Kienböck’s Disease Hidden behind the Ganglion Cyst: A Clinical Clue
Denız Aydin1, Bariş Polat2
1 Department of Orthopaedics and Traumatology, Near East University, Faculty of Medicine, Nicosia, Cyprus.
2 Department of Orthopaedics and Traumatology, Near East University, Faculty of Medicine, Nicosia, Cyprus.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bariş Polat, Near East University, Near East Boulevard Nicosia/TRNC Mersin 10, ZIP-99138, Nicosia, Cyprus.
E-mail: drbpolat@hotmail.comdrbindiya@yahoo.co.in
Ganglion cyst is the most common soft tissue mass of the wrist. Diagnosis is made by physical examination. Ultrasonography is used for diagnosis of occult ganglions. Cosmetic appearence and annoying pain are the most common complains of the patient with a wrist ganglion. It is a benign lesion and most of the time it regresses spontaneously or is treated with simple strategies. On the other hand, dorsal wrist ganglions could be misleading in diagnosis of underlying more serious pathologies. Traumatic bone or ligament injuries, benign bone tumours, inflammatory arthropathies, ulnar impaction syndrome, Kienböck’s disease and many other pathologies may have the similar symptoms with the wrist ganglion. Physicians should be suspicious in case of debilitating progressive symptoms. Ultrasonography is not diagnostic for most of the possible underlying diseases so further evaluation should be done with radiography and Magnetic Resonance Imaging (MRI). We report a case of 21-year-old man with severe right wrist pain and dorsal wrist ganglion, diagnosed with Kienböck’s disease seven months after the beginning of symptoms.
Avascular necrosis, Delayed diagnosis, Lunate pathology, Wrist pathology
Case Report
A 21-year-old man presented with severe wrist pain and swelling on the dorsal side of the right wrist since seven months. Previously, he was evaluated in another hospital with wrist radiographs and ultrasonography. He has been told that there was no osseous pathology and there was a 2×2 cm dorsal ganglion cyst. He was treated with wrist orthosis limiting wrist range of motion and NSAI drugs. He said that as far as he was taking painkillers and using the wrist orthosis his pain was mild but with time he became unable to do wrist motions cause of extreme pain.
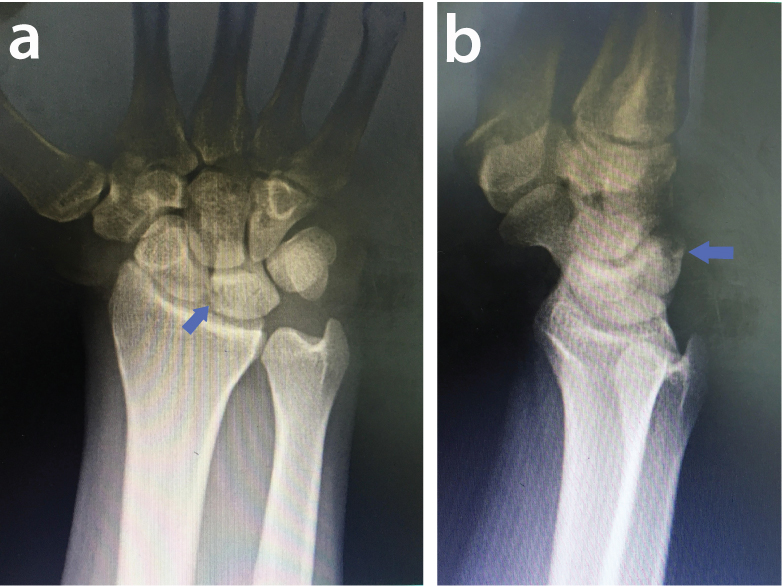
His physical examination showed a soft and mobile swelling with fluctuation over the dorsal side of the right wrist which look like dorsal ganglion cyst. There was mild to moderate tenderness around the dorsal wrist mass. Active wrist dorsiflexion was 30 degrees, volar flexion was 40 degrees and passive motion above these ranges were extremely painfull on the right side. There was fragmentation on the dorsal side of the lunate in his lateral X-ray [Table/Fig-1a,b]. His MRI evaluation showed panlunate increased signal intensity on proton density fat saturated images and 11×4×7 mm ganglion cyst on the dorsal side of the lunate bone [Table/Fig-2]. The patient was diagnosed with Kienböck’s disease and associated ganglion cyst. He refused surgical treatment and did not attend follow-up clinic. The patient was informed that his radiographs and case details would be submitted for publication and he gave his consent.
Anteroposterior (a) and lateral (b) wrist radiographs. Fragmentation on the dorsal side of the lunate bone is seen on the lateral X-ray.
Proton density fat saturated image of the wrist. Increased panlunate signal intensity and associated darsal ganglion cyst is observed.

Discussion
Ganglion cyst is the most common soft tissue mass around the wrist [1]. An obvious dorsal wrist ganglion cyst could be misleading for the physician in case of an associated less frequent devastating condition like Kienböck’s disease.
Ganglion cysts are benign lesions [2]. Aetiology is unclear but sometimes patients give a history of acute or repetitive trauma. Patients in all age groups may be affected; however, most commonly seen in ages 20-40 [1]. Swelling and tenderness over the dorsal wrist, limitation in range of motion and decreased grip strength can be foundon physical examination. The symptoms are more likely to be annoying than debilitating. Physical examination is adequate for the diagnosis in most of the cases. Ultrasonography and MRI is used in the diagnosis ofoccult ganglions [3]. In case of dorsal wrist pain with a suspected occult dorsal wrist ganglion, it is advised to use ultrasonography instead of MRI cause of its significant cost effectiveness. Wong SA et al., reported that routine wrist radiography is not useful for the evaluation of wrist ganglions [4]. However, radiographic evaluation should be used for diagnosing any suspected osseous pathology.
