Case Report
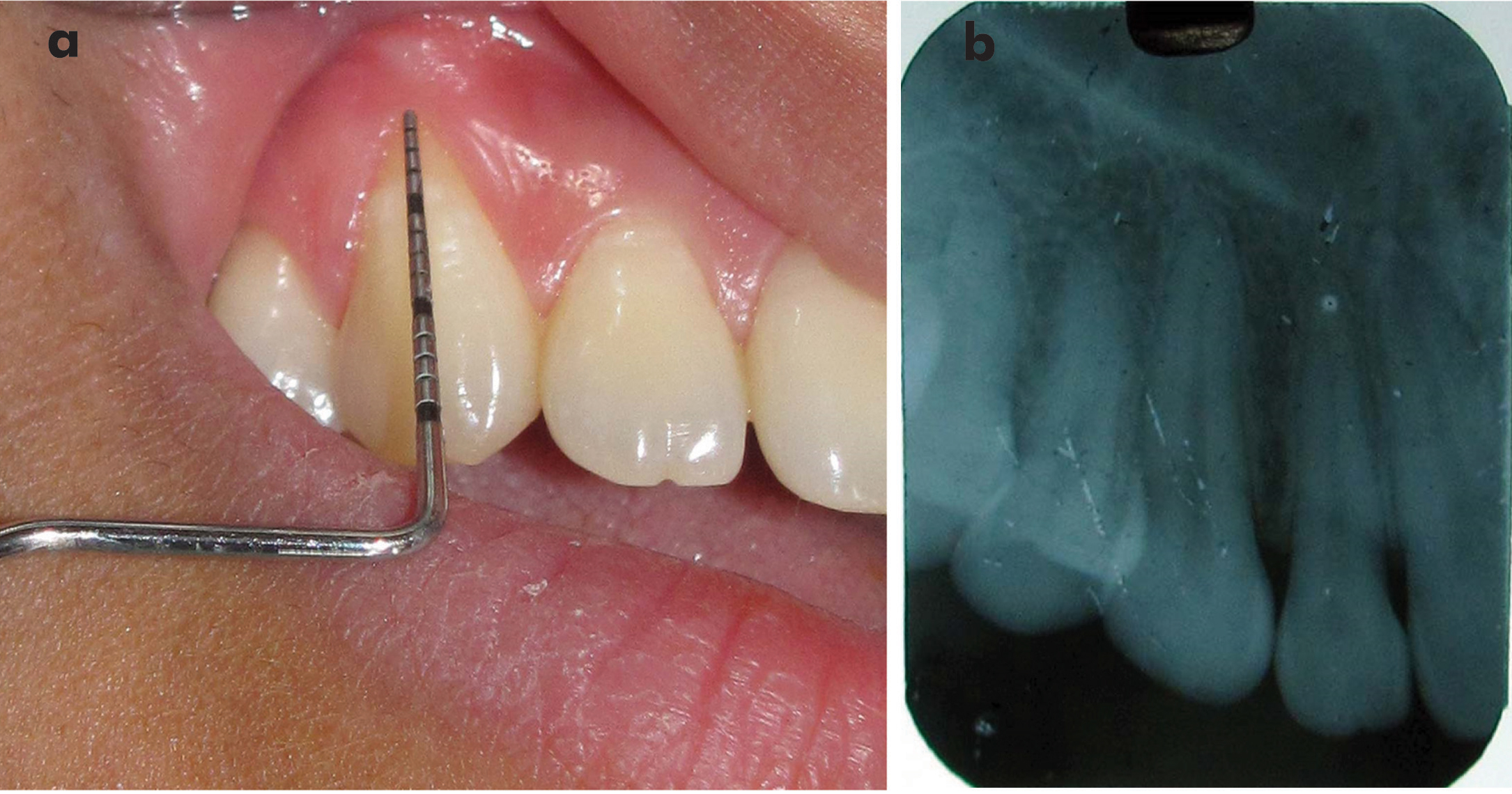
A 22-year-old young female patient had chief complain of receding gum in upper front tooth region. On intra-oral examination, visible gingival recession of Miller class I at labial surface of the upper right canine (#13) [1] was present due to toothbrush trauma. The visible gingival recession depth was 3.5 mm recorded by using UNC-15 periodontal probe-measured from Cemento Enamel Junction (CEJ) of labial surface to the margin of free gingiva [Table/Fig-1a]. Gingival height was 4.0 mm when measured from the apical most margin of free gingiva to the mucogingival junction. Probing depth was 2.0 mm as when measured from the margin of free gingiva to bottom of the gingival sulcus. Radiographically, no signs of interproximal bone loss were evident and no other pathology was detected [Table/Fig-1b].
