Healthcare organisations are accountable to address the needs of the population. Estimates from global burden of disease demonstrate, that oral diseases affect 3.9 billion people [1]. Additionally, oral diseases significantly affect quality of life and impact social and psychological well-being, consequently leading to social isolation.
With the advent of newer technologies and materials, dentistry has seen a paradigm shift in recent times. It is need of the hour to make these latest treatment options accessible to all groups of population. Keeping this in mind, the CoE at VSPMDCRC Nagpur, India was started in 2016 to cater to oral healthcare in rural Indian population. Another aim of this initiative was to foster organisational development through an integrated approach. The long-term objective for establishing the CoE was to stand out as a pioneer in Central Indian region in the respective fields.
A CoE may be described as an organisational environment that strives for and succeeds in developing high standards of conduct in a field of research, innovation and learning [7,8]. The CoE at VSPMDCRC focuses on economically disadvantaged groups in rural geographies and can be classified as a direct service intervention program for comprehensive oral healthcare.
The present CoE model was planned and executed with consensus building for 12 months using several methods to involve stakeholder groups (staff, students and patients). These included clinicians, researchers, managers and patients from the institute. The CoE comprised of two working units as:
These two units involved faculty, consultants and post-graduate students. Detailed prospective planning was done for development and working of these units with specific targets and milestones to be achieved, in a stipulated timeframe. Main thrust areas common for both of them included:
Although many institutes are working towards oral healthcare in India, reports have not been found in literature regarding their functioning and effectiveness of the program. Assessing the centre of excellence can stimulate continuous improvement in the way the institute perceives, plans, and performs treatment for the benefit of patients. It can also help to develop a network of future excellence centres that can focus their collaboration and share best practices through regular benchmarking.
Thus, the present article was aimed to preliminarily evaluate the impact of CoE through an assessment framework that was developed using a consensus building exercise with stakeholder groups and experts and present an evaluation report for the same.
Materials and Methods
The present study was designed as a cross-sectional survey at VSPMDCRC, Nagpur for a period of 2 years (June 2015 to June 2017). Formal inauguration of the centre took place in January 2016 (established), however, planning and ground work started 6 months prior.
Assessment of Functioning Framework and Analysis at the End of One Year
A literature search was carried out using the terminology; Centre of excellence, expert centre and oral healthcare using Boolean characters in PubMed for the last 10 years (2007-2017). No published data was found on any centre of excellence for oral healthcare in rural population. Also, no assessment framework and evaluation has been specifically focused and researched. So, an innovative framework using logic model [9] was designed and quantitative data was collected under following headings, [Table/Fig-1].
Logic model based evaluation framework (quantitative analysis).
| S No. | Topic | Sub-topic |
|---|
| 1 | Inputs | Funds and other resources |
| 2 | Activities | Clinical patient inflow |
| Academic publications and research |
| Outreach (Continuing dental education workshops, camps) |
| 3 | Outputs | Short-term (at the end of 1 year) |
Qualitative data was collected using personal interviews and structured validated questionnaires (https://www.cdc.gov/eval/guide/introduction/index.htm) for assessing implementation, effectiveness, efficiency, cost-effectiveness and attribution of the CoE in the following format [Table/Fig-2]. Eight staff were interviewed, Professors, Associate professors, Senior lecturers, Clinical assistants/tutors (two each):
Qualitative data assessment questionnaire.
| S No. | Topic | Question | Answers |
|---|
| 1 | Implementation | Were your program activities put into place as originally intended | |
| 2 | Effectiveness | Is your programme achieving the goals and objectives it was intended to accomplish? | |
| 3 | Efficiency | Is your program being produced with appropriate use of resources such as budget and staff time? | |
| 4 | Cost-effectiveness | Does the value or benefit of achieving your program goals and objectives exceed the cost of producing them? | |
| 5 | Attribution | Can progress on goals and objectives be shown to be related to your programme, as opposed to other things that are going on at the same time? | |
The overall impact was categorised and discussed as per the following excellence criteria’s (modified based on Boyer’s model of scholarship) [10,11]:
Criteria 1: Academics
Criteria 2: Research
Criteria 3: Clinical
Criteria 4: Faculty development
Criteria 5: Technology
Criteria 6: Social
Quantitative Data Analysis
The data was collected and analysed using Microsoft Excel based on frequency charts and quantitative values. The obtained data gave information about the working units of CoE in the institute for one year.
