Left-Sided Vanishing Lung Tumour: A Rare Case
Karanam Gowrinath1, Chinnangari Vijay Amaranatha Reddy2
1 Senior Consultant, Pulmonary Medicine, Apollo Speciality Hospital, Nellore, Andhra Pradesh, India.
2 Consultant Cardiology, Apollo Speciality Hospital, Nellore, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Karanam Gowrinath, Senior Consultant, Department of Pulmonary Medicine, Apollo Speciality Hospital, Pinakininagar, Muthukur Road, Nellore-524004, Andhra Pradesh, India.
E-mail: drkgowrinath@gmail.com
In some cases of congestive heart failure, interlobar transudative pleural effusions may occur and appear like a tumour in the chest radiograph and disappear with diuretic therapy. They are called as Vanishing or Phantom or Pseudotumours and detected most often in the right lung. Left-sided vanishing lung tumour is very rare and we are not aware of similar previous case report in English literature. We report a left-sided vanishing lung tumour as a manifestation of cardiac failure in an elderly man who presented with intermittent swelling of feet during follow-up after coronary bypass surgery. Addition of oral diuretic (furosemide) led to rapid symptomatic relief and complete resolution of interlobar effusion in the left oblique fissure within two months. The follow-up computed tomography of chest showed left-sided small residual pleural thickening near left oblique fissure as possible cause of unusual site of vanishing tumour in our case.
Congestive heart failure, Interlobar pleural effusion, Phantom tumour, Pseudotumour, Vanishing tumour
Case Report
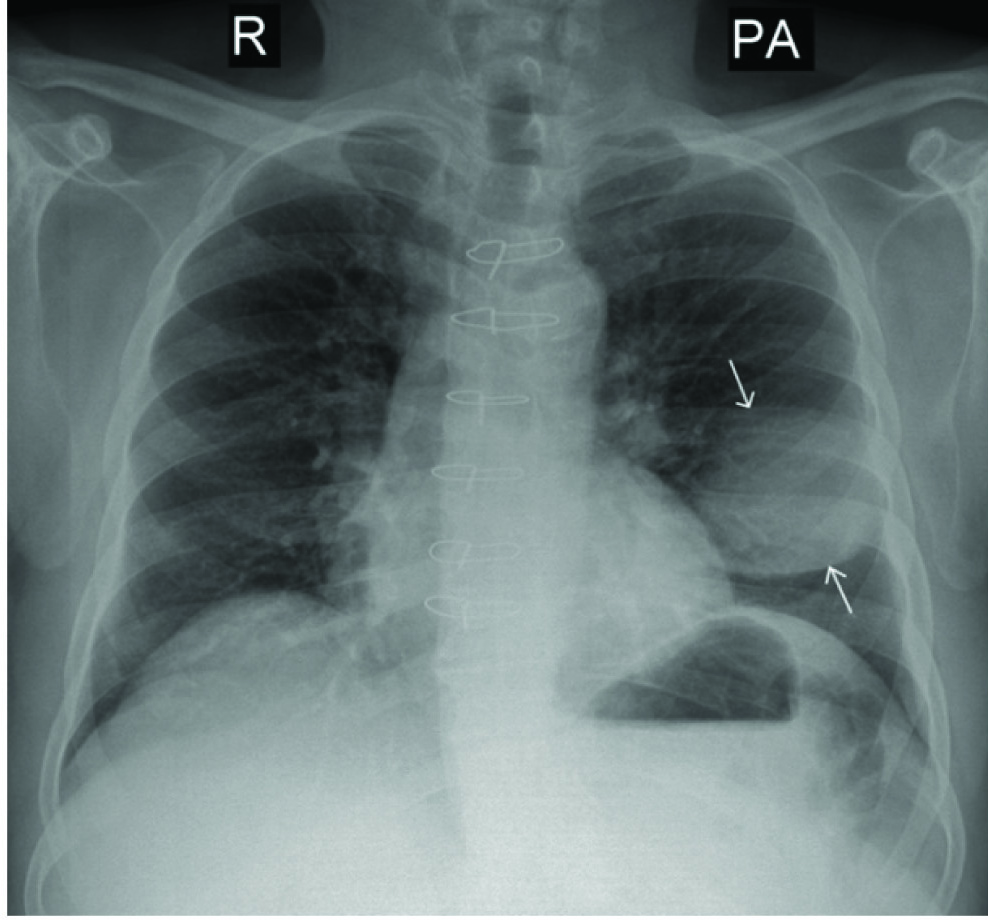
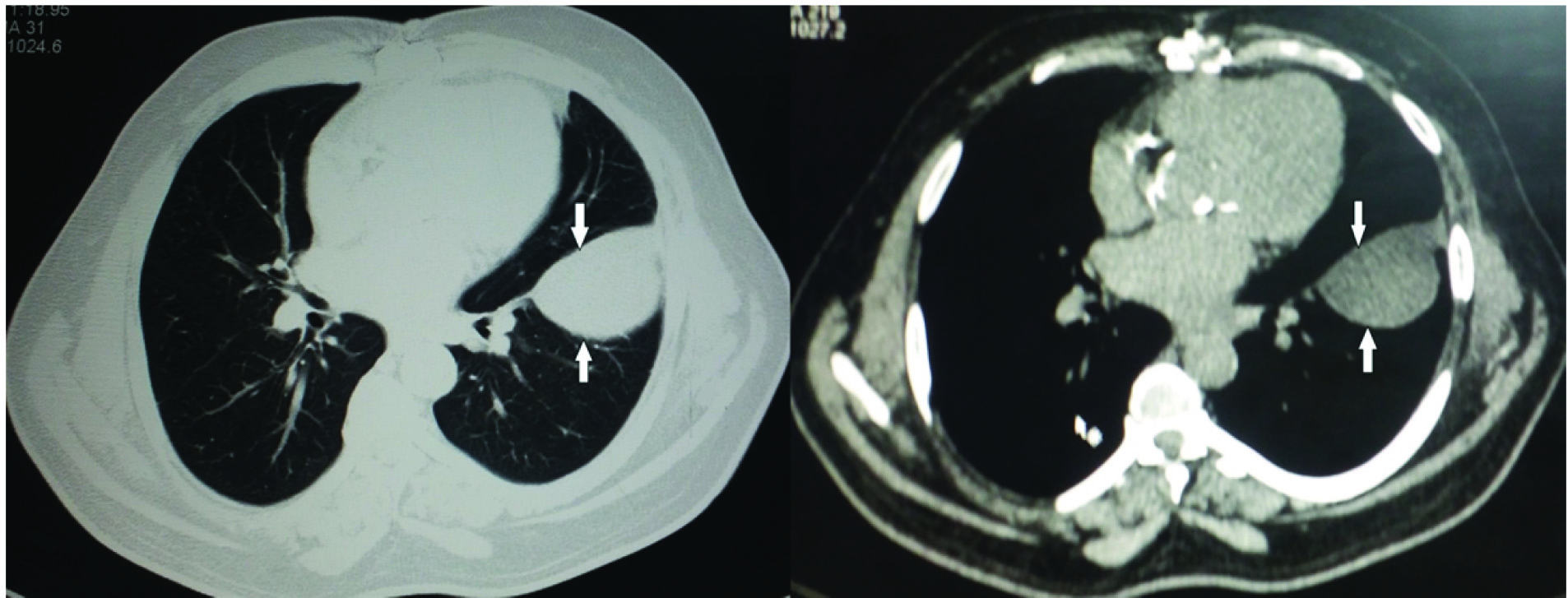
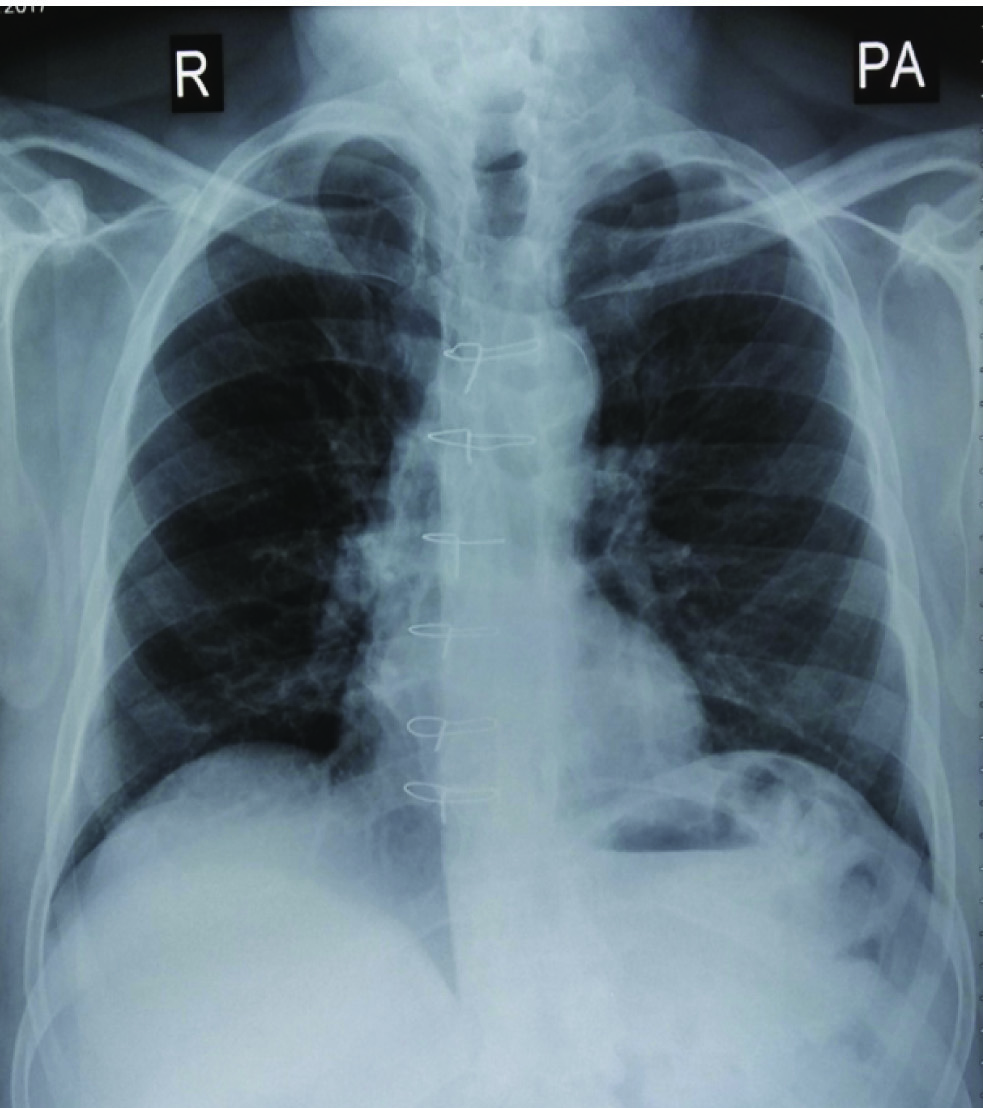
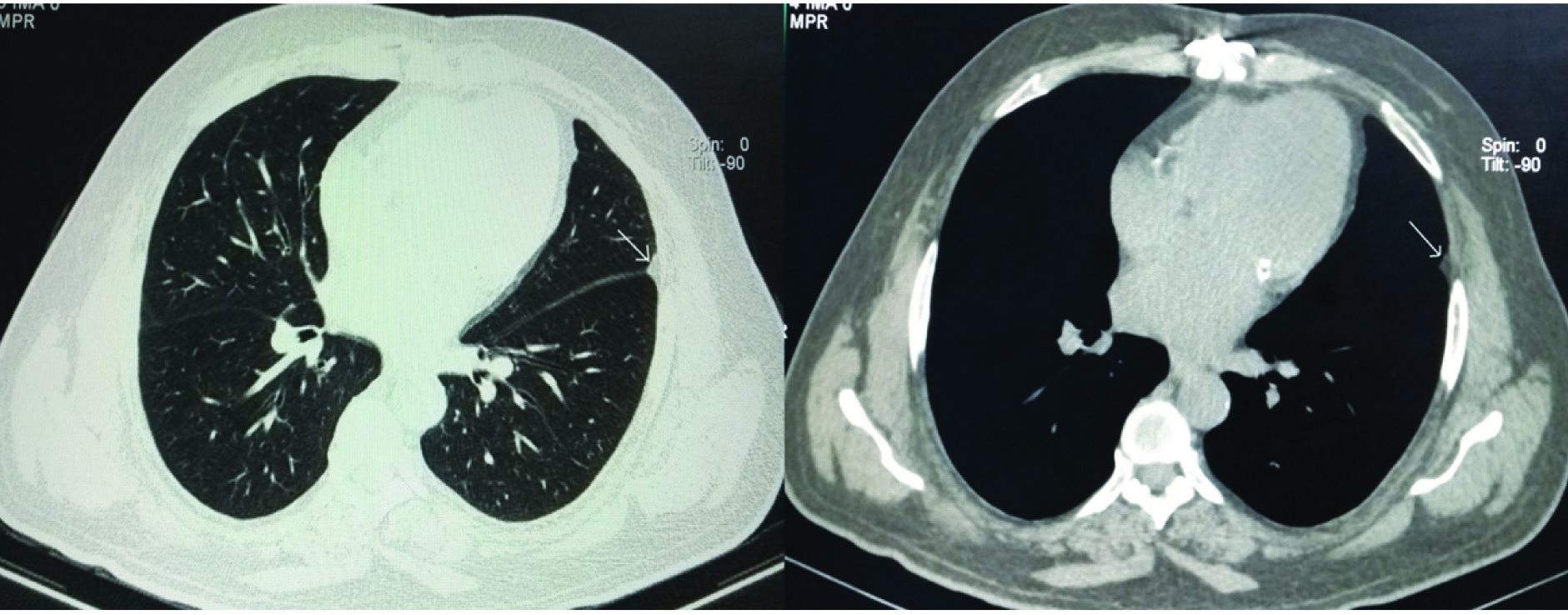
A 68-year-old male ex-smoker was referred to our outpatient department for opinion regarding abnormal chest radiograph. Patient had 7 month history of on and off swelling of feet. There was no significant cough or limitation of routine daily activities. Patient underwent coronary artery bypass surgery for triple