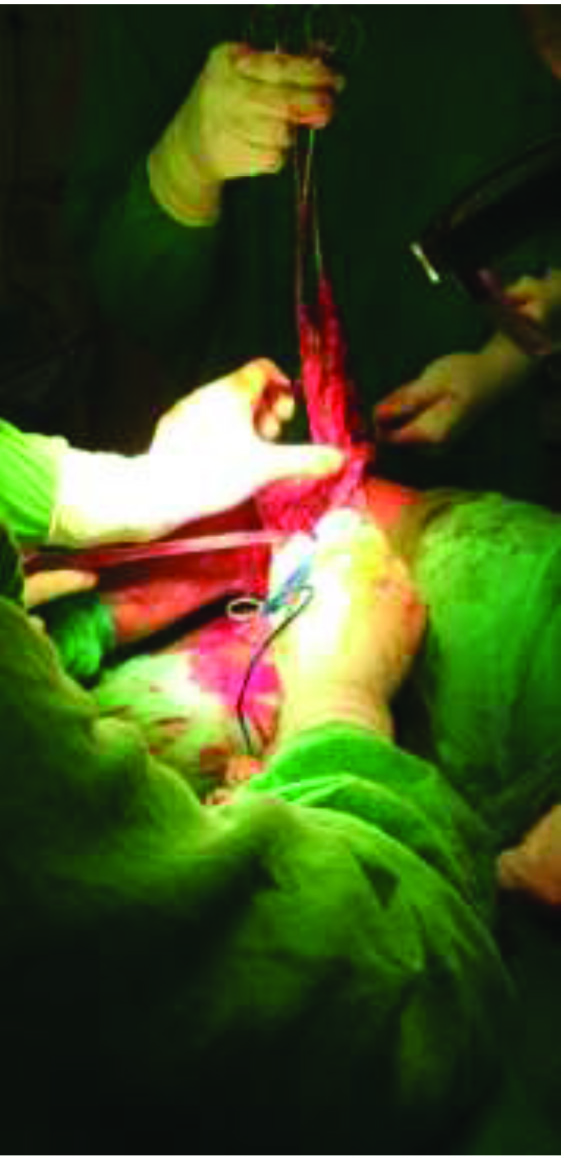
After informed consent, excisional biopsy was planned. In prone position, posterior midline longitudinal incision was given, then the mass was excised along the pseudo-capsule taking care of neuro-vascular structure, and closed under drain by cutaneofascial sutures. Since the pseudo-capsule was adherent to nearby neuro-vascular bundle, it was not feasible to dissect it completely. So we left the some part of its cystic wall [Table/Fig-4]. Biopsy finding displayed the cholesterol clefts, middle zone of eosinophilic material, inner zone of granulation tissue and haemosiderin pigmentation, which clinched the diagnosis of chronic haematoma. Postoperative period was un-eventful and sutures were removed at 10th postoperative day. At the end of about one year of follow-up, patient was symptom free and had the normal looking limb.
Posterior and lateral view respectively showing the extension of swelling.

Scalloping effect of mass over postero-latarel part of distal femur.

T1 and T2 weighted MRI respectively showing the well defined cystic lesion with fluid intensity in deep posterior muscles of thigh.
Near complete resection of swelling along the pseudo-capsule due to adherence to surrounding neuro-vascular structure.
Discussion
In unusual paradigm the chronic haematoma formation and its acute expansion is not well understood. They remain dormant for a long time, but their importance lay in its sudden growth and mimicry to soft tissue malignant lesions. Usual side of chronic expanding haematoma is thigh, followed by calf area [1]. Here we are presenting a case of chronic haematoma, which became painful and expanded in size in short intervals. The clinical presentation of swelling installed the unusual differential diagnosis and experience.
Reid JD et al., coined the term chronic expanding haematoma which is persistent and keep on increasing in size even after the one month of initial haemorrhage [2]. Traumatic displacement of skin and subcutaneous tissue from underlying fixed fascia resulted in a blood filled cysts, is the most common mechanism [3].
Usually haematoma gets absorbed with the time, but if it’s huge then it gets encapsulated by fibrous wall and persists as a chronic swelling [4]. Sometimes the persistent chronic haematoma expands. The authors have produced various mechanisms to explain the sudden expansion of dormant haematoma. One such mechanism is a breakdown of haematoma product, resultant high osmotic pressure gradient which cascade the local inflammatory progression [5]. Another theory states that vasoactive substance and factor of coagulation pathway are responsible for inflammatory reaction which ultimately causes bleeding from fragile vessels. Finally, this additional bleeding again by inflammation perpetuates the vicious cycle [6,7].