a) Pretreatment clinical situation showing visible gingival recession on #13; b) IOPA radiograph of #13 showing no interproximal bone loss.
Phase I periodontal therapy was completed which consist of scaling, root planing and oral hygiene instructions. Patient was advised rolling stroke technique for toothbrushing with visible gingival recession to stimulate gingival augmentation and to reduce injury of gingival margin. Surgery for treatment of visible gingival recession was planned after three weeks of phase I therapy despite the patient had clinically normal probing depth because this period is considered adequate for resolution of gingival inflammation. Presence of gingival inflammation can alter the measurements and ultimately the treatment outcome also.
At the time of surgery, informed written consent was taken from the patient. This case report was approved by the institutional ethical committee for human subjects and was also conducted in accordance with the Helsinki Declaration of 1975, as revised in 2000. Patient was instructed to do presurgical rinse by 0.2% chlorhexidine gluconate solution for one minute. The perioral area was cleaned with spirit and scrubbed by 5% aqueous solution of povidone iodine solution. The iodine coating is non-burning and non-irritating to skin, lip and oral mucosa.
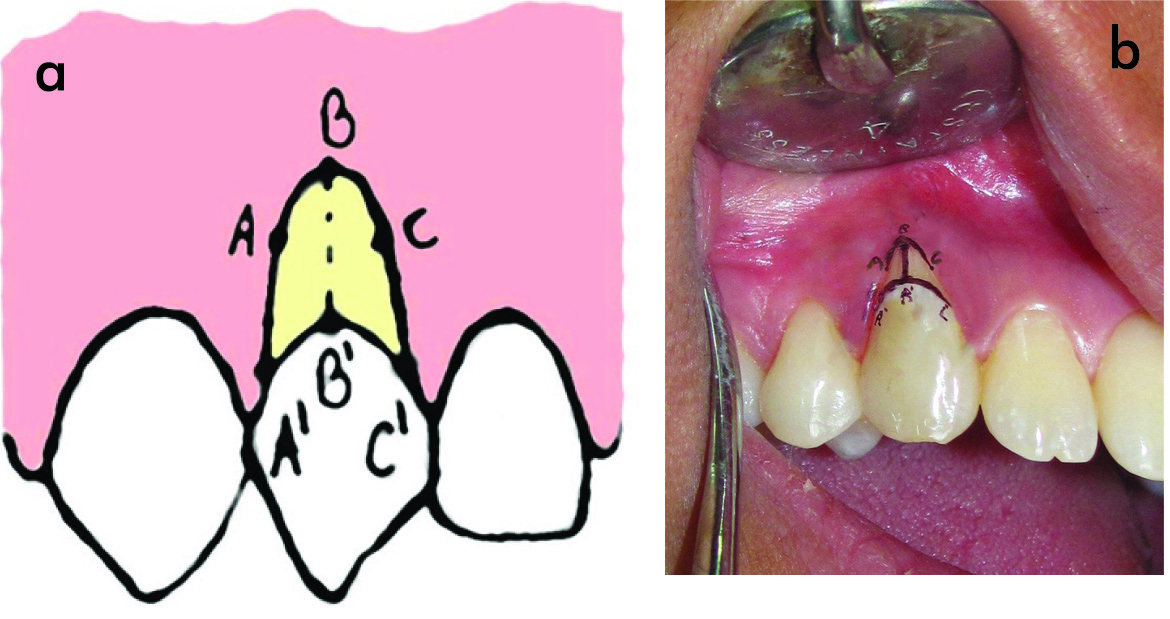
After proper part preparation, right infraorbital and naso-palatine nerves were anaesthetized by 2% lignocaine hydrochloride with 1:80,000 adrenaline. Before surgery, two points located at apical most end of margin of free gingiva and mid-labial CEJ of involved tooth were marked as points B and B’, respectively. The depth of visible gingival recession defect was recorded as a distance from point B to B’ and was denoted as BB’. Furthermore, we assume that BB’ is X mm for further development of incision design. Points A’ and C’ were marked at the junction of CEJ and gingival margin of distal and mesial site, respectively. Additional points, A and C were marked exactly X mm above the points A’ and C’, respectively [Table/Fig-2a,b].