Results
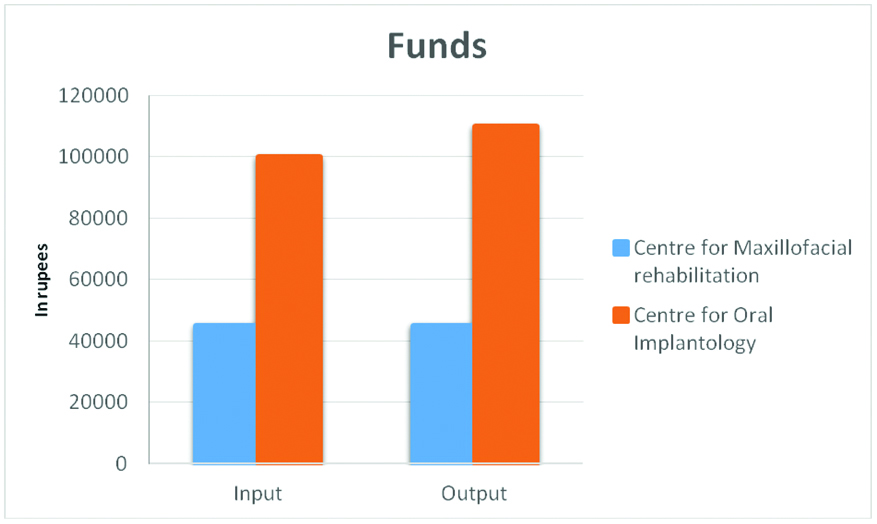
Allocated funds were sufficient for the development and working of units in the first year. Furthermore, the research proposals secured additional funds from state government university. Consultants who were experts in the field of maxillofacial rehabilitation and oral implantology across the country were invited to conduct training programmes for faculty and student capacity building in the present institute.
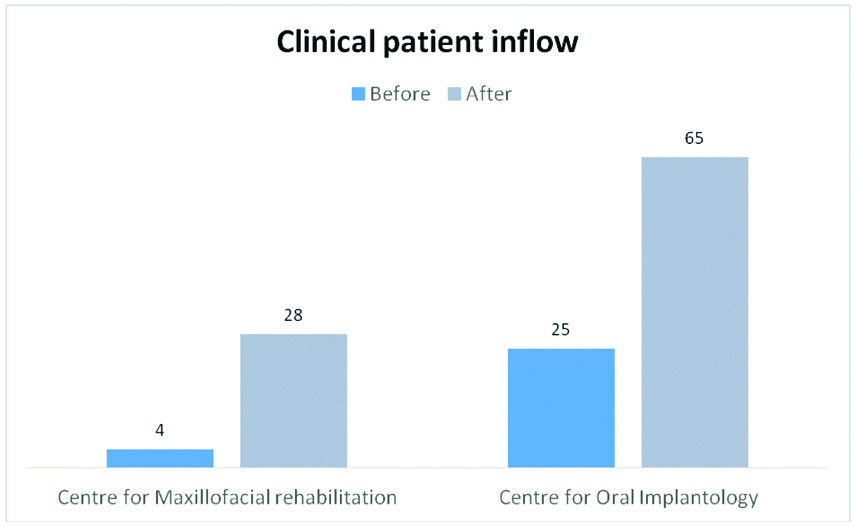
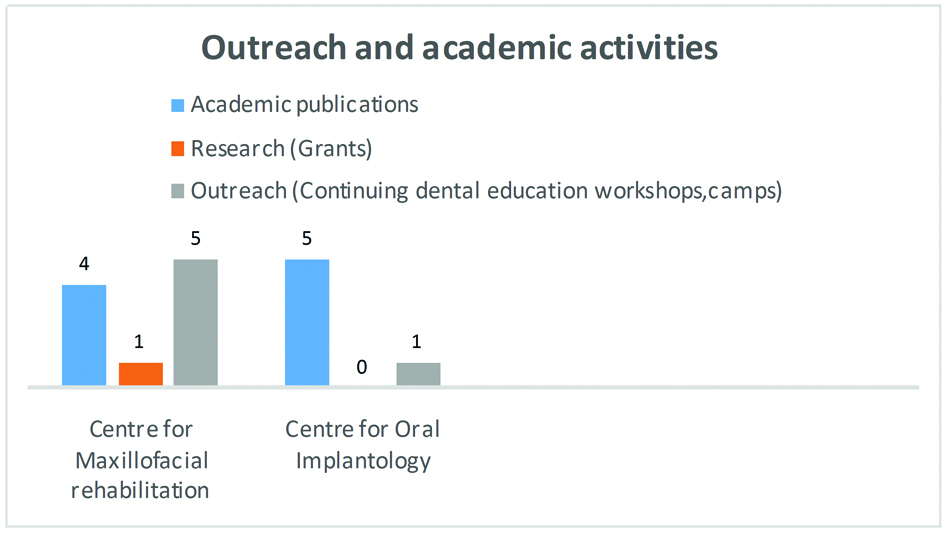
Outreach activities were carried out in the form of continuing dental education workshops, awareness programs and treatment camps. Outreach activities were increased by 40%, coupled with an average increase of patient inflow by 28%. In academic activities, a significant rise in clinical research was found which translated into 12% rise in number of publication by faculty and staff [Table/Fig-3,4 and 5].