coronary vessel block two years back. He was treated for left-sided tuberculous pleurisy with effusion in 1997. Patient has been under treatment for diabetes mellitus and hypertension for the past 20 years. Physical examination revealed obesity, normal jugular venous pressure, bilateral 2+ pitting pedal oedema and blood pressure of 140/90 mmHg. Clinical examination of cardiovascular system and other systems was not particularly significant. A postero-anterior chest radiograph [Table/Fig-1] showed a round opacity (White arrows) in the left para-cardiac region. A CT scan of chest [Table/Fig-2] showed well-defined elliptical shaped pleural fluid collection in the left oblique fissure with attenuation of zero Hounsfield units. Trans-thoracic echocardiogram demonstrated good biventricular function with moderate mitral regurgitation. Oral diuretic (furosemide) was added to the existing drug therapy of the patient and swelling of feet subsided within a week. Patient returned to us after two months and follow-up chest radiograph [Table/Fig-3] was normal and chest CT [Table/Fig-4] was also normal except for localized pleural thickening (Thin white arrow) near the edge of left oblique fissure which might have caused left-sided vanishing lung tumour in our case.
Postero-anterior chest radiograph showing round opacity (White arrows) in the left para-cardiac region
CT of chest showing elliptical shaped localized collection of fluid in the left oblique fissure
Follow-up chest radiograph (Postero-anterior view) showing resolution of left interlobar effusion.
Follow-up chest CT showing localized residual pleural thickening (Thin white arrow) in left haemothorax.
Discussion
In some cases of Congestive Heart Failure (CHF), transient localization of pleural fluid may occur within pulmonary fissures and appear like a tumour in the chest radiograph and disappear with diuretic treatment. They are called as vanishing or phantom or pseudotumours. Vanishing lung tumour is often an incidental finding in the chest radiograph and most cases are associated with