Precise refractive status measurement plays an important role in schoolchildren vision screening [1]. Moreover, a dependable screening measurement of refractive status in young children can give meaningful data for early intervention and prevention of amblyopia. Currently, a number of objective methods and instruments are available for assessing refractive status, including retinoscopy, Hartmann-Shack sensor, ray tracing method and rotary prism technology [2-4].
The KR-1W wavefront analyser (Topcon Group, Tokyo, Japan) is an optical system combined with wavefront analyser and corneal topographer. Similar to traditional keratometers, the KR-1W wavefront analyser uses a hypothetical refractive index of n=1.3375, which is based on a model of the cornea as a single refracting surface, for the refractive error calculation within the region of interest. It uses a Hartmann-Shack sensor to analyse higher-order aberration in a central 4 mm and 6 mm diameter on the pupil. Moreover, it can provide standard corneal topography with 19 infrared illuminated placido rings on the anterior surface of the cornea. The higher-order aberration and corneal astigmatism measurements generated by the KR-1W have been shown to have good repeatability [5-7].
The KR-8800 auto kerato-refractometer (Topcon Corporation, Tokyo, Japan) uses rotary prism technology to assess ophthalmic refractive status; it measures spherical refractive power, cylindrical refractive power, the direction of the astigmatic axis, corneal curvature, the direction of the principal meridian and the corneal refractory power. Our previous study showed excellent repeatability of this instrument for keratometry measurement [8].
Current literature has not established whether the refractive error values of these two devices are interchangeable, especially for school children. The purpose of this study was to compare the refraction measurements of the KR-1W and KR-8800 instruments in school children age from 8 to 18 years.
Materials and Methods
Study Population
This observational study was performed at the Affiliated Sixth People’s Hospital Shanghai Jiao Tong University (Shanghai, China) between June 2014 to October 2014. The research protocols were approved by the institutional review boards of the Affiliated Sixth People’s Hospital Shanghai Jiao Tong University and carried out in accordance with the tenets of the Declaration of Helsinki. Written informed consent was obtained from each subject after they were given an explanation of the nature of the study. For participants with an age less than 18 years, written informed consent was obtained from their legal guardian.
Based on a previous study, this study included a total of 57 eyes from 57 school children (26 males, 31 females) [9] Eligible subjects had a normal ophthalmic examination that included the following: a best-corrected visual acuity of ≥16/20, normal slit-lamp and fundoscopy examinations, an IOP <21 mmHg. Children with media opacity, amblyopia, squint, or any detectable ocular diseases of decreased vision were excluded. One eye from each subject was randomly selected.
Data Acquisition
The sphere, cylinder power, and cylinder axis were measured on KR-1W and KR-8800 in non-cyclopleged eyes. Each measurement was repeated three times in each eye and the averaged value was used in the final analysis. The software was version 1.06 for KR-1W. The data capture procedure for both devices was as follows: the subject’s chin was placed on the chin rest, the subject’s forehead was pressed against the forehead strap and the subject’s eye was aligned to the visual axis by a central fixation light or target. A single trained operator performed all of the examinations using both instruments following the procedural guidelines with the sequence of KR-8800 and KR-1W with the time interval less than five minutes under no cycloplegic condition.
Vector Analysis of Astigmatism
Vector analysis was used to compare astigmatism values from the two devices [10]. According to the conversion formulas, the astigmatism value was decomposed into two components as follows:
X=A cos (2α); (1A)
Y=A sin (2α) (1B)
Where
X=cardinal component,
Y=oblique component,
A=astigmatism magnitude in diopters,
α=astigmatism axis in degrees
Statistical Analysis
The statistical analyses were performed with commercial software (SPSS version 13.0; SPSS Inc.). The statistical significance of the interdevice differences in refractive error parameters was evaluated with the paired two-tailed t-test. The correlation coefficient was also calculated, and a scatter plot was created to evaluate the relationship among the refractive error values, age and gender. Interdevice agreement was evaluated using Bland-Altman analysis [7]. The interdevice differences were plotted against their means, and the 95% LoA were determined using this method. The significance level for all of the tests was set at p-value=0.05.