Effect of CoE establishment on outreach and academic domain.
Qualitative Data Analysis
The data was obtained with the help of personal interviews and structured validated questionnaires.
When solicited about perceptions, it was commented that, “the program helped for exposure to wide variety of cases and offered a chance for inter-professional collaborations.”
Furthermore, “there was an evolution of better treatment protocols, advantage of learning from renowned faculties of the country and ultimately growth in publications and research”. Students reported enhanced clinical skills due to increased patient exposure and hands-on experience with latest materials. Staff reported some roadblocks faced during this process such as lack of advanced diagnostic facilities in the department had limited some procedures and research activities, time management for faculty and students was difficult [Table/Fig-6].
Qualitative data assessment response.
| S No. | Topic | Question | Answers |
|---|
| 1 | Implementation | Were your program activities put into place as originally intended | It was stated that the program activities were put into place as they were originally intended. |
| 2 | Effectiveness | Is your programme achieving the goals and objectives it was intended to accomplish? | Being the very first year of CoE program, the goals and objectives envisioned were not completely accomplished. |
| 3 | Efficiency | Are your program being produced with appropriate use of resources such as budget and staff time? | The program could efficiently produce resources, funds and faculty development as proposed. |
| 4 | Cost-effectiveness | Does the value or benefit of achieving your program goals and objectives exceed the cost of producing them? | The value of achieving the program goals and objectives did not exceed the cost of producing them. |
| 5 | Attribution | Can progress on goals and objectives be shown to be related to your program, as opposed to other things that are going on at the same time? | Since the progress of the program was monitored periodically, with distinct progress indicators, the growth could be attributed to COE alone. |
The current excellence intervention has indeed laid down a foundation for our institute by virtue of pillars of excellence encompassing the following:
Criteria 1: Academics: Being an academic institution, the implications on teaching-learning were very promising. Undergraduate students were sensitised towards maxillofacial rehabilitation and implant planning at an early stage. Residents were most advantaged to implement enhanced theoretical knowledge in clinical skills.
Criteria 2: Research: There was an enthusiastic response from the students as well as faculty to explore newer avenues for research in these chosen fields. This ultimately led to submission of research proposals for grant procurement, publications and other scholarly activities. Inter-professional training programs were conducted which helped towards better understanding of the subject and ultimately serve the needs of rural population.
Criteria 3: Clinical: Better patient exposure and increase in access to care was observed. Complex clinical cases which were earlier perceived difficult were treated by multispeciality experts with more confidence, leading to better outcomes.
Criteria 4: Faculty development: The faculty were trained through workshops, interdisciplinary programs and focussed discussions during CoE modules. Faculty were self-motivated and showed better confidence in training undergraduates as well as postgraduates for academics and clinical teaching and learning. Faculty engagement was enhanced and better inter-professional rapport and communication was developed.
Criteria 5: Technology: Although the faculty got acquainted with state of the art technological breakthroughs, practical implications were still limited at this stage.