a) Line diagram illustrating three-points A, B and C at the gingival margin; and three-points A’, B’ and C’ at the cementoenamel junction; b) Clinical photograph showing reference markings A, B and C at the gingival margin; and reference markings A’, B’ and C’ at the cementoenamel junction.
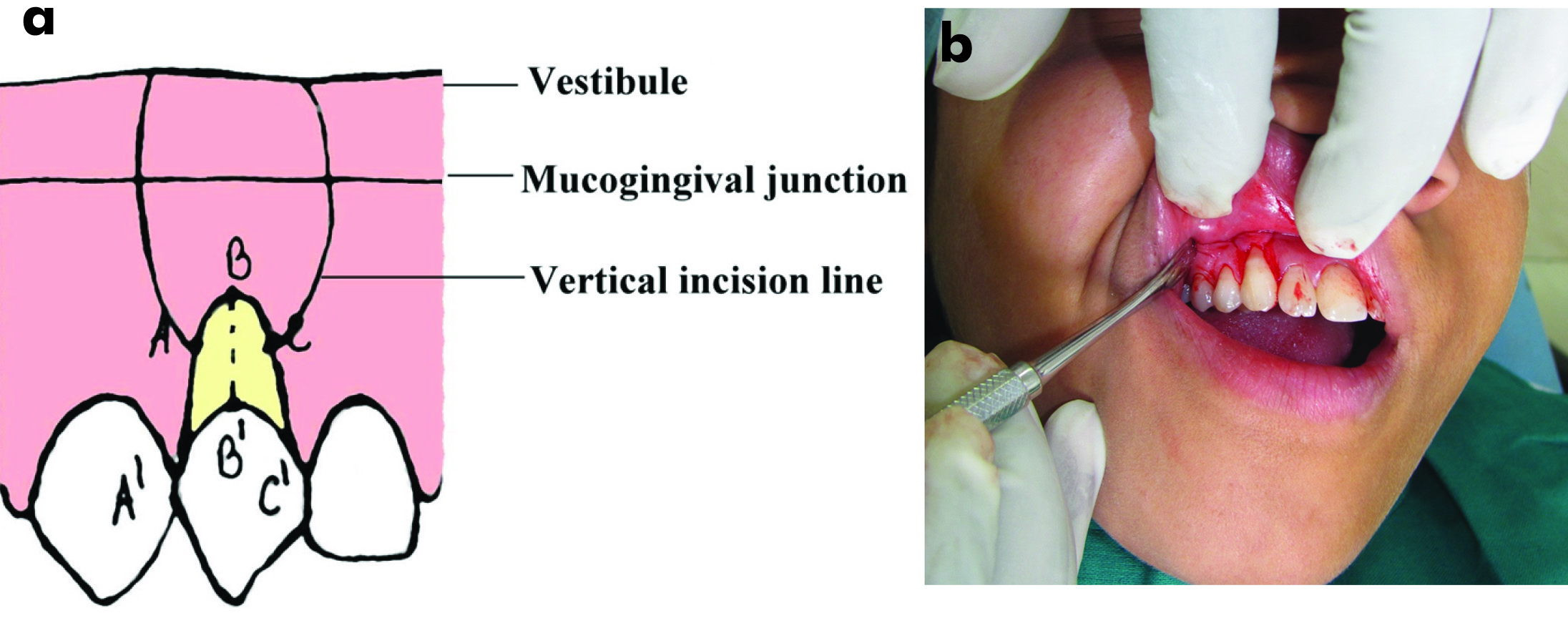
After effectiveness of local anaesthesia, two lateral vertical bevel incisions were made, starting from point A and C, and end into vestibule [Table/Fig-3a,b]. Sulcular incision was given between two vertical incisions. A flap was reflected which was full thickness till mucogingival junction and partial thickness into vestibule. After reflection of the flap, root surface and bone became visible [Table/Fig-4a]. Visible root surface was conditioned with 24% ethylenediaminetetra-acetic acid for three minutes and washed with a normal saline solution for 60 seconds. Conditioned root surface appeared frosted [Table/Fig-4b]. The flap was coronally advanced and approximated at cementoenamel junction by matching points A, B and C on the flap to points A’, B’ and C’ on cementoenamel junction, respectively as defined previously [Table/Fig-4c]; and sutured with 5-0 black silk suture by sling suture technique coronally and interrupted sutures technique proximally [Table/Fig-4d]. The upper lip was manipulated vertically and laterally to ensure that the flap was without tension. Finger pressure was then applied for five minutes on the operated area. No periodontal dressing was applied on surgical area to allow good chemical plaque control by 0.2% chlorhexidine gluconate solution.