Results
The mean age of all the enrolled subjects was 12±3 years (range, 8-18 years). [Table/Fig-1] shows the mean spherical power, astigmatism magnitude, astigmatism cardinal and astigmatism oblique values for each instrument.
Summary of refractive error measurement and mean inter-device difference between KR-8800 and KR-1W
| KR-8800 | KR-1W | KR-8800-KR-1W | p* |
|---|
| Sphere (D) | -2.26±2.24 | -2.11±2.28 | -0.16±0.51 | 0.024 |
| Astigmatism Magnitude (D) | -0.63±0.50 | -0.73±0.52 | 0.11±0.32 | 0.014 |
| Astigmatism Cardinal | -0.48±0.54 | -0.58±0.61 | 0.09±0.29 | 0.017 |
| Astigmatism Oblique | 0.09±0.34 | 0.04±0.32 | 0.05±0.19 | 0.036 |
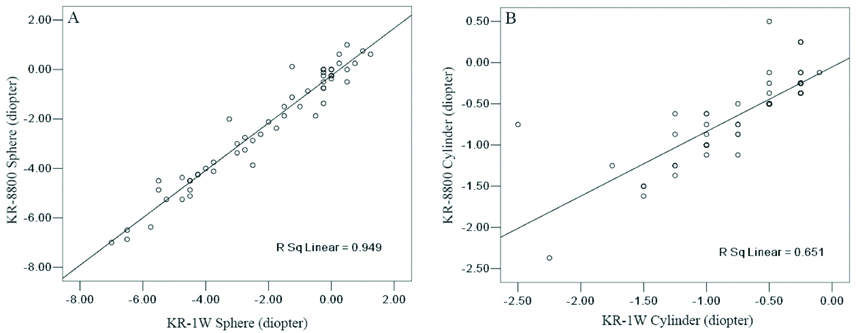
The spherical power values measured by the KR-8800 were significantly more negative than those of the KR-1W (p=0.024). The cylinder power values measured by the KR-8800 were significantly more positive than those of the KR-1W (p=0.014). Moreover, KR-8800 and KR-1W were significantly different in astigmatism measurements using vector analysis [Table/Fig-2]. However, there was a significant linear correlation between the KR-8800 and KR-1W instruments for the spherical error (r=0.974, p<0.0001) [Table/Fig-3a], cylinder power (r=0.807, p<0.0001) [Table/Fig-3b].
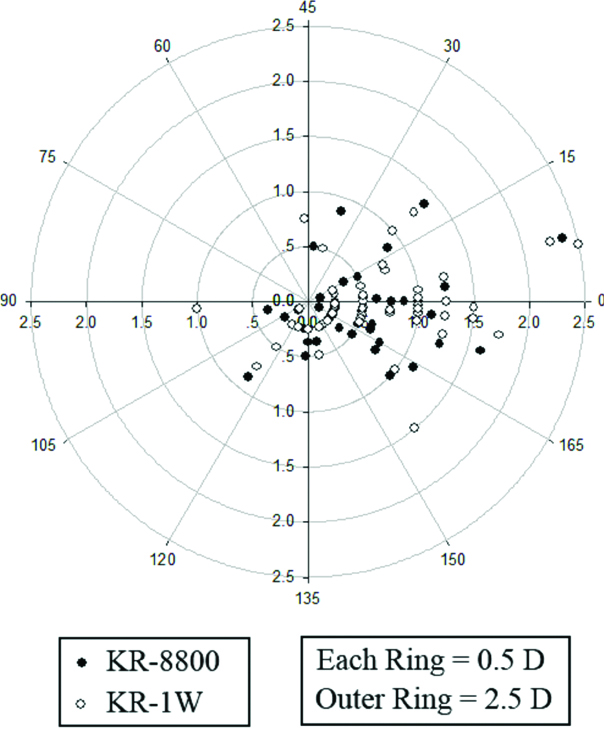
Double-angle plot of negative astigmatism in the KR-8800 and KR-1W group. The astigmatism magnitude was lower in KR-8800 compared to KR-1W by 0.11 D (p=0.014).