Criteria 6: Social: The rural population was benefitted through this institutional CoE program to a great extent. Furthermore, better access to care was provided and it was depicted through increase in patients reporting to the centre with increased awareness.
Discussion
Healthcare organisations are continuously striving to develop programs focused on quality and the patient experience that will differentiate them in the community. The capacity to grow, change and transform is inherent in the human experience. As a step towards organisational development, the building and promotion of specific Centres of Excellence was taken up at VSPMDCRC.
A Centre of Excellence is an organisation that is viewed as a preferred place of treatment for a specific condition [12]. This preference stems from delivering comprehensive, evidence-based care that is multidisciplinary, and yields exceptional outcomes and high patient satisfaction. Accordingly, a CoE provides more effective and efficient care, and has the evidence to support this claim. The actual role and form of a CoE is largely dependent on the organisational and business context but the essential features include leadership, multidisciplinary team approach, standardised processes and clinical practice, long-term tracking of patient outcomes, and a focus on creating a unique patient experience. Leadership, expertise, and guidance are needed for developing a successful program centered on education, research, and the use of new technology [13]. The present CoE in our institute was focused on comprehensive dental treatment and enhanced quality of care for patients.
Balderston FE et al., discusses dimension of excellence from a management perspective. He claims that the extent to which the institution satisfies some conditions for long-term viability is of central importance, where the most important components are a sound governance structure ensuring autonomy and self-direction, and a broadly accepted commitment to academic values [14]. Hemlin S et al., suggested that management with harmonised intents, excellent concepts and group participation with well-managed staff selection are crucial to outstanding research settings [15]. As with Balderston, the correct background with major focus on genuine research stimulates superior output. The present CoE model was semi-autonomous, with decentralisation of powers to a large extent and governance from the management. The stakeholders controlled the decision making process under the leadership of higher authorities.
Any program evaluation needs to be practical and feasible and conducted within the confines of resources, time, and political context. Evaluation findings helped to make decisions about program implementation and to improve program effectiveness [16]. The evaluation framework used in the present study was based on public health program evaluation criteria’s and it was substantiated into qualitative and quantitative data based on logic model. It included assessing and documenting program implementation, outcomes, efficiency and cost-effectiveness of activities. This evaluation was conducted according to a set of guidelines and was influenced by real-world constraints.
In one of the first evaluations of such a program in India, we found that CoE development greatly influenced clinical expertise, academic training and innovations in oral healthcare through research, blended with technological advances. In addition, faculty development and social responsibility was enhanced, ultimately leading to provision of dental and public health practices of the highest standard.
Organisational researchers have long sought to establish the impact of organisational structures and managerial processes on outcomes such as profitability, effectiveness, performance, and organisational growth and survival [17]. The present CoE intervention impacted these managerial processes in our institute to a great extent, particularly faculty and student performance and patient care. However, the institute being in a rural setup, profitability was not a major focus of the intervention. As a preliminary report, impact on organisational survival was not assessed in the present study.
Clinical governance, better human resource management practices, quality patient care are important planks for organisational development. All these demand attention, not just to the individual level of analysis, but to the ways that clinical directorates, divisions, trust boards, and professionals work together to achieve quality [17]. These goals move organisational research onto the centre stage. In this regard, CoE development and execution was taken up as a novel initiative in rural settings. The development of focused CoE’s at institutional level would greatly impact the organisational development, patient care and overall growth. The key success factors include the planned development and execution of the program and timely evaluation with proper management of human resources. Indeed, not all changes are improvements but all improvement involves change.
Limitation
As it was a preliminary report, long-term evaluation of the CoE program was not carried out. Also, the constituent members feedback regarding practical difficulties, analysis of functioning of CoE, its utility for patient care services needs to be assessed for long-term period.
Such CoE modules would serve as an example for other institutes across the country and aid in faculty and student development as well as to provide efficient patient care services to the community.
Conclusion
The preliminary evaluation of the current CoE program showed potential for the institutional growth in all aspects, reflected in the form of advancements in the six pillars of excellence. Although there are many impediments ahead, the stakeholders benefitted from starting the CoE program to a large extent. It also helped in fostering teamwork and collaboration, improving patient outlook towards the institution and generating better training opportunities for students. Nonetheless, certain key policy changes for much better growth are anticipated.