CHF or any other disease causing transudative pleural effusion [1]. Vanishing lung tumours (Single or multiple) most often occur in the transverse fissure followed by oblique fissure of the right lung but left lung is rarely involved [2]. In CHF, most vanishing tumours occur in the right lung because of higher hydrostatic pressure and also due to higher venous pressure along with impaired lymphatic drainage as a result of frequent right recumbent posture preferred by many cardiac failure patients [3]. Another mechanism of localization of pleural effusion in CHF may be due to local increase in elastic recoil by adjacent partially collapsed lung as a result of suction cup effect [4]. An elliptical opacity of localized pleural fluid collection along the long axis of a pulmonary fissure can usually be diagnosed through chest radiograph but CT confirms loculated fluid collection within a major or minor fissure [5]. In our case, CT of chest revealed the site, shape and the transudative nature of the pleural fluid. Vanishing lung tumour can develop irrespective of the cause and severity of CHF and its different shapes like round, oval, spindle, wedge or linear shadows in the chest radiograph indicate the volume and position of fluid, the angle of projection of X-ray beam, patient’s position and the degree of compression of surrounding lung parenchyma [6]. In our case, the transudative effusion localized in left oblique fissure appeared as round opacity in the postero-anterior chest radiograph and elliptical in the CT scan of chest. Localization of pleural effusion can occur anywhere in the lung whenever adhesions develop between contiguous surfaces of parietal and visceral pleura including interlobar fissures as a result of intense pleural inflammation in conditions like empyema, haemothorax or tuberculous pleuritis [7]. In CHF, transudation from the pulmonary vascular space exceeds resorption ability of the pleural lymphatics resulting in accumulation of pleural fluid in pulmonary fissure/s but adhesion and obliteration of pleural space