There was a significant linear correlation between spherical power measurements by KR-1W and KR-8800 (A: r=0.974, p< 0.0001). The best-fit line (y=-0.25+0.96x) is designated by the solid line; there was a significant linear correlation between cylinder power measurements by KR-1W and KR-8800 (B: r=0.807, p<0.0001). The best-fit line (y=-0.05+0.78x) is designated by the solid line.
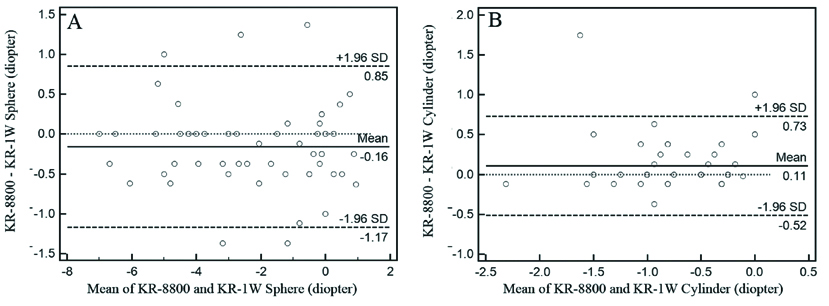
Bland-Altman plots were created to evaluate the differences in the individual measurements as a function of the mean of the two instruments for each subject. Both methods showed good agreement for the spherical and cylinder power values that were measured with mean of differences centering around zero [Table/Fig-4]. The interdevice 95% LoA range for the spherical and cylinder power were 2.02 D and 1.25 D, respectively. The difference in the cylinder power values between the two instruments showed the smallest range of variation [Table/Fig-4b].
Differences in mean spherical power (A) and cylinder power (B) values between KR-8800 and KR-1W. The means and means±standard deviation (SD) are indicated.
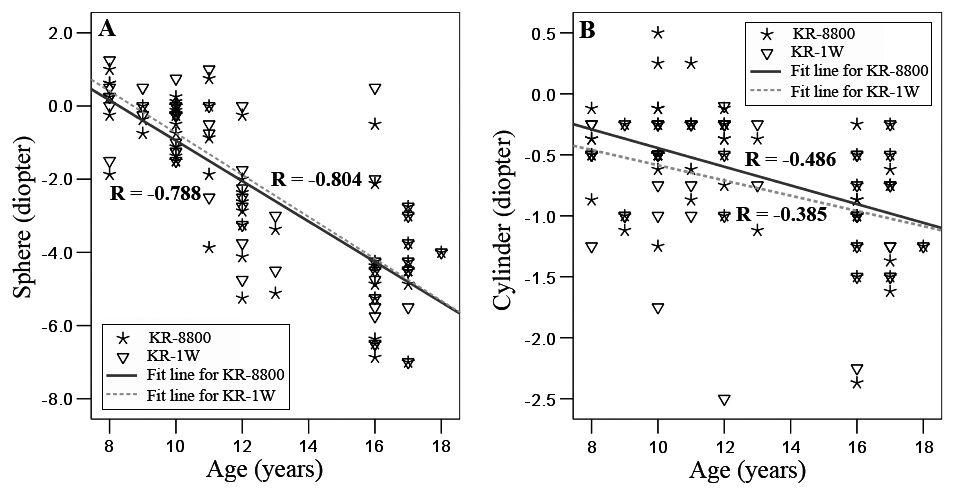
A Pearson correlation analysis showed that for the two devices, age was negatively correlated with spherical error and cylinder power and the spherical error showed much more negative correlation values than cylinder power [Table/Fig-5]. On the contrary, gender showed no significant correlations with neither spherical error nor cylinder power of both instruments (For KR-8800: sphere: r=-0.016, p=0.904; cylinder: r=-0.115, p=0.396; For KR-1W: sphere: r=-0.062, p=0.646; cylinder: r=-0.102, p=0.450).
Plots of spherical error versus age (A) and cylinder power versus age (B) for both KR-8800 and KR-1W devices. For the KR-8800 instrument, age was negatively related with the spherical error and cylinder power (r=-0.788, p<0.001; r=-0.486, p<0.001). In the KR-1W group, age was also negatively correlated with the spherical error and cylinder power (r=-0.804, p<0.001; r=-0.385, p=0.003).
