The Window Approach for Extraction of Tooth Root Fragments: A Different Soft Tissue Management
Roberto Pippi1, Rita Colaci2, Alessandra Pietrantoni3
1 Associate Professor, Department of Oral and Maxillo Facial Sciences, Sapienza, University of Rome, Rome, Italy.
2 Resident, Department of Oral and Maxillo Facial Sciences, Sapienza, University of Rome, Rome, Italy.
3 Resident, Department of Oral and Maxillo Facial Sciences, Sapienza, University of Rome, Rome, Italy.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Roberto Pippi, Via Caserta 6, Rome, Italy.
E-mail: roberto.pippi@uniroma1.it
Different techniques have been proposed for the removal of the apical portion of fractured teeth. The window approach was proposed in the past to remove a tooth root fragment through a buccal bone opening at the level of fragment. In the classical approach, a marginal triangular flap is elevated, only the bone overlying the fractured apex is removed and then the apex is pushed out by an elevator toward the alveolar crest. In this technique, the bone removal is minimal, and it does not involve the marginal bone so that patient’s post-surgical discomfort is reduced, and bone resorption is less. A different kind of soft tissue management for bone exposure is proposed here with a simple linear incision at the level of the root apex without any vertical incision. This kind of incision is simple and versatile, leads to a lesser discomfort to the patient and avoids un-aesthetic scar.
Elevator, Incision, Tooth fracture
Case Report
The case presented here concerns the surgical extraction of the apical portion of the left maxillary canine root in a 45-year-old male patient in good general health condition, after the coronal portion of the tooth was fractured during luxation due to the presence of a wide external root resorption, possibly inflammatory in nature, which made extraction necessary [Table/Fig-1].

Using the already extracted part of the tooth as reference height, a 1 cm full-thickness linear incision was performed on the buccal gingiva at the root apex level, parallel to the marginal bone [Table/Fig-2], without any further anaesthesia, in addition to the 3%-carbocaine periapical anesthesia performed before tooth extraction procedure started.
Surgical view: soft tissue incision.

The soft tissue flap above the incision margin was then elevated with a Prichard periosteal elevator to expose the area overlying the apex of the root fragment which had to be extracted.
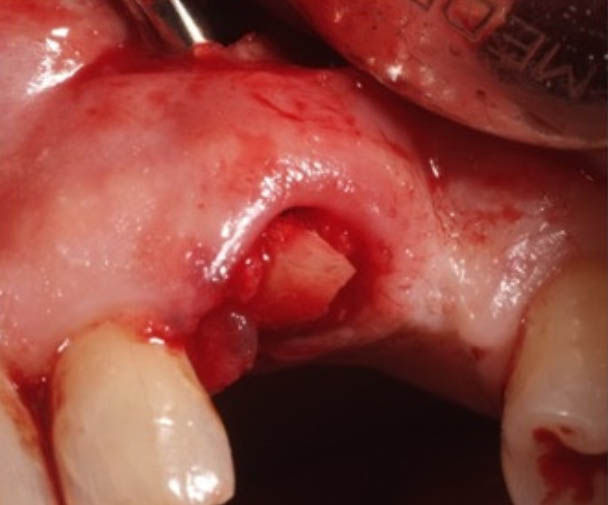
A 2.1 mm multi-blade round steel bur (ISO: 310.205.001291.021) was used to uncover the root tip and to remove the bone overlying the apical portion of the fractured fragment to allow sufficient access for inserting an elevator. A small curved elevator was then used to displace the root tip out of its socket through the alveolar cavity [Table/Fig-3]. At this point, all tooth fragments were extracted [Table/Fig-4].
Surgical view: the apical portion of the tooth was displaced out of its socket.
All post-extraction tooth fragments. Apical portion is that in the middle.

Finally, the bone window margins were rounded with a 3.3 mm multi-blade steel bur (ISO: 310.205.001291.033), the residual cavity was revised and irrigated with saline solution and the soft tissues were sutured using a 4-0 synthetic absorbable suture (Vicryl®) [Table/Fig-5], without any surgical packing.
Surgical view: the sutured wound.

The postoperative course was uneventful with no pain, haemorrhage or discomfort. Suture were removed after five days [Table/Fig-6].
Wound healing, after suture removal.