around the edge of the fissure may prevent its free spread. Many patients who present with vanishing lung tumour fail to give history of pleuritis. In a retrospective study, all 12 cases of vanishing lung tumours in CHF were right-sided and it was postulated that vanishing lung tumours at unusual sites may occur in regions where tuberculosis is common and penetrating chest injuries like stab injuries are frequent [8]. Vanishing lung tumour can occur many years after infection or injury with pleural involvement. Our case had history of left-sided tuberculous pleuritis and developed left-sided vanishing tumour as a feature of CHF twenty years later. Vanishing lung tumour has been reported as a manifestation of CHF in the middle age where pneumonia with pleural involvement occurred in childhood [9]. An isolated case of left-sided multiple vanishing lung tumours as a manifestation of CHF was reported in a patient following gunshot injury to left and haemothorax 20 years back [10]. Vanishing lung tumour due to adhesive pleurisy tends to recur in the same area whenever CHF returns [11]. In our case, the unusual location of vanishing lung tumour prompted us to order chest CT which established the cause and transudative nature of pleural fluid simultaneously showing the normal lung parenchyma and mediastinum. We are not sure about the timing of disappearance of vanishing lung tumour as patient came for review after two months only. We are not aware of any similar previous report of left-sided vanishing lung tumour in the English literature. Once diagnosed, vanishing lung tumour does not have any separate treatment other than that of underlying cause like CHF.
Conclusion
Left oblique fissure is an unusual site of vanishing lung tumour which may occur even if CHF is mild. Chest CT can detect vanishing lung tumour as well as its predisposing factor/s and helps to rule out other causes of radiographic opacity.
[1]. Haus BM, Stark P, Shofer SL, Kuschner WG, Massive pulmonary pseudotumorChest 2003 124(2):758-60.10.1378/chest.124.2.75812907571 [Google Scholar] [CrossRef] [PubMed]