a) Line diagram illustrating incision design for point matching technique; b) Clinical photograph showing incision line for point matching technique.
a) After reflection of full-cum-partial thickness flap; b) Frosted appearance of conditioned root surface; c) Flap coronally advanced and approximated at cementoenamel junction. d) Flap sutured by sling suture coronally and interrupted sutures proximally..

Immediately following surgery, use of ice packs was recommended for three hours. Patient was not allowed for brushing to avoid injury and disturbance of healing over the operated area. In case of the pain, the use of Nimesulide (100 mg twice daily) was recommended. A 0.2% chlorhexidine gluconate solution rinse was prescribed four times for one minute daily for the first 10 days [2].
The sutures were removed after 10 days. The patient was instructed to clean the surgical site with a cotton pellet soaked in a 0.2% chlorhexidine gluconate solution four times daily for 10 days. Patient was allowed for manual tooth brushing after three weeks of surgery over the operated site by using soft bristles toothbrush and rolling stroke technique [2].
Patient was recalled once a month up to one year. At each visit, scaling and reminder of oral hygiene instructions were done.
Healing was uneventful. Patient reported no clinical complications or delayed healing and only minimal amount of pain and discomfort. At the end of one year, 3.5 mm that is, 100% root coverage, 5.0 mm of gingival height and 1.0 mm of probing depth were obtained [Table/Fig-5].
At the end of one year, showing complete root coverage.