Since no symptoms were present, the patient decided not to undergo further check-up visits or radiographs.
Discussion
Different techniques have been proposed for the removal of the apical portion of the fractured teeth [1-6]. A close technique has been suggested to be preferable rather than the open one [1], since the latter results in more extensive bone resorption while the removal of a root tip with a non-surgical procedure results in a better residual ridge [7] to support restorative appliances.
The open technique involves the elevation of a buccal flap, the exposure of the root fragment by buccal cortical bone removal, luxation and extraction of the fragment through the bone opening or its displacement out of the socket with a small elevator [6]. Many authors proposed alternative techniques with the aim to preserve the bucco-crestal bone which is important if the extracted tooth has to be replaced with either a traditional prosthesis or an implant-supported prosthesis [1-5].
In the close technique, no flap is elevated, the bone is not removed, and root extraction is performed through the alveolar cavity with different instruments. Tip elevators are used in the traditional approach [6], however several other instruments have been suggested alternatively, such as an Hedstrom file [1,2], a hypodermic needle [3], a large surgical bur [4] or an expandable micro-motor bur [5].
The window technique is a valid alternative to the classical surgical technique which requires the buccal bone removal for inserting the elevator tip. In the window technique the bone removal is minimal, and it does not involve the marginal bone so that patient’s post-surgical discomfort is reduced, and bone resorption is lesser. This approach is simple and versatile since it can also be used in difficult situations such as in the case of curved apices and hypercementosis. Finally, it allows to remove small apical fragments directly through the bone windows, not only in the case of a newly fractured apex but also in the case of retained root fragments.
A different kind of soft tissue management was presented here, with a small linear incision at the level of the tooth apex, without any vertical incisions differing from the classical window technique triangular flap. This kind of incision leads to a lesser discomfort for the patients and avoids un-aesthetic scars since no vertical incisions are involved. The proposed surgical approach is a valid alternative for tooth root fragment extraction when the closed techniques have not been successful, or it could not be used due to maxillary sinus proximity, to avoid root fragment displacement into that space.
Actually, it is a less invasive procedure which allows the surgeon to obtain a direct visual access to the apical fragment that can be easily removed without extensive bone loss.
Conclusion
The window approach with bone exposure by a simple linear incision of the overlying soft tissues is a good alternative for the quicker removal of a fractured root apex and for the better wound healing as compared to the traditional technique.
[1]. Kannan VS, Narayanan GR, Ahamed AS, Velavan K, Elavarasi E, Danavel C, A new atraumatic method of removing fractured palatal root using endodontic H-files luted with resin modified glass ionomer cement: A pilot studyJ Pharm Bioallied Sci 2014 6(Suppl 1):S156-59.10.4103/0975-7406.13743125210360 [Google Scholar] [CrossRef] [PubMed]
[2]. Cerny R, Removing broken roots - a simple methodAust Dent J 1978 23(4):351-52.10.1111/j.1834-7819.1978.tb03536.x282839 [Google Scholar] [CrossRef] [PubMed]
[3]. Uppal N, Dental root fragment extraction using a hypodermic needleTrop Doct 2008 38(1):1610.1258/td.2007.06017218302854 [Google Scholar] [CrossRef] [PubMed]
[4]. Uppal N, Hong LW, Quasi-surgical technique for easy removal of broken tooth rootsTrop Doct 2013 43(4):136-37.10.1177/004947551350508924056669 [Google Scholar] [CrossRef] [PubMed]
[5]. Bonjar AHS, Expandable Micro-motor Bur, design of a new device for least invasive extraction of broken teeth rootsAnn Surg Innov Res 2013 7(1):0210.1186/1750-1164-7-223497515 [Google Scholar] [CrossRef] [PubMed]
[6]. Peterson LJ, Principles of complicated exodontia. In: Peterson LJ, Ellis E, Hupp JR, Tucker MR, editorsContemporary oral and maxillofacial surgery 2003 4th edSt. LouisMosby:179-80. [Google Scholar]
[7]. Costich ER, Ramfjord SP, Healing after partial denudation of the alveolar processJ Periodontol 1968 39(3):127-34.10.1902/jop.1968.39.3.1275240004 [Google Scholar] [CrossRef] [PubMed]