[2]. Gefter WI, Boucot KR, Marshall EW, Localized interlobar effusions in congestive heart failure: vanishing tumour of lungCirculation 1950 2(3):336-43.10.1161/01.CIR.2.3.33615434934 [Google Scholar] [CrossRef] [PubMed]
[3]. Rabinowitz JG, Kongtawng T, Loculated interlobar air fluid collections in congestive heart failureChest 1978 74(6):681-83.10.1378/chest.74.6.681153830 [Google Scholar] [CrossRef] [PubMed]
[4]. Stark P, Leung A, Effects of lobar atelectasis on the distribution of pleural effusion and pneumothoraxJ Thorac Imaging 1996 11(2):145-49.10.1097/00005382-199621000-000048820023 [Google Scholar] [CrossRef] [PubMed]
[5]. Lemos J, Klein JS, Methods of examination, Normal anatomy and Radiographic findings of Chest disease. In Brant WE, Helms CA, editorsFundamentals of Diagnostic Radiology 2012 4th edPhiladelphiaWolter Kluwer/Lippincott Williams & Wilkins:324-66. [Google Scholar]
[6]. Willerson JT, Fred HL, Eiband JM, Collins LC, Felson B, Spitz H, Roentgenogram of the monthDis of Chest 1965 48:85-86.10.1016/S0096-0217(15)30351-4 [Google Scholar] [CrossRef]
[7]. Light RW, Pleural diseases 2007 5th edPhiladelphia, PAWalters Kluwer/Lippincott Williams & wilkins [Google Scholar]
[8]. Van Gelderen WFC, Vanishing pleural fluid collections in cardiac failure simulating lung tumoursJournal of Medical Imaging and Radiation Oncology 1994 38(2):93-96.10.1111/j.1440-1673.1994.tb00143.x8024517 [Google Scholar] [CrossRef] [PubMed]
[9]. Baks T, Kock MC, Kofflard MJM, Computed tomography unmasks a phantom tumourInt J Cardiol 2011 149(1):e38-39.10.1016/j.ijcard.2009.03.09219380168 [Google Scholar] [CrossRef] [PubMed]
[10]. Buck KP, Morehead RS, Multiple left-sided vanishing tumorsChest 2000 118:1486-89.10.1378/chest.118.5.148611083706 [Google Scholar] [CrossRef] [PubMed]
[11]. Lozo M, Vukovac EL, Ivancevic Z, Platikosic I, Phantom tumour of the lungs: Localized interlobar effusion in congestive heart failureCase Rep Cardiol 2014 2014:20729410.1155/2014/20729425328714 [Google Scholar] [CrossRef] [PubMed]