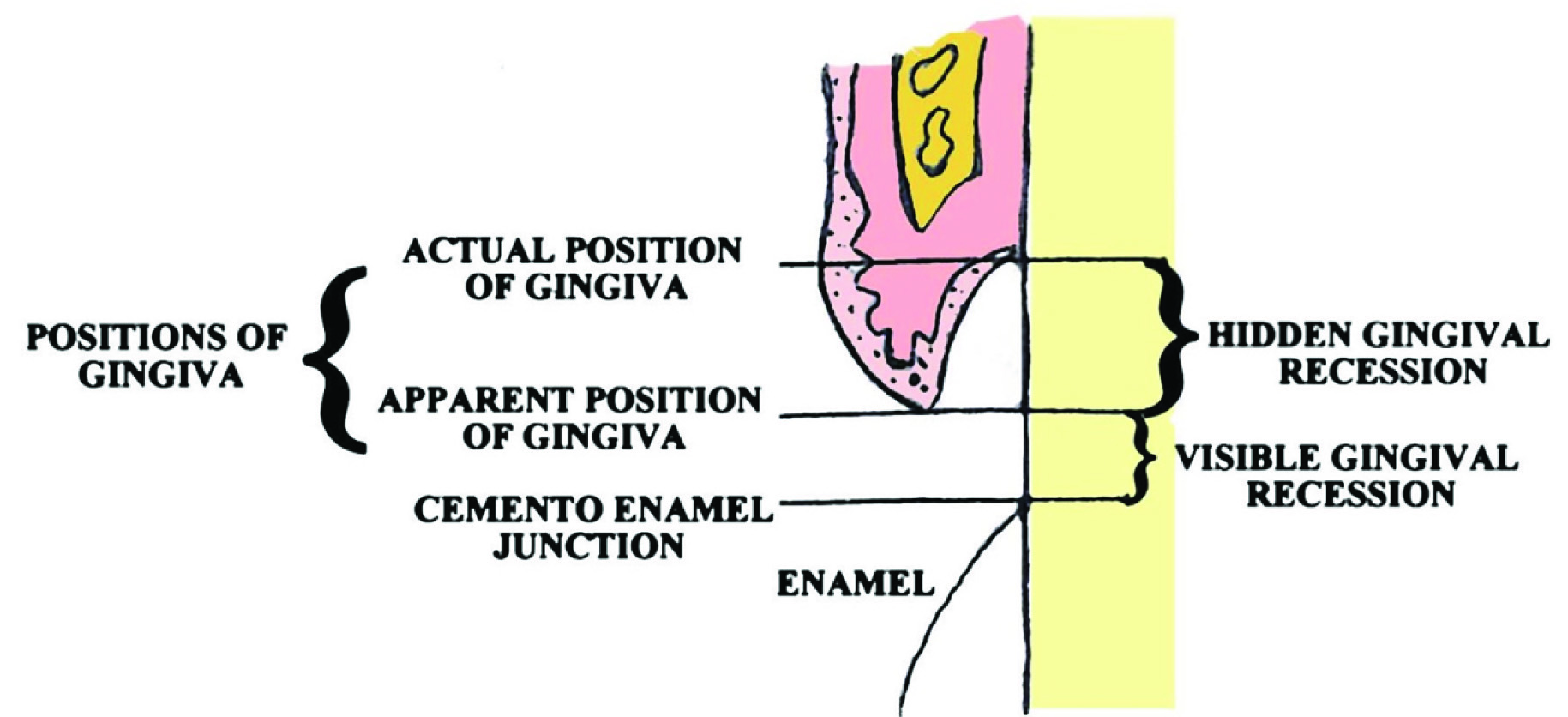
Line diagram illustrating apparent and actual positions of gingiva; and visible and hidden gingival recessions.
Discussion
The goal of any therapeutic intervention aimed at root coverage should be to restore the tissue margin at the CEJ and to achieve an attachment of tissues to the root surface so that a normal healthy gingival sulcus with no bleeding on probing and a minimal probing depth are present [3].
The gingiva is attached to the tooth at the CEJ in adult, with healthy periodontium. When the attachment is apical to the CEJ, the condition is termed gingival recession. Recession, therefore, is the exposure of the root surface by an apical shift in the position of the gingiva. In periodontitis, with the destruction of the periodontal attachment, the junctional epithelium migrates apically on to the root surface. A portion of the exposed root surface may be covered by the lateral wall of the pocket. As a result, gingiva has actual and apparent positions. Actual position of the gingiva is the level of coronal most layer of junctional epithelial attachment and apparent position of gingiva is the level of the crest of the marginal gingiva. Gingival recession, therefore, may be visible gingival recession or hidden gingival recession. Visible gingival recession is the distance from CEJ to the gingival margin while the hidden gingival recession is the distance from the gingival margin to the epithelial attachment [Table/Fig-6]. The exposed root surface may be extremely sensitive, susceptible to cemental caries and aesthetically unacceptable. Visible gingival recession is aesthetically more important than hidden gingival recession [4].