Discussion
The accurate measurement of refractive status is not only an important factor in the diagnosis and follow-up of myopia but is also crucial in the determination of the level of correction that can safely be performed during refractive surgery. As a routine examination device for refractive status measurement, the auto kerato-refractometer has been widely used worldwide. As a device for wavefront analysis, the KR-1W integrated the Hartmann-Shack and Placido-disk topography system, allowing the keratometry, autorefraction as well as the pupillometry to be analysed in a single measurement. It is essential to investigate the inter-device interchangeability in clinical application. This study investigated the comparability of refractive status measurements between KR-8800 and KR-1W in schoolchildren. The results of the present study show statistical refractive status measurement differences including the spherical power and astigmatism between the KR-8800 and KR-1W. However, these differences are small and not clinically meaningful. Moreover, age showed statistically negative correlations with both spherical and cylinder power in this population.
In the current study population, the KR-1W wavefront analyser demonstrated slightly less mean spherical error (by 0.16 D) compared to the KR-8800 automatic refractometer, which shows similar changing tendency as McCullough SJ et al., study of the refractive error measurements comparison between IRX3 abberrometer and autorefractor in school-aged children [11]. The more hyperopic spherical error in KR-1W is unexpected because that wavefront analysers have been demonstrated to produce device myopia even in the cycloplegic condition owing to their measurements including much more peripheral optic area compared to the automatic refraction, which mainly considers the central area of the pupil [12,13]. However, the time interval in the testing sequence between the two devices and the different methods to relax accommodation for autorefractometer and wavefront analyser in the measurements may attribute to this difference [11].
Different from previous refractive error measuring studies in adult and children using Shin-Nippon autorefractor, the KR-8800 slightly underestimated cylinder power about 0.11D relative to the KR-1W in our younger population in the present study [11,14]. This may be because the KR-8800 is a closed-field autorefractor, which is different from the open-field Shin-Nippon autorefractor. Compared to closed-field devices, Open-field autorefractor can provide more naturalistic viewing condition, which is beneficial to relax accommodation. However, maintaining steady and accurate fixation is much more important for precisely measuring refractive status, especially for astigmatism in clinical application [11].
Similar to previous population-based studies about refractive errors of school-age children in China, age was significantly negative correlated with myopic spherical refractive error for both devices in present research [15,16]. Moreover, we demonstrated the statistical negative correlation between age and cylinder power for school children, which may partially be consistent with the age-related changing of corneal astigmatism studied by Ho JD et al., [17]. These changing tendencies may partially attribute to the studying pressure, longer daily reading and studying duration and less physical activities, which has been confirmed by previous researches in China [15,18].
Limitation
First, subjects were asked to fixate on the internal fixation target during the measurement of refractive status with both devices, but potential slight misalignments of fixation target may result in slight overestimation or underestimation of the refractive error measurements. Therefore, the experienced examiner encouraged steady fixation during examination and measurements were repeated if the operator found alignment was poor to eliminate the potential influencing of misalignment. Second, Autorefraction was considered as the gold standard in the present study to compare with the refractive error measurements from KR-1W. For refractive status evaluation, subjective measurements of astigmatism are considered to be more accurate than objective refraction, especially for school-age children [19]. Hence, a further study of KR-1W wavefront analyser compared to subjective refraction would be much more valuable. Third, the sequence of measured devices may cause refractive error differences due to accommodation fluctuation under noncycloplegic condition [20,21]. Therefore, a further study of refractive error comparison using of cycloplegic is needed.
Conclusion
In conclusion, this comparative study showed that the spherical power and astigmatism were statistically different between the KR-1W wavefront analyser and KR-8800 automatic refractometer. However, the measurements of the two instruments showed significant linear correlation to each other.
Compliance with ethical standards
Funding: This work was supported by the National Natural Science Foundation of China under Grant No. 81501544.
Conflict of interest: The authors declare that they have no conflict of interest regarding the publication of this paper.
Ethics approval and consent to participate Written informed consent was obtained from each subject. For participants with an age less than 18 years, written informed consent was obtained from their legal guardian. The research protocols were approved by the institutional review boards of the Affiliated Sixth People’s Hospital Shanghai Jiao Tong University and carried out in accordance with the tenets of the Declaration of Helsinki.