Kienböck’s disease aetiology is also unclear and it is most common in ages 20-40. Dorsal wrist tenderness, decreased range of motion and loss in grip strength are the physical examination findings [5]. The symptoms are progressive and more debilitating than dorsal wrist ganglions. In progressed stage of Kienböck’s disease, radiographic evaluation is diagnostic; but radiographic findings are mild or absent in early stages of the disease [5]. MRI is useful in diagnosis of Kienböck’s disease in case of negative radiologic findings. Radiographs and MRI are necessary for the staging of the disease. Lichtman classification is the most commonly used staging scheme [5]. The treatment options are guided by the Lichtman stage and radiologic measurements. Kienböck’s disease is a progressive disease. Carpal collapse and wrist arthrosis is the end stage of the disease with significant morbidity [5].
Patient’s history and clinical findings in early stage of Kienböck’s disease are similar with dorsal wrist ganglion. If the physician focus on the ganglion cyst, misdiagnosis of the other underlying more serious injuries is possible. Bone bruise or occult fracture of wrist bones, scapholunate and other wrist ligaments injuries, triangular fibrocartilage complex tear, ulnar impaction syndrome, intraosseous ganglion, benign bone tumours (aneurysmal bone cyst, osteoid osteoma, enchondroma, giant cell tumour), inflammatory arthropathies (chronic gout) and carpal amyloidosis may have the similar symptoms with the ganglion cysts [6]. A detailed anamnesis, careful physical examination and also adequate radiologic evaluation are important to prevent misdiagnosis and delayed diagnosis of these diseases. Although, the cost effectiveness of routine wrist radiography is questioned in the literature, in case of debilitating symptoms routine X-rays should be obtained and evaluated carefully [4]. In case of occult lesion with dorsal wrist pain, if occult dorsal wrist ganglion is suspected, ultrasonography is preferred for diagnosis cause of its cost effectiveness. However, ultrasonographic evaluation is not diagnostic in most of the possible underlying serious injuries. MRI is a precious non invasive diagnostic tool for evaluating occult wrist lesions. It is able to detect both bony and soft tissue pathologies, also it is sensitive and specific for occult carpal bone lesions [7]. Senevirathna S et al., reported delayed MRI findings of 110 patients after acute wrist injuries with persisting pain and normal radiographs. MRI revealed 25.4% normal result, 21.8% occult bone fracture, 10.9% bone bruise, 4.5% triangular fibrocartilage complex tear, 12.7% ganglion cyst and 2.7% Kienböck’s disease in their study [7]. It is concluded that MRI is a useful tool for definitive diagnosis of persistent wrist symptoms [7]. There are several important lunate pathologies that may cause abnormal lunate signal on MRI [8]. The most frequent causes are Kienböck’s disease (25%), and the others; ulnar impaction syndrome (25%), intraosseous ganglion (20%), lunate fracture, degenerative diseases and inflammatory diseases [8]. MRI are sufficient for diagnosis when evaluated by the patient’s symptoms and examination.
Conclusion
Dorsal wrist ganglions with debilitating persistent pain should be suspected for underlying more serious lesions and further evaluation with radiographs and MRI is necessary for definitive diagnosis.
[1]. Minotti P, Taras JS, Ganglion cysts of the wristJ Hand Surg 2002 2(2):102-07.10.1053/jssh.2002.33318 [Google Scholar] [CrossRef]
[2]. Mathoulin C, Gras M, Arthroscopic management of dorsal and volar wrist ganglionHand Clin 2017 33(4):769-77.10.1016/j.hcl.2017.07.01228991587 [Google Scholar] [CrossRef] [PubMed]
[3]. Osterwalder JJ, Widrig R, Stober R, Gachter A, Diagnostic validity of ultrasound in patients with persistent wrist pain and suspected occult ganglionJ HandSurg 1997 22(6):1034-40.10.1016/S0363-5023(97)80044-5 [Google Scholar] [CrossRef]
[4]. Wong SA, Jebson PJL, Murray PM, Trigg SD, The use of routine wrist radiography is not useful in the evaluation of patients with a ganglion cyst of the wristHand 2007 2(3):117-19.10.1007/s11552-007-9032-818780070 [Google Scholar] [CrossRef] [PubMed]
[5]. Lutsky K, Beredjiklian PK, Kienböck diseaseJ Hand Surg 2012 37(9):1942-52.10.1016/j.jhsa.2012.06.02922916868 [Google Scholar] [CrossRef] [PubMed]
[6]. Paparo F, Fabbro E, Picazzo R, Revelli M, Ferrero G, Muda A, Multimodality imaging of intraosseous ganglia of the wrist and their differential diagnosisRadiol Med 2012 117(8):1355-73.10.1007/s11547-012-0875-x22986695 [Google Scholar] [CrossRef] [PubMed]
[7]. Senevirathna S, Rajeev A, Newby M, The value of delayed MRI scans in the assesment of acute wrist injuriesActa Orthop Belg 2013 79(3):275-79. [Google Scholar]
[8]. Schmitt R, Christopoulos G, Kalb K, Coblenz G, Fröhner S, Brunner H, Differential diagnosis of the signal-compromised lunate in MRIRofo 2005 177:358-66.10.1055/s-2004-81393115719297 [Google Scholar] [CrossRef] [PubMed]