Now days, a number of surgical approaches available for root coverage are pedicle grafts, free grafts and regeneration by regenerative materials and barrier membranes. Regeneration is only possible, when all protocols of regeneration are properly followed by patient and operator. If there is any break in protocols of regeneration, regeneration is not possible. Free grafts are successful if the grafted tissue survives on the exposed root surface. The survival of grafted tissues is critical on avascular root surface [5]. The surgical executions of pedicle soft grafts require a number of surgical incisions and displacement. The surgical incisions could impair blood supply to the flap, and displacement of the flap could stretch the residual vessels [5]. A new predictable and less traumatic root coverage technique, the point matching technique was design.
The concept of the incision design in point matching technique is remarkably simple. The technique, in principle, is a straight forward mathematical matching of a set of three points A, B and C to a second set of points A’, B’ and C’, respectively [Table/Fig-2a,b]. The distance between each matched set of points AA’, BB’ and CC’ is designed to be equal (AA’=BB’=CC’=X as marked in [Table/Fig-2a,b]). This warrants no tension after displacement of the flap, which keeps the main blood supply directed caudo-cranially from the vestibule, flowing throughout entire flap [5]. A statistical analysis performed by Pini-Prato et al., concluded that the higher the flap tension, the lower the recession reduction. They also showed that minimal flap tension does not influence recession reduction after three months when shallow recessions were treated by means of coronally advanced flap procedures [5,6].
Another significance predictor of the clinical outcome of root coverage and recession reduction treated with the coronally positioned flap procedure is the flap thickness. There was direct relationship between flap thickness and recession reduction [2]. For the point matching technique, a full-thickness flap was raised till mucogingival junction and then partial-thickness flap into the vestibule to fulfill the requirements of creating a flap which have maximum thickness that lies on receded root area, but having no tension on apical end. The accurate measurements and matching of reference points are hallmark for success of this technique.
Chen et al., reported a three-point-translation technique with enamel matrix derivative as a means for achieving predictable root coverage. The technique involved a unique flap design and protocol as well as the use of a bone replacement graft over the exposed root surface. They obtained 100% root coverage at six months with excellent color match [5]. In Chen et al., three-point-translation technique, the recession depth was recorded as the distance between alveolar crest and mid-buccal CEJ while in the present study; the recession depth was recorded as the distance between apical most margin of free gingiva and mid-labial CEJ. Thus, measuring the recession depth as in this technique is easier than the Chen et al., technique.
This technique is different from coronally advanced flap technique in vertical incision line. In coronally advanced flap technique, vertical incision lines start from line angles of the tooth where as in this technique; vertical incision lines start from fixed points which are determined by measurements. Surgical execution of coronally advanced flap technique involved a number of surgical incisions which could impair blood supply of the flap and affect healing, whereas, this technique is the less traumatic root coverage technique with better healing, as a result, this technique should be preferred over conventional coronally advanced flap technique. Advantages of point matching technique include predictable root coverage, minimal postoperative discomfort and stability of results. Unlike traditional free soft tissue grafting procedures, point matching technique allows periodontists to treat gingival recession without significant discomfort or complications. The disadvantage of this technique is the time taking for measurements, as a result; there may be limited routine clinical implementations.
Indication of point matching technique is the isolated single tooth recession of Miller class I type. Contraindications of this technique include multiple tooth recession and isolated single tooth recession of Miller class II or III types. In this case, we choose point matching technique because of presence of isolated single tooth recession of Miller class I type. Criteria for point matching technique are that the recession did not extend to mucogingival junction and no interproximal bone loss or loss of papillae was present.