The accepted treatment for unresolved haematoma is excision of the haematoma with pseudocapsule [8,9]. But a few cases have reported the recurrence of it, even after the marginal resection [10]. However, the total excision of the haematoma is not always feasible. Enormous vascularization and adhesion of pseudocapsule to adjacent structures makes it reportedly difficult [11]. So in literature, it has been advocated to leave the pseudocapsule in situ to avoid the injury of surrounding vital structures [12].
In our case the pseudocapsule was adherent to the adjacent fascia and nerve (sciatic nerve); and the dissection of the nerve was not feasible. Due to deep involvement of haematoma, probably leaving the pseudocapsule could have avoided the neurological deficit, but it may not have been adequate for management.
Conclusion
Only clinical finding cannot delineate between a chronic, unresolved haematoma and underlying neoplasm. Conventional approach by X–ray is only helpful to rule out any fracture or bony mass. MRI is the most valuable diagnostic method to evaluate the chronic expanding haematoma. T2-weighted imaging displays the heterogeneous signal intensity. There is high-signal intensity at central zones of fluid collection and a peripheral low-signal rim of thick pseudo capsule. Surgical excision is the mainstay of treatment. Adhesion to the adjacent tissue (neurovascular) must be anticipated prior to surgery, especially for a deep located lesion and must be dealt accordingly.
[1]. Negoro K, Uchida K, Yayama T, Kokubo Y, Baba H, Chronic expanding hematoma of the thighJoint Bone Spine 2012 79(2):192-94.10.1016/j.jbspin.2011.08.00221944978 [Google Scholar] [CrossRef] [PubMed]
[2]. Reid JD, Kommareddi S, Lankerani M, Park MC, Chronic expanding haematomas; a clinico pathologic entityJAMA 1980 244(21):2441-42.10.1001/jama.1980.033102100430266448929 [Google Scholar] [CrossRef] [PubMed]
[3]. Bradshaw JR, Davies GT, Edwards PW, Richards HJ, The radiological demonstration of traumatic cysts due to severe soft tissue traumaBr J Radiol 1972 45:905-10.10.1259/0007-1285-45-540-9054647140 [Google Scholar] [CrossRef] [PubMed]
[4]. Imaizumi S, Morita T, Ogose A, Hotta T, Kobayashi H, Ito T, Soft tissue sarcoma mimicking chronic hematoma: value of magnetic resonance imaging in differential diagnosisJ Orthop Sci 2002 7:33-37.10.1007/s776-002-8410-511819129 [Google Scholar] [CrossRef] [PubMed]
[5]. Lim-Hing K, Rincon F, Secondary hematoma expansion and perihaemorrhagic edema after intracerebral haemorrhage: from bench work to practical aspectsFront Neurol 2017 8:7410.3389/fneur.2017.0007428439253 [Google Scholar] [CrossRef] [PubMed]
[6]. Sreenivas M, Nihal A, Ettles DF, Chronic haematoma or soft tissue neoplasm? A diagnostic dilemma!Arch Orthop Trauma surg 2004 124:495-97.10.1007/s00402-004-0698-x15248076 [Google Scholar] [CrossRef] [PubMed]
[7]. Labadie EL, Glover D, Physiopathogenesis of subdural haematomas. Histological and biochemical comparisons of subcutaneous haematoma in rats with subdural haematoma in manJ Neurosurg 1976 45:382-92.10.3171/jns.1976.45.4.0382956874 [Google Scholar] [CrossRef] [PubMed]
[8]. Muramatsu T, Shimamura M, Furuichi M, Ishimoto S, Ohmori K, Shiono M, Treatment strategies for chronic expanding hematomas of the thoraxSurgery Today 2011 41(9):1207-10.10.1007/s00595-010-4462-221874416 [Google Scholar] [CrossRef] [PubMed]
[9]. Babu VL, Rana MM, Arumilli BR, Dean T, Brown C, Paul A, Chronic expanding hematomas with interesting presentationsIowa Orthop J 2007 27:108-11. [Google Scholar]
[10]. Okada K, Sugiyama T, Kato H, Tani T, Chronic expanding hematoma mimicking soft tissue neoplasmJ Clin Oncol 2001 19:2971-72.10.1200/JCO.2001.19.11.297111387374 [Google Scholar] [CrossRef] [PubMed]
[11]. Takanami I, Successful treatment of huge chronic expanding hematoma after thoracoplastyJ Thorac Cardiovasc Surg 2003 126:1202-03.10.1016/S0022-5223(03)00787-6 [Google Scholar] [CrossRef]
[12]. Roper CL, Cooper JD, Chronic expanding hematoma of the thoraxJ Thorac Cardiovasc Surg 2001 122:1046-48.10.1067/mtc.2001.11761711689822 [Google Scholar] [CrossRef] [PubMed]