The evaluation period use in this case report was one year from last surgical treatment because more than six months is considered adequate to provide soft tissue maturity and stability [7]. In this case report of point matching technique 3.5 mm that is, 100% root coverage was obtained at the end of 1 year. Pini-Prato et al., reported coronally advanced flap procedure for root coverage. They found mean percent root coverage of 89% and 83% following coronally advanced flap along with treatment of root surface by root planing and polishing, respectively [8]. Zucchelli et al., found root coverage of 92% and 97% by coronally advanced flap with and without vertical releasing incisions after one year [9].
This case report study of point matching technique has certain limitations as like in any study. The technique, although simple, is technique sensitive for the operator, especially during the mathematical matching of points at margin of gingiva to points at CEJ.
Conclusion
We concluded that point matching technique might be potentially useful in achieving the goals for root coverage exposed by visible gingival recession in terms of root coverage, gingival height and probing depth. Clearly, long-term and more close follow-up appointments with clinical and histological studies will be required to obtain more information about the point matching technique for root coverage exposed by visible gingival recession.
[1]. Keiser-Nielsen S, Federation Dentaire Internationale. Two-digit system of designation teethInt Dent J 1971 21:104-06. [Google Scholar]
[2]. Baldi C, Pini-Prato G, Pagliaro U, Nieri M, Saletta D, Muzzi L, Coronally advanced flap procedure for root coverage. Is flap thickness a relevant predictor to achieve root coverage? A 19-case seriesJ Periodontol 1999 70:1077-84.10.1902/jop.1999.70.9.107710505811 [Google Scholar] [CrossRef] [PubMed]
[3]. Singh P, Thakral R, Kaur M, Narula T, Combination of platelet rich fibrin membrane with coronally advanced flap in treatment of gingival recession: A case reportInt J Res Health Allied Sci 2016 2:35-39. [Google Scholar]
[4]. Verma BRR, Nayak RP, Gingivitis. In: Clinical Periodontology. Verma BRR, Nayak RP, editors. Revised edition 2005 2005 Arya (Medi) Publishing House India:129-131. [Google Scholar]
[5]. Chen L, Cha J, HO CH, A three-point-translation technique for root coverage with 4-years follow-upDent Today 2002 21:112-15. [Google Scholar]
[6]. Pini-Prato G, Pagliaro U, Baldi C, Nieri M, Saletta D, Cairo F, Coronally advanced flap procedure for root coverage. Flap with tension versus flap without tension: a randomized controlled clinical studyJ Periodontol 2000 71:188-201.10.1902/jop.2000.71.2.18810711609 [Google Scholar] [CrossRef] [PubMed]
[7]. Ozcelik O, Haytac MC, Seydaoglu G, Treatment of multiple gingival recessions using a coronally advanced flap procedure combined with button application: Coronally advanced flap with buttonsJ Clin Periodontol 2011 38:572-80.10.1111/j.1600-051X.2011.01724.x21443557 [Google Scholar] [CrossRef] [PubMed]
[8]. Pini-Prato G, Baldi C, Pagliaro U, Nieri M, Saletta D, Rotundo R, Coronally advanced flap procedure for root coverage. Treatment of root surface: root planing versus polishingJ Periodontol 1999 70:1064-76.10.1902/jop.1999.70.9.106410505810 [Google Scholar] [CrossRef] [PubMed]
[9]. Zucchelli G, Mele M, Mazzotti C, Marzadori M, Montebugnoli L, De Sanctis M, Coronally advanced flap with and without vertical releasing incisions for the treatment of multiple gingival recessions: A comparative controlled randomized clinical trialJ Periodontol 2009 80:1083-94.10.1902/jop.2009.09004119563288 [Google Scholar] [CrossRef